-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Journal of Health Science
p-ISSN: 2166-5966 e-ISSN: 2166-5990
2022; 12(1): 7-13
doi:10.5923/j.health.20221201.02
Received: Feb. 5, 2022; Accepted: Feb. 18, 2022; Published: Mar. 15, 2022

Knowledge and Attitude of Menstrual Regulation among Ever-Married Women in Bangladesh
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLDhaneswar Chandro Sarkar
Department of Statistics, Mawlana Bhashani Science and Technology University, Tangail, Bangladesh
Correspondence to: Dhaneswar Chandro Sarkar, Department of Statistics, Mawlana Bhashani Science and Technology University, Tangail, Bangladesh.
| Email: |  |
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

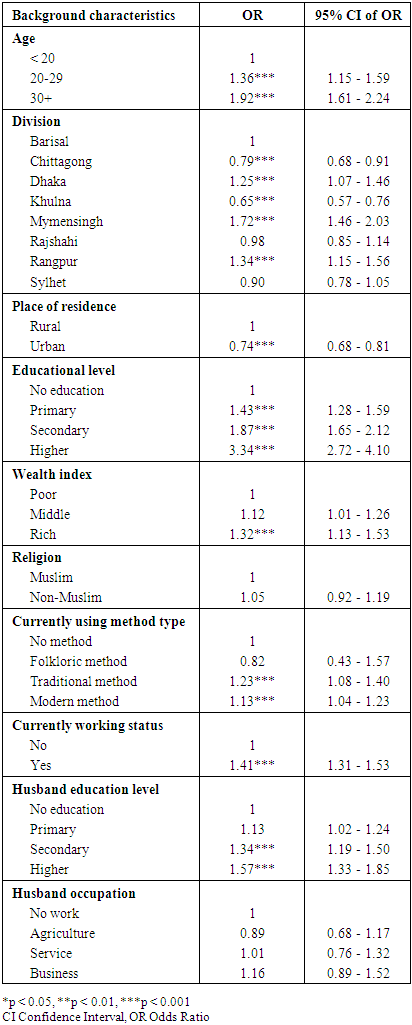
Menstrual regulation (MR) is often utilized as a substitute for abortion in Bangladesh. Despite the remarkable reduction of maternal mortality, unsafe and untimely menstrual regulation (MR) remains a major women health problem in Bangladesh. This study attempts to assess the knowledge, attitude and identify the determinants of MR among ever-married women in Bangladesh. Data for this study have been extracted from the nationally representative Bangladesh Demographic and Health Survey 2017-2018 and uni-variate, bivariate and multivariate analyses were employed. The findings show that the knowledge of MR is 74.1% among ever-married women in Bangladesh. Therein, the knowledge of MR is highest (58.5%) among women aged 30 years or above and lowest among those women aged less than 20 years (5.7%). Women are less likely to have MR if they are from Chittagong (OR: 0.97, 95% CI: 0.68-0.91, p < 0.001) and Khulna (OR: 0.65, 95% CI: 0.57-0.76, p < 0.001) divisions. Women are more likely to have MR if they are completed primary (OR: 1.43, 95% CI: 1.28-1.59, p < 0.001), secondary (OR: 1.87, 95% CI: 1.65-2.12, p < 0.001) and higher (OR: 3.34, 95% CI: 2.72-4.10, p < 0.001) education. Results also show that women are more likely to have MR if they are from high (OR: 1.32, 95% CI: 1.13-1.53, p < 0.001) socio-economic status (SES) group, having contraception of traditional method (OR: 1.23, 95% CI: 1.08-1.40, p < 0.001) and modern method (OR: 1.13, 95% CI: 1.04-1.23, p < 0.001) and being worked (OR: 1.41, 95% CI: 1.31-1.53, p < 0.001). Finally, health policy should prioritize in reducing spatial and socioeconomic inequalities in relation to MR services by ensuring knowledge of accessibility and availability of MR services, especially in suburban divisions in Bangladesh.
Keywords: Menstrual regulation, Knowledge, Determinants, Multivariate analysis, Bangladesh
Cite this paper: Dhaneswar Chandro Sarkar, Knowledge and Attitude of Menstrual Regulation among Ever-Married Women in Bangladesh, Journal of Health Science, Vol. 12 No. 1, 2022, pp. 7-13. doi: 10.5923/j.health.20221201.02.
