-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Journal of Health Science
p-ISSN: 2166-5966 e-ISSN: 2166-5990
2022; 12(1): 14-22
doi:10.5923/j.health.20221201.03
Received: Feb. 10, 2022; Accepted: Feb. 18, 2022; Published: Mar. 15, 2022

Knowledge of Some Nigerian University Students about COVID-19 Pandemic
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAdedamola Olutoyin Onyeaso1, Chikamaram O. Okino2, Chukwudi O. Onyeaso3
1Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Port Harcourt, Rivers State, Nigeria
2Department of Oral Pathology and Medicine, University of Port Harcourt Teaching Hospital (UPTH), Port Harcourt, Rivers State, Nigeria
3Department of Child Dental Health, Faculty of Dentistry, College of Health Sciences, University of Port Harcourt / University of Port Harcourt Teaching Hospital (UPTH), Port Harcourt, Rivers State, Nigeria
Correspondence to: Adedamola Olutoyin Onyeaso, Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Port Harcourt, Rivers State, Nigeria.
| Email: |  |
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Introduction: Considering the enormous impact of the highly infectious COVID-19 Pandemic on human existence and the place of the knowledge of this disease for its effective control, as well as the important role of health educators in this aspect, this study aimed at assessing the knowledge of COVID-19 Pandemic of some undergraduate students of Human Kinetics and Health Education in Nigeria, who are student-teachers and health educators. Materials and Methods: A self-administered questionnaire survey of 223 students and 202 of them – 64(31.7%) males and 138 (68.3%) females, correctly filled and returned the questionnaire. Using the SPSS, the data was analysed descriptively and the paired samples t-test used to test the hypotheses with significance level set at P<0.05. Results: On average, 62.6% of the participants had good knowledge of the signs and symptoms of COVID-19 Pandemic, while 74.9% had good knowledge of the transmission of the disease. The participants significantly had good knowledge of COVID-19 Pandemic (P<0.05), while the female gender significantly had better COVID-19 Pandemic knowledge (P<0.05). Conclusion/Recommendation: The participants significantly have good knowledge of COVID-19 Pandemic with the female gender significantly having better knowledge. A national survey would be worthwhile involving more variables such as the omicron variant, socio-economic status, educational level, vaccines and age influence for purposes of health education and promotion.
Keywords: COVID-19 Pandemic, Knowledge, Health Education, Students, Gender, Nigeria
Cite this paper: Adedamola Olutoyin Onyeaso, Chikamaram O. Okino, Chukwudi O. Onyeaso, Knowledge of Some Nigerian University Students about COVID-19 Pandemic, Journal of Health Science, Vol. 12 No. 1, 2022, pp. 14-22. doi: 10.5923/j.health.20221201.03.
Article Outline
1. Introduction
- The Coronavirus Disease 2019 (COVID-19) has caused many problems globally virtually in every aspect of human life activities such as disruptions in education, movement of people, goods and services, healthcare systems and the economy. Despite the efforts of international health agencies like World Health Organization (WHO), Centre for Disease Control (CDC) to educate and the masses on the signs and symptoms of the disease and the necessary preventive measures to reduce the infection rates across nations of the world, the disease has spread so much that currently the second wave is still on in many countries, even as omicron variant has added to the anxiety associated with this Pandemic..According to the meta-analysis study and the follow up by Struyf et al [1,2], the signs and symptoms of the COVID-19 could be grouped into systemic, respiratory, gastrointestinal and cardiovascular. According to that meta-analysis, the studies gave signs and symptoms with low sensitivity and high specificity with only six symptoms having sensitivity of at least 50% in at least one study - cough, sore throat, fever, myalgia or arthralgia, fatigue, and headache. The reports [1,2] further stated that of those, fever, myalgia or arthralgia, fatigue, and headache could be considered red flags for COVID-19 as their specificity was above 90%, meaning that they substantially increase the likelihood of COVID-19 disease when present. In a meta-analysis of 38 studies involving 3062 COVID-19 patients [3], the most commonly experienced symptoms of COVID-19 patients were fever, fatigue, cough and expectoration. A relatively small percentage of patients were asymptomatic. Most patients showed normal leucocytes counts, lymphopenia, elevated levels