-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Journal of Health Science
p-ISSN: 2166-5966 e-ISSN: 2166-5990
2018; 8(1): 12-18
doi:10.5923/j.health.20180801.03

Comparative Efficacy of Quadriceps Strengthening, Infrared Radiation Therapy and Oral Diclofenac Sodium in the Management of Symptomatic Osteoarthritis of the Knee
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLEbere Yvonne Ihegihu1, Chima Collins Ihegihu2, Egwuonwu Afamefuna Victor3, Okonkwo Uchenna Prosper1
1Department of Physiotherapy, Nnamdi Azikiwe University Teaching Hospital, Nnewi
2Department of Orthopaedic and Trauma Surgery, Nnamdi Azikiwe University, Nnewi
3Department of Medical Rehabilitation, Nnamdi Azikiwe University, Nnewi
Correspondence to: Egwuonwu Afamefuna Victor, Department of Medical Rehabilitation, Nnamdi Azikiwe University, Nnewi.
| Email: |  |
Copyright © 2018 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Physiotherapy and non steroidal anti-inflammatory drugs form the bedrock of non surgical management of knee osteoarthritis (KOA) which focuses on reducing pain, maintaining or improving joint mobility, limiting functional impairment, and improving health-related quality of life. The purpose of this study was to compare the efficacy of quadriceps strengthening and infrared radiation alone; oral diclofenac sodium alone and the combination of quadriceps strengthening, infrared radiation and oral diclofenac sodium in the management of patients with symptomatic KOA. Knee pain intensity, quadriceps muscle strength and 30.4 metres walk-time were used as outcome measures. Methods: The research population comprised of patients with symptomatic KOA randomly assigned into four groups: group 1 (combination of quadriceps strengthening, infrared therapy and oral diclofenac sodium), group 2 (quadriceps strengthening and infrared therapy), group 3 (oral diclofenac sodium) and group 4 (control/placebo). The participants in groups 1 and 3 received one tablet of diclofenac sodium and one tablet of vitamin B complex twice daily while participants in the groups 2 and 4 received one tablet of vitamin B complex twice daily. In addition, the participants in groups 1 and 2 performed supervised quadriceps strengthening exercises and received infrared radiation therapy three times every week. Each participant was treated for seven consecutive weeks. Results: The participants comprised 43 (33.08%) males and 87 (66.92%) females. The male to female ratio was 1:2. At the end of seven weeks of intervention, there was reduction in the knee pain intensity in groups 1, 2 and 3, which was statistically significant (p<0.05). There was increase in the quadriceps strength in groups 1 and 2 which was statistically significant (p<0.05). There was reduction in the 30.4m walk-time in groups 1, 2 and 3, which was statistically significant (p<0.05). Conclusion: The combination of quadriceps strengthening, infrared radiation and oral diclofenac sodium was superior to oral diclofenac sodium therapy alone in all parameters used for comparison: knee pain intensity, quadriceps muscle strength and 30.4m walk-time. The combination of quadriceps strengthening, infrared radiation and oral diclofenac sodium was also superior to quadriceps strengthening and infrared radiation alone, only in reducing knee pain intensity. However quadriceps strengthening and infrared radiation alone was superior to diclofenac sodium therapy alone in all outcome measures except reducing knee pain intensity.
Keywords: Comparative efficacy, Quadriceps strengthening, Infrared radiation therapy, Oral diclofenac sodium, Knee pain intensity, Quadriceps strengthening, 30.4m walk time
Cite this paper: Ebere Yvonne Ihegihu, Chima Collins Ihegihu, Egwuonwu Afamefuna Victor, Okonkwo Uchenna Prosper, Comparative Efficacy of Quadriceps Strengthening, Infrared Radiation Therapy and Oral Diclofenac Sodium in the Management of Symptomatic Osteoarthritis of the Knee, Journal of Health Science, Vol. 8 No. 1, 2018, pp. 12-18. doi: 10.5923/j.health.20180801.03.