Article Outline
1. Introduction
- In developing countries, abortion is a significant cause of maternal morbidity and mortality, and often unsafe [1]. As of 2010-2014, an estimated of 55.9 million abortions occur each year globally of which 88% are from developing countries [2]. Between 1990-1994 and 2010-2014, the proportion of abortion has increased from 76% to 88% in developing regions, and 49% of these were unsafe [2,3]. The risk of unsafe clandestine abortion, related complications and deaths are usually high in the countries where the law prohibits abortion or abortion is only permitted to save the life of a woman [2,4,5]. The socio-economic and psychological impact of abortion is also substantial [5]. The international health field has recognized the public health significance of unsafe abortion and there appears to be widespread agreement that unlike many other causes of maternal mortality and morbidity, death and disabilities resulting from unsafe abortion are largely preventable [6,7]. The vice-president of the International Women's Health Coalition maintains that causes of abortion-related deaths and disabilities are "punitive laws, narrowly defined health policies, and failure to provide adequate health and family planning services" [6].Bangladesh is thickly populated country in South Asia having populace thickness 1063 for each square kilometer and all out populace is around 160 million; accomplished maternal mortality related Millennium Development Goal significantly [8,9,10]. Of this colossal populace around 25 percent are women of reproductive age (15-49 years of age) [10]. The nation has high contraceptive prevalence (61%) but there is also unmet needs for family planning due to low utilization of long term or permanent contraceptive methods, a high discontinuation rate [11].With regards to Bangladesh where abortion is illegal except in situations where it is important to save a woman's life and menstrual regulation broadly known as MR is frequently viewed as a substitute process [12]. The process of MR isn't directed by the penal code and hence legislative boundaries are absent for its situation in Bangladesh [13]. Menstrual regulation has been characterized as an interim method for establishing non-pregnancy or in other words, a process to regulate or reestablish the menstrual cycle when menstruation is absent for a short duration. Menstrual Regulation (MR) is a time technique for setting up non-pregnancy for women who are in danger of getting pregnant irrespective of whether conception has happened or not, was introduced in Bangladesh in 1970s as a system to decrease maternal morbidity and mortality related with unsafe abortion. Menstrual regulation is usually conducted without a confirmatory pregnancy test, within 10 weeks of a missed menstrual period by paramedics and within 12 weeks of a missed menstrual period by medical doctors [14]. The Government of Bangladesh has undertaken significant initiatives to improve the accessibility of MR services. These include training of existing mid-level providers such as nurses and midwives, recruiting more MR services providers, making MR services free of cost, increasing the time frame for allowing MR, developing national MR guidelines on service provision and quality of care, and introducing medicinal MR [15,16]. However, a recent study based on health facilities and health professionals’ surveys have reported that the rate of MR has declined, and rate of abortion has increased [17]. Different demand-side issues can be present because of which the health care seeking pattern regarding MR services is hampered or discontinued. The knowledge level of potential service users can be a crucial demand-side issue which can determine the utilization of MR procedures from health-care service centers. It was found in a large scale study (in Bangladesh) that 57% of unmarried adolescents and 40% of married adolescents have not even heard of menstrual regulation [18]. Different service-related confusions and unwillingness have also been found to be generated from the lack of knowledge of MR resulting in non-utilization of MR services in the context of Bangladesh [18-20]. Thus, this study aimed to assess women’s knowledge and attitude of MR and identify the determinants of accessing MR services in Bangladesh using a nationally representative sample from household survey. The findings of this study are important for health policy implications as it can help to design increasing use of MR services, which can reduce maternal morbidity and mortality in Bangladesh.
2. Methods and Materials
2.1. Data Sources
- The data utilized for this study extracted from Bangladesh Demographic and Health Survey (BDHS) 2017-18. The worldwide Demographic and Health Survey serve as a source of population and health data for policymakers and the research community. The 2017-18 BDHS was organized in association with the National Institute of Population and Research and Training (NIPORT), ICF and USA. The investigation was funded by the United States Agency for International Development (USAID) in Bangladesh. This was implemented under the auspices of the National Institute of Population Research and Training (NIPORT), Medical Education and Well-Being Division of the Ministry of Health and Family Welfare, Mitra and Associates, a private investigative agency, was collecting data from October 2017 to March 2018 study.