of C-reactive protein and ESR, while bilateral lungs involvement was common. Neurological and neuropsychiatric manifestations of COVID-19 have been documented with clinical features of both central and peripheral nervous system involvement very evident [4]. According to Roy et al [4], most of the psychological effects are secondary to pandemic-associated regulatory, socioeconomic and psychosocial changes, and they opined that this demands a wide index of suspicion for prompt diagnosis of SARS-CoV-2 to prevent further complications and mortality. Zahra et al [5] stated that the presence of olfactory and taste dysfunction (OTD) could potentially be used as a screening tool for COVID-19, especially in young and female patients. They [5] suggested that further research would be required to establish the true diagnostic value of these symptoms and efficacy as screening tools for COVID-19 patients due to limited literature on the association between OTD and COVID-19.Meanwhile, in a more recent study by Mehraeen et al [6], the results supported recent reports that SARS-CoV-2 may infect oral and nasal tissues and cause olfactory and gustatory dysfunctions. These findings may aid future research on the diagnosis, prevention, and treatment of COVID-19 consequences. Poncet-Megemont [7] highlighted the high prevalence of new headaches during COVID-19 infection in French patients, and recommended further studies for more detailed characterization of patients with COVID-19-associated headaches. Eighty-two (59%) of their sample reported new headaches during the acute phase and 3.6% had persistent headaches 1 month after fever and dyspnoea remission. According to the report, anosmia and ageusia were also very common, occurring in 60.4% and 58.3% of the patients, respectively. The study further stated that both anosmia and ageusia persisted in 14.4% and 11.5% of COVID-19 patients 1 month after recovery. According to that brief communication [6], headaches were neither clearly associated with anosmia, nor with ageusia, and were not associated with disease severity.The results of the study by Huart et al [8] suggested that mechanisms of COVID-19 related olfactory dysfunction are different from those seen in an acute cold (AC) and may reflect, at least to some extent, a specific involvement at the level of central nervous system in some COVID-19 patients.Huang et al [9] reported that even 6 months post acute infection; COVID-19 survivors were mainly troubled with fatigue or muscle weakness, sleep difficulties, and anxiety or depression. Although it is generally believed that the signs and symptoms of COVID-19 are not easily observed in children, there are reports that in communities with high rates of the COVID-19, some children have been observed with unusual syndrome of fever and inflammation. Whittaker et al [10] reported that 58 children met with the criteria for Pediatric Inflammatory Multisystem Syndrome Temporally Associated with SARS - COV-2 (PIMS-TS) with a wide spectrum of presenting signs and symptoms and disease severity, ranging from fever and inflammation to myocardial injury, shock, and development of coronary artery aneurysms. According to Gul [11], skin lesions could be related to personal protective equipment and personal hygiene measures, skin findings observed in SARS-CoV-2 virus infections and skin findings due to COVID-19 treatment agents. The meta-analysis revealed that incidence of skin lesions due to COVID-19 was reported to be between 0.2% and 29%. The study further stated that many skin lesions including maculopapular, urticarial, vesicular, chilblain-like, thrombotic/ischemic, etc. are observed in COVID-19 patients while some authors have stated that there is an absence of SARS-CoV-2 virus infection-specific skin findings. However, in asymptomatic or pre-symptomatic COVID-19 patients in particular, skin lesions can lead to the diagnosis of COVID-19. Meanwhile, the diagnosis and prevention measures for asymptomatic cases remain a challenge, and the specific characteristics of asymptomatic infections need to be further clarified [12].University undergraduate students, especially those studying health related subjects, like those in Human Kinetics and Health Education Department, are expected to pay attention to the signs and symptoms of this devastating COVID-19 pandemic so as to, at least, be able to educate others for preventive and early presentation for testing purposes. This study aimed at assessing the level of knowledge about COVID-19 pandemic by the undergraduate students of Human Kinetics and Health Education, Faculty of Education of the University of Port Harcourt, Rivers State, Nigeria.