Article Outline
1. Introduction
- Osteoarthritis (OA) of the knee is a chronic, heterogeneous, complex degenerative joint disorder characterized by progressive destruction of articular cartilage with joint space narrowing, osteophyte formation, subchondral sclerosis and synovitis. [1] The knee is the most clinically significant site of primary osteoarthritis involvement [2] and by far the most common cause limiting the daily activities of the elderly population. [3] Clinically patients present with knee pain, knee stiffness, reduced knee joint range of motion, swelling, crepitation and disability. In the knee, OA radiographic abnormalities are present in more than 30% of people aged 65 years and above and approximately 40% are symptomatic [4] affecting more women than men. [5] The current treatments for knee OA focus on ameliorating the illness not cure, since there is presently no pharmacologic agent that modifies the structural changes that occur in OA joints. Reducing knee pain, maintaining or improving knee joint mobility, limiting functional impairment, and improving health-related quality of life (QOL)are the objectives of most knee OA (KOA) treatment protocols. Several guidelines have been recommended for managing OA of the knee. [6, 7, 8, 9] Analgesics, non-steroidal anti- inflammatory drugs (NSAIDs), opioids, weight loss and physiotherapy form the bedrock of management before joint replacement. Physiotherapy is a health care profession that provides a range of non-pharmacological interventions for knee OA. It is frequently recommended in addition to NSAIDs to increase the efficacy of treatment. [6, 7] Physiotherapy encompasses numerous treatment modalities such as quadriceps strengthening exercises, infrared radiation therapy, short-wave diathermy therapy, ultrasound therapy, transcutaneous electrical nerve stimulation (TENS) and interferential therapy. [10, 11] Two studies; such as that by Roddy et al [12] Imoto et al [13] have reported that strengthening the quadriceps muscles can be beneficial in the management of osteoarthritis of the knee. The benefits include improved knee joint range of motion, improved knee function and reduced joint pain. Infrared radiation therapy is frequently used to ameliorate symptoms of osteoarthritis of the knee. Heat from infrared radiation relieves pain by increasing the pain threshold, increasing blood flow and washing away pain producing metabolites. [14] It enables collagen to deform easily causing an increase in the extensibility of the connective tissue [15]. Some researchers have reported that superficial heat decreases joint pain and stiffness, while increasing joint range of motion and improving disability in patients with OA of the knee. [16, 17]Diclofenac sodium a non steroidal anti-Inflammatory drug is among the medications most widely used worldwide in the treatment of OA. It has been shown to decrease pain and stiffness while improving function. [18, 19] Diclofenac sodium prevents prostaglandin synthesis at both the peripheral and central levels by inhibiting Cyclo-oxygenase 1 and 2 (COX-1 and COX2) enzymes non-selectively. [20] It possesses analgesic, anti-inflammatory and antipyretic properties and following administration passes into the synovial fluid where maximum concentrations are measured 2-4 hours after peak plasma values have been obtained. [20] However Diclofenac therapy is associated with undesirable side effects such as gastro-intestinal (GIT) ulcers and bleeding. [21] Other undesirable side effects of diclofenac sodium therapy include destabilization of blood pressure, renal function impairment and an increased risk of cardiovascular events. [22, 23] B vitamins are a class of water-soluble vitamins that play important roles in cell metabolism. Each B vitamin is either a coenzyme for key metabolic processes or is a precursor needed to make one. They have not been reported to have any relieving effect in the treatment of symptomatic OA of the knee.The purpose of this study was to compare the efficacy of the combination of quadriceps strengthening, infrared therapy and oral diclofenac sodium with quadriceps strengthening and infrared therapy alone and oral diclofenac sodium alone in the management of patients with symptomatic OA of the knee using reduction in knee joint pain intensity, increase in quadriceps muscle strength and reduction in 30.4 metres walk-time as outcome measures.
2. Methods
- The research population comprised of patients who had confirmed diagnosis of symptomatic osteoarthritis of the knee according to the criteria established by the American College of Rheumatology. [24] Ethical approval was obtained from Nnamdi Azikiwe University Teaching Hospital Ethical Committee. All patients gave written informed consent for participation. A total of 130 patients aged 45yrs and above were consecutively recruited into the study. Patients who had any form of inflammatory arthropathy, recent injury in the knee, history of peptic ulcer, congestive heart disease, pregnant or lactating were excluded from the study. Patients participating in other clinical trials were also excluded from the study. The sample size for the study was determined using 19.6% prevalence as reported by Brandt. [25] The participants were randomly distributed into four groups: group 1 (combination of quadriceps strengthening, infrared radiation and oral diclofenac sodium); group 2 (quadriceps strengthening and infrared radiation alone); group 3 (oral diclofenac sodium alone) and group 4 (control).