2.2. Study Design
- The BDHS model for 2017-18 is nationally representative and covers the entire population living in non-governmental housing units in the country. As a sampling frame, the survey lists the Counting Areas (EA) provided by the Population and Housing Census of the People's Republic of Bangladesh for 2011 for the Bangladesh Bureau of Statistics (BBS). The Primary Sample Unit (PSU) of the survey is an EA, with an average of 120 households. Bangladesh has eight administrative units: Barisal, Chittagong, Dhaka, Mymensingh, Khulna, Rajshahi, Rangpur and Sylhet. Each division is partitioned into districts, and each district is separated into Upazilas. Each urban area of the upazila is subdivided into wards, which are further subdivided into mohollas. The rural area of upazilas is partitioned into union parishads (UP). These divisions make it possible to divide the entire country into rural and urban areas.This survey is based on a two-stage stratified sample of households. In the first step, the 675 EA was chosen with the probability corresponding to the EA size, 250 EA in urban areas and 425 EA in rural areas. In the first phase, BBS extracted households according to the specifications provided by the DHS team. A complete household listing operation was conducted on all selected EAs to provide a model framework for second-level households’ selection.In the second stage, an average of 30 households strain samples per EA were selected for statistical confidence in national, urban, and rural, and eight key demographic and health variables. According to this design, 20,250 households have been selected. The completed interview is expected by approximately 20,100 ever-married women aged 15-49. Finally, this study used 16990 ever-married women aged 15-49 years who have ever heard about MR.
2.3. Outcome Variable
- To conduct this study we have used one outcome variable: Heard of MR (menstrual regulation). In this term respondents were asked if they heard of MR or not. For answering this question they respond as yes or no. So heard of MR was categorized as yes or no, where yes means they have heard of MR and no means they do not have heard of MR.
2.4. Explanatory Variables
- From a huge number of variables, we have included 14 explanatory variables in this study these are: women’s age, division, place of residence, women’s educational level, religion, wealth index, current use by method type, women’s currently working status, husband’s educational level and husband’s occupation.
2.5. Statistical Analysis
- Data have been statistically analyzed by univariate, bivariate and multivariate: multiple logistic regression analyses for identify the significant determinants and the effect of explanatory variables on response variable. All data were analyzed using statistical package (SPSS Inc.). A probability of
 was considered statistically significant.
was considered statistically significant.2.5.1. Estimation of Parameters
- The multiple logistic regression model is defined as,
 | (1) |
 | (2) |
 The partial derivatives of the log likelihood with respect to B as,
The partial derivatives of the log likelihood with respect to B as, | (3) |
 is the fitted value of πi: and thus, estimating equations set the fitted sum
is the fitted value of πi: and thus, estimating equations set the fitted sum  In matrix from, we may write the estimating equations as,
In matrix from, we may write the estimating equations as, Note that, the similarity of the least squares estimating equations of the general linear model, which may be written as X'Y = X'Y.
Note that, the similarity of the least squares estimating equations of the general linear model, which may be written as X'Y = X'Y.2.5.2. Test Statistic
- For test the significance of the coefficients the present study used the Wald’s test statistic. To test the hypothesis
 vs.
vs.  the wald’s test statistic is given by;
the wald’s test statistic is given by; Or equivalently,
Or equivalently,  under
under  where
where  can be obtained from the inverse of the observed information matrix. i.e.
can be obtained from the inverse of the observed information matrix. i.e. 
3. Results
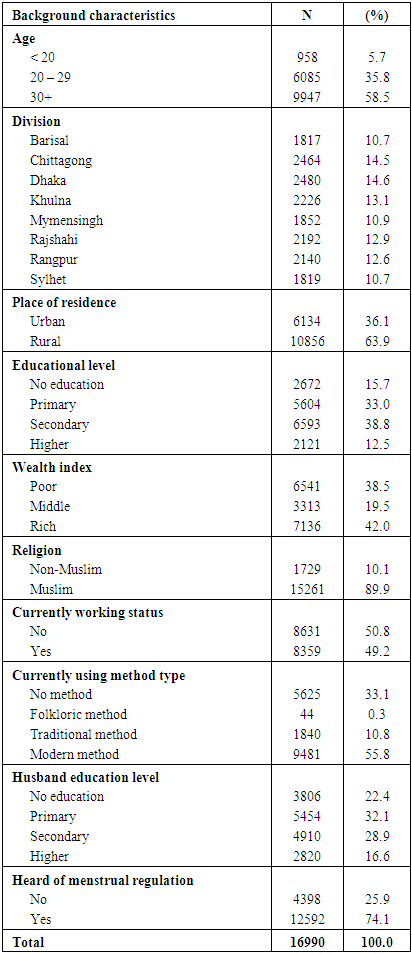
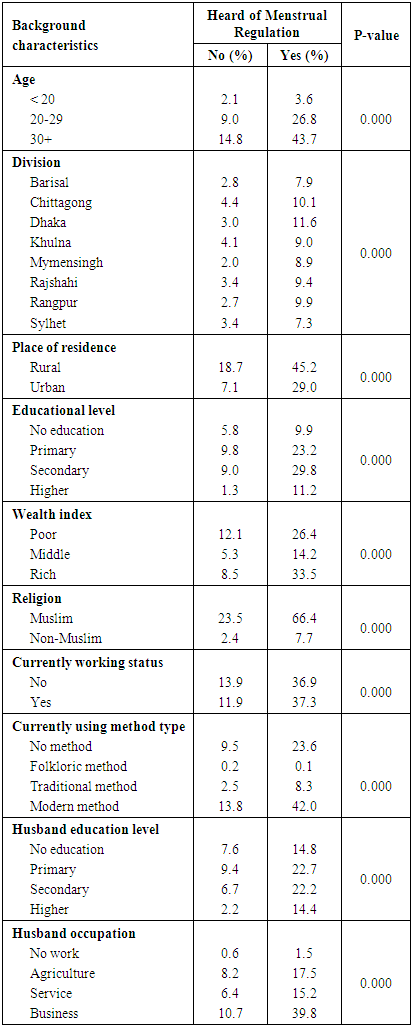