2. Materials and Methods
2.1. Study Design
- A cross-sectional self-administered questionnaire study was used.
2.2. Population of Study
- 223 copies of a self-administered questionnaire containing some questions to assess their general knowledge and signs and symptoms of COVID-19 Pandemic as shown in the attached Appendix were distributed to some undergraduate students of the Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Rivers State, Nigeria. Twenty one (21) copies of the questionnaire were removed because of poor filling of the forms, giving the final study sample of two hundred and two (202) students. The final study population consisted of 64(31.7%) males and 138(68.3%) females with mean age of 22.09 ± 2.42 (SD) years and age range of 18 to 32 years.The following null hypotheses were generated and tested:Ho1: The general knowledge of COVID-19 pandemic by the participants would not be statistically significant.Ho2: There would be no statistically significant gender difference in their knowledge of COVID-19 Pandemic.
2.3. Categorization of the Participants’ Responses
- The responses of the participants were categorized into ‘correct’ and ‘incorrect’ responses based on whether they ticked the correct option or incorrect option. The correct responses were weighted 2 while the incorrect responses had 1 for purposes of further statistical analyses. The questions are shown in the attached Appendix (Questionnaire).
2.4. Statistical Analysis
- The Statistical Package for Social Sciences (SPSS) was used to analyse the data. Both descriptive statistics and paired samples T- tests were used to analyse and test the hypotheses, while the significance level was set at P<0.05.
2.5. Ethical Approval and Participants Consent for the Study
- Approval from the University was not considered necessary because the survey was very relevant to the curriculum of study of the participants. In addition, this survey is completely non-invasive.
3. Results
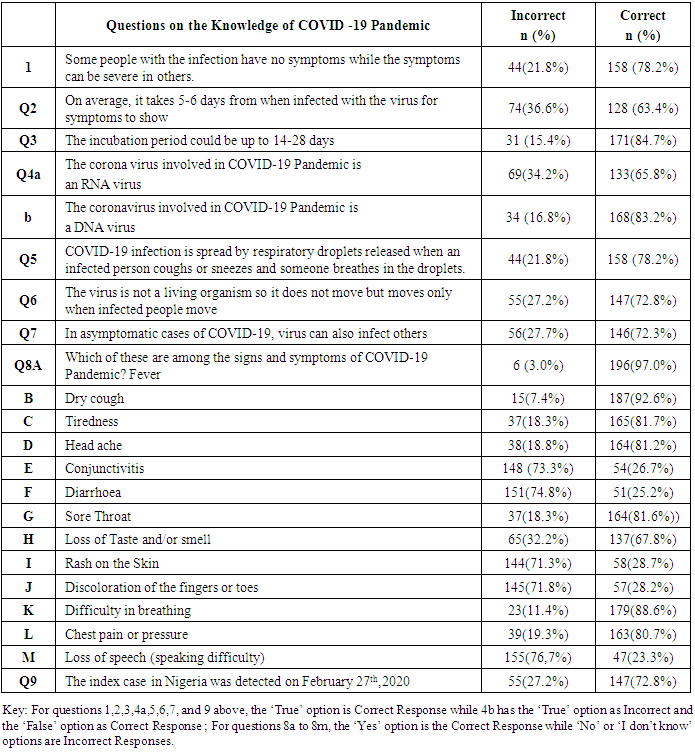
- On average, 62.6% of the participants had good knowledge of signs and symptoms of COVID-19 while 74.9% had good knowledge of the transmission of the disease. The mean score for positive (correctly answered questions) responses by the participants was 135.36 ± 48.31 (SD) while the mean score for negative (incorrectly answered questions) responses came to 66.59 ± 48.34 (SD).