- Characteristics of the study womenOf 16990 study ever-married women, 5.7% belongs to the age less than 20 years, 35.8% belongs to the age group 20-29 years, and 58.5% belongs to the age at 30 years and more. Among the study women, 63.9% lived in rural areas, 15.7% had no formal education, 38.5% lived with lowest wealth, and 89.9% was Muslim (Table 1). About 50.8% of the study ever-married women were unemployed, 33.1% women reported that they did not use any method of contraception, and only 55.8% women were used modern contraception in Bangladesh. Among the participants, 22.4% women’s husband had no formal education, and 25.9% ever-married women had no knowledge of menstrual regulation in Bangladesh (Table 1).
|
 associated with women’s knowledge of menstrual regulation in Bangladesh.
associated with women’s knowledge of menstrual regulation in Bangladesh.
|
|
4. Discussion
- The study reflected a slight rise the knowledge regarding MR of ever-married women in Bangladesh. This finding is consistent with that of another study where a similar scenario of MR related knowledge in Bangladesh was found [15]. Regarding the knowledge of menstrual regulation, it is found to be highest among ever-married women aged 20-29 years and above 30 years. Another study indicated that even in cases where women are aware of the service provision, they are not knowledgeable enough to utilize this information in time for their urgent needs and because of this, existing knowledge seen to be having little impact on utilization of MR [15]. The proportion of MR is disproportionate with the regional concentration, which showed that women from Chittagong and Khulna division are less likely to have MR compared with women from Barisal division. In contrast to women from Barisal division, women in Chittagong and Khulna may have less knowledge and access to MR services, and they face higher restriction and social stigma, which are consistent with previous studies [4,21,22]. The findings of this study suggest that women who completed primary, secondary and higher education are more likely to have MR than the women who no education in Bangladesh which is consistent with other studies [23,24]. Consistent with studies conducted in developing countries, our study revealed that women with higher socio-economic status (SES) are more likely to have MR than their counterpart [22,23,25,26]. Women from higher SES have more control over their reproductive behavior, access to better living standard and health care particularly both public and private health care services [27]. In contrast to our results, some studies showed a reverse association between higher SES of women and lower risk of MR [26,28]. However, most of these studies are conducted in developing countries in which structural mechanisms are entirely different from developing countries [27]. Currently working women have higher odds of MR than the women who are not currently working in Bangladesh, which is consistent with previous studies [23,25,29,30]. The possible explanation could be the overall empowerments of women, which enable them to act on fertility choice, traditional role of mothers, reduce the family size, avoidance of unintended pregnancy and access to MR services [23,25,27,31,32].
5. Conclusions
- This study provides an effort to illustrate the situation regarding the knowledge and attitude of MR in Bangladesh. MR apparently is an indispensable part of the family planning package run by the government. The finding affirms that one fourth women do not have any knowledge of MR in Bangladesh. Findings also show that knowledge of MR is highest among women aged 20-29 years and women aged 30 years and above. The knowledge of MR varied by division and knowledge of MR is highest among women in Dhaka division and lowest among women in Sylhet and Barisal division. Women who were lived in urban areas, knowledge of MR is higher than women who are lived in rural areas. Findings also reveal that women from rich family, currently working women, women education, and women those using contraceptives have higher level of knowledge of MR in Bangladesh. Moreover, the findings of this study suggest that women’s age, administrative division, place of residence, women’s education, SES, contraception, currently working status and husband education are the significant determinants of MR in Bangladesh.
ACKNOWLEDGEMENTS
- I am thankful to the Measure DHS (Demographic and Health Surveys), ICF International, USA for granting access to the BDHS 2017-2018 data. I am also thankful to the National Institute of Population Research and Training (NIPORT) of the Ministry of Health and Family Welfare, Bangladesh for allowing me to use the BDHS 2017-2018 data set.