|
|

|
|

4. Discussion
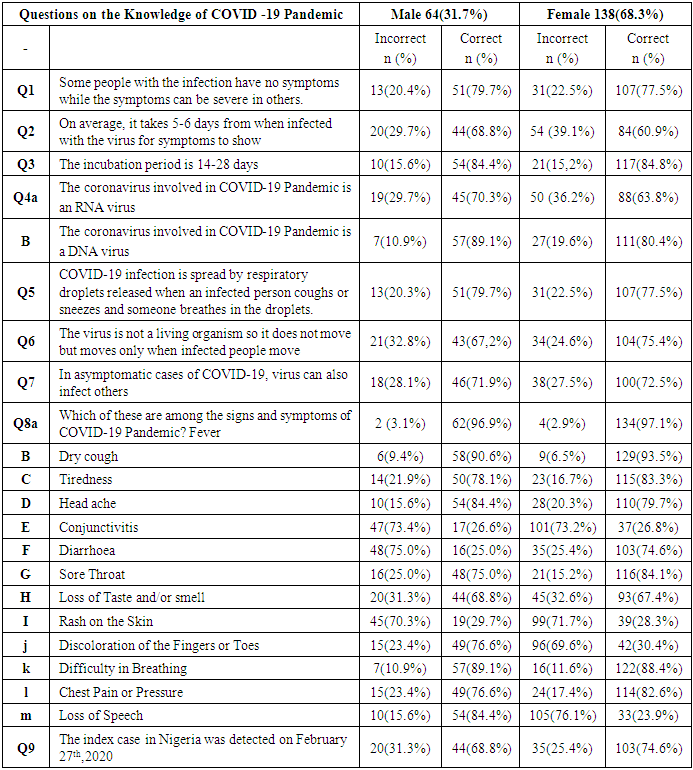
- This present Nigerian study that assessed the general knowledge of COVID-19 by some undergraduate students of Human kinetics and Health Education has shown that significant proportion of them had good knowledge of COVID-19 pandemic, while the female students significantly knew better than their male counterparts. An earlier related study from Nigeria concluded that their results showed that healthcare workers (HCWs) in Nigeria had excellent knowledge of the COVID-19 outbreak [13]. Their study [13] was among practising healthcare workers on the field while the current Nigerian study was among University students hoping to be the future teachers and health educators in Nigeria.The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has become a major concern for the people and governments across the world due to its impact on individuals, as well as on public health. The infectiousness and the quick spread across the world make it an important event in everyone's life, often evoking fear [13]. In India, according to Parikh et al [14], almost 98% of healthcare professionals and 97% of the general public, respectively, identified difficulty in breathing as the main symptom. This Nigerian study revealed that 88.6% of the participants were able to note that difficulty in breathing is a major symptom of this highly infectious disease. Their conclusion that most healthcare professionals and the general public that they surveyed were well informed about SARS-CoV-2 could be said to apply to these healthcare-related participants in Nigeria. In another related survey in Mumbai [15], the overall awareness for all subgroups was adequate with 71.2% reporting correct answers, while the highest percentage of correct responses came from undergraduate medical students and the lowest was from non-clinical/administrative staff. In Ghana, Hasford et al [16] concluded that some aspects of the awareness of radiation medicine professionals on COVID-19 pandemic were adequate and others needed critical improvement to help reduce spread of the disease. Al-Rasheedi et al [17] reported that the general public and health care professionals from Qassim Region showed adequate awareness of COVID-19. However, they recommended that there was a strong need to implement periodic educational interventions and training programs on infection control practices for COVID-19 across all healthcare professions. In a similar study to the current Nigerian study, Zhang et al [18] reported that the result of their study revealed suboptimal COVID-19-related knowledge, attitude and practice among healthcare students in China, and concluded that to effectively control future outbreaks of COVID-19, there is a need to implement public sensitization programs to improve the understanding of COVID-19 and address COVID-19-related myths and misconceptions, especially among healthcare students. Naveed and Shaukat [19], in an online questionnaire-based study, had it that health literacy of university students positively predicted their Covid-19 awareness and protective behaviours indicating that students with high health literacy were likely to be more aware of COVID-19 and adopt health protective behaviours. They [19] also observed gender and rural/urban differences. Their [19] conclusion was that the results demonstrated an urgent need for planning a needs-based health literacy programme focusing specifically on Covid-19 literacy in Pakistan.In another online survey of University students in Pakistan, Faisal et al [20] reported that most of the students had an adequate level of knowledge and were doing better preventive measures against COVID-19 but that health education initiatives were required to ensure best practice among the high-risk groups. According to their report [20], 95.8% of the participants knew about the signs and symptoms of COVID-19 infection and 83% knew about its transmission while the present Nigerian study revealed 62.6% and 74.9%, respectively. The much better knowledge of the Pakistan University students of COVID-19 Pandemic over Nigerian students could be attributed to attitudinal and behavioural differences of the citizens in the two countries because both countries put in place impressive control measures Other recent studies [21,22] from Pakistan agree that the majority of the University students and people of Pakistan have demonstrated overall adequate knowledge of COVID-19 and good perception towards the pandemic. In addition, Afzal et al [23] showed that the knowledge of COVID-19 among the Pakistanis in community was positively correlated with attitude and practices whereas negatively correlated with risk factors. In Veitnam, it was reported that face mask use knowledge was statistically associated with COVID-19 knowledge [24]. Clavel et al [25], in their review work, reported that the level of knowledge of COVID-19 was moderate to high in both general and high-risk adult populations, among other variables reviewed.. Wake [26], in a review work, stated that the majority of the studies reflected a good knowledge, positive attitude, and good practice towards COVID-19 respective to their countries, while some studies identified factors associated with knowledge, attitude, and practice regarding COVID-19. For instance, age, educational level, residence, monthly income, profession, gender, marital status, and news media were factors significantly associated with knowledge [26]. The present Nigerian study also revealed a significant gender association with COVID-19 knowledge of the participants with the female gender significantly having better knowledge. The participants are students (youths) in close age bracket which did not necessitate assessing any age association with their knowledge of COVID-19 Pandemic. Haftom et al [27] reported that knowledge score was statistically significantly associated with gender, age, and educational status of the study participants, whereas attitude and practices were significantly associated with educational status and knowledge of participants in Ethiopia. Among the Sudanese population, Sayedahmed et al [28] reported that their participants had good knowledge, and positive attitude toward the COVID-19, and their findings further revealed that education was positively associated with knowledge, and good level of knowledge was associated with good practice toward COVID-19. As already known, the participants in this Nigerian study are of the same educational status.In a study among the undergraduate and postgraduate students at the University of Jordan, Sallam et al [29] found that the false belief that COVID-19 was the result of a global conspiracy could be the consequence of a lower level of knowledge about the virus and could lead to a higher level of anxiety, which should be considered in the awareness tools of various media platforms about the current pandemic. In a related study [30], a negative correlation between the knowledge about the COVID-19 pandemic and the severity of psychopathological symptoms was observed. The study [30] further stated that the results clearly indicated that the complexity of the global problem of the current pandemic was related to the development of psychopathological symptoms, and recommended the need for longitudinal studies to identify the direction of causality.According to Middleton et al [31], amongst their study participants, 68.8% responded correctly to at least 60% of knowledge-related questions. Misconceptions were identified in 30%. Only 29.1% expressed a positive attitude toward a hypothetical person with COVID-19 without projecting judgment (9.2%) or blame (38%). Odds of expressing a positive attitude increased by 18% (95% CI 13-24%; p < 0.001) per unit increase in knowledge. Postgraduate level education was predictive of better knowledge (odds ratio (OR) 1.81; 95% CI 1.34-2.46; p < 0.001 among doctoral students] and positive attitude [OR 1.35; 95% CI 1.01-1.80; p = 0.04). The study concluded that specific knowledge gaps and misconceptions existed among University students about SARS-CoV-2 and COVID-19 and their prevalence was associated with negative attitudes toward people with COVID-19. In another related study among nursing students in Saudi Arabia, Albaqawi et al [32] discovered that being female, being in the fourth year, and gaining good perceived knowledge were associated with high actual COVID-19 knowledge. They observed that University, gender, age, academic level, and perceived COVID-19 knowledge were the associated factors. Stefanowicz-Bielska et al [33], in an electronic survey conducted among students of nursing, midwifery, and emergency medicine during the COVID-19 pandemic, from 8 April 2021 to 6 June 2021 in the Pomeranian Voivodeship, reported that a moderate level of knowledge was found in 88% and high in 11% of students. They found also that midwifery students had a higher level than nursing students (p = 0.002) and students of emergency medicine (p = 0.003), while the female gender was much more afraid of SARS-CoV-2 virus infection.Among Brazilian nursing students, Reis et al [35] reported that the students' knowledge about COVID-19 in general was considered inadequate but had limited knowledge about preventive measures in the hospital environment.
5. Strengths and Limitations of the Study
- Although our sample is a convenient one, the Admission Criteria in Nigerian Federal Universities provide for a fair representation of youths from different parts of the country in each Federal University, and the University of Port Harcourt is a Federal University. This has served as an advantage in automatically helping to have a fairly representative sample when the students are involved in a study like this just like in our earlier works [35,36]. However, caution must be exercised while making a generalization of the findings for the whole country. This study did not have equal number of male and female participants, which is a reflection of the gender distribution among the undergraduate students of Human Kinetics and Health Education and possibly in our environment.
6. Conclusions
- The participants had significantly good knowledge of COVID-19 Pandemic, while the female gender was significantly associated with better knowledge of COVID-19 Pandemic.
7. Recommendations
- It would be worthwhile to carry out a related national survey in Nigeria possibly involving information on socio-economic status of the participants, educational level, vaccine use or otherwise, and possible influence of age on knowledge of the disease and behaviour toward the Pandemic, as well as additional variables like the omicron variant because we are not aware of any of such study so far in the country.
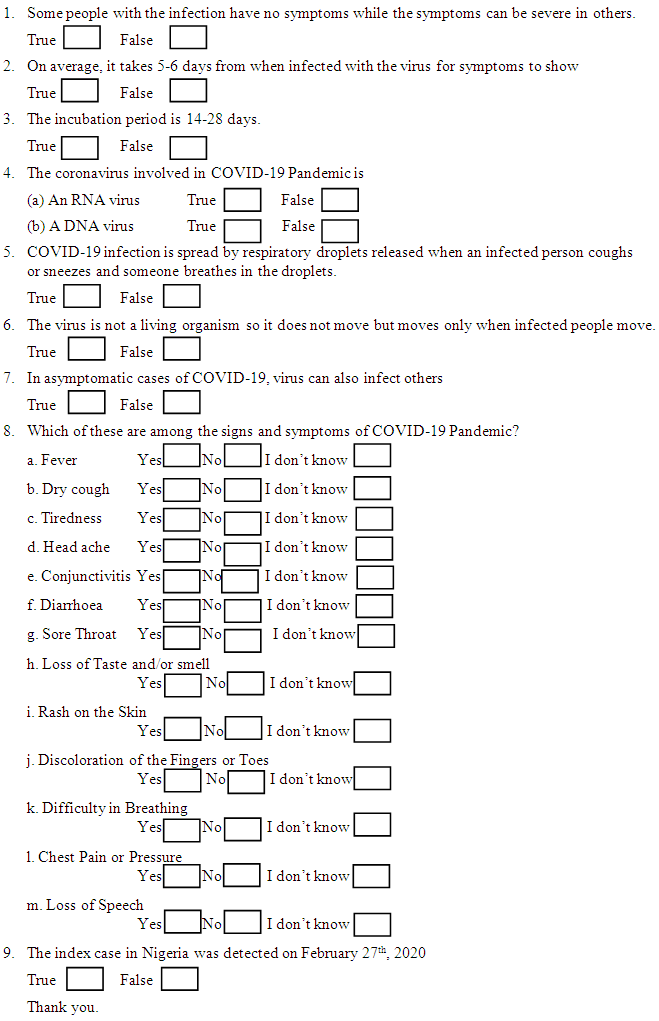
Appendix
- QUESTIONNAIRE ON KNOWLEDGE OF COVID-19 PANDEMICDear Participant,Please, kindly provide your sincere answers to these questions without consulting with anyone else. This is purely for research purposes only. Your confidentiality is guaranteed. Thank you so much. Section Aa. Age: - -- -- - - -- b. Sex: --- --- - -- -- c. Year of Admission / Matriculation Number:------ -- - - - - - - - - - - - -- - - - - - -- - Section B