3. Materials
- Diclofenac sodium tablets each containing 50mg of diclofenac sodium (manufactured by Merckle GmbH, Blaubeuren-Weiler, Germany for Mepha LLC, Aesch-Basel, Switzerland) were used for NSAID therapy while vitamin B complex tablets (Manufactured by Emzor Pharmaceutical Industries Isolo-Lagos, Nigeria) each containing 1mg of vitamin B1, 1mg of B2 and 15mg of Nicotinamide were used as the placebo drug. Sand bags of different weights were used to increase resistance during quadriceps strengthening exercises while Infra-red Lamp (Infraphil, Philips model, 150watts) was used for infrared radiation therapy. A Stadiometer (SECA model) was used to measure the weights and heights of the participants and Stop watch (Nokia model, 8850) was used to record walk time. Water Marker was used to mark out anatomical land marks on the participants whilst a masking tape was used to mark out the distance for walk time. An inelastic measuring tape (Bouncing Rabbit, made in China) was used to measure out the 30.4metres walk distance and the quadriceps muscle strength of the affected limbs were obtained using the Oxford grading Scale. [26] Box Numerical Pain Scale (BNPS) of 1-10 was used to assess knee joint pain intensity. [27]The sex, age, occupation, duration of knee pain, family history, social history and radiology reports of weight bearing plain radiographs of the knee(s) of the participants were documented. Baseline knee pain intensity score, quadriceps muscle strength and 30.4m walk-time for each participant were recorded at the beginning of the study. The height, weight and 30.4m walk time of the participants were measured and recorded in metres (m), kilograms (kg) and seconds (sec) respectively. The participants in groups 1 and 3 received one tablet of diclofenac sodium and one tablet of vitamin B complex twice daily (morning and evening) taken before a meal without chewing, together with a glass of water while participants in groups 2 and 4 took one tablet of vitamin B complex only twice daily (morning and evening) before a meal without chewing, together with a glass of water. The drugs were taken by each participant for seven consecutive weeks. In addition the participants in groups 1 and 2 performed supervised quadriceps muscle strengthening exercises (isotonic and isometric) and received infrared radiation therapy [28] three times every week for seven consecutive weeks. The infrared radiation therapy was administered for 15 minutes during each treatment session. During the study period, participants were not allowed to have any additional therapies such as topical NSAIDS, intra-articular corticosteroid injections and other analgesics. At the end of seven weeks, the knee joint pain intensity score; quadriceps muscle strength and 30.4m walk time were measured and recorded for each participant.
4. Data Analysis
- The Statistical Package for Social Sciences (SPSS) version 20 software package was used for the data entry and analysis. Descriptive statistics of mean and standard deviation were calculated for measurements taken. Analysis of variance (ANOVA) was used to compare the baseline characteristics across the four groups. Paired t-test was used to compare pre and post mean test score changes for each parameter (knee pain intensity score, quadriceps strength and 30.4m walk-time) in each treatment group. Alpha level for all statistical analysis employed was set at p<0.05.
5. Results
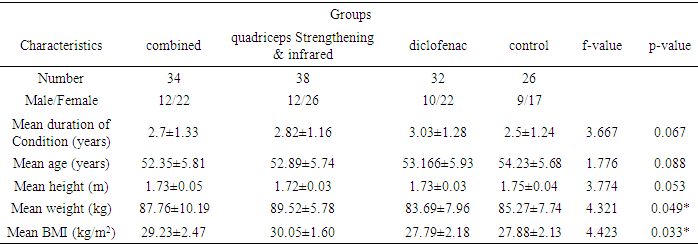
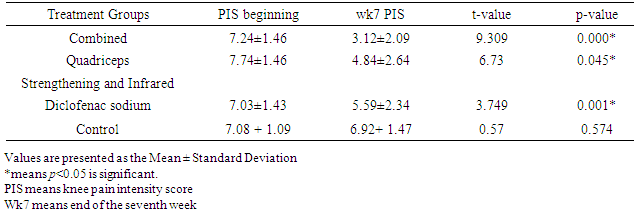
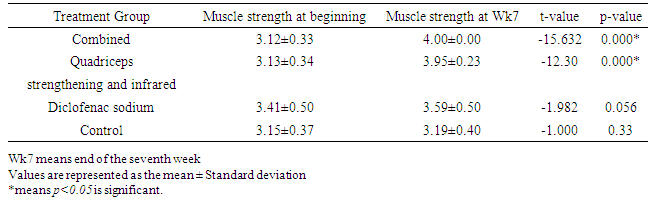
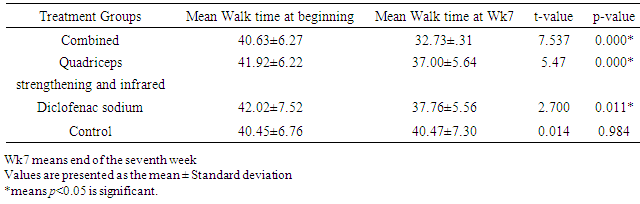
- One hundred and thirty participants completed the study. They comprised 43 (33.08%) males and 87 (66.92%) females. The male to female ratio was 1:2. The participants were within the age range of 45 and 68 years, with a mean age of 52.35 ± 5.81 years. The mean weight, height and body Mass Index (BMI) of the participants were 86±8.19kg, 1.73±0.03m, 28.05±2.17kg/m2 respectively. The mean length of time since onset of condition was 2.79±1.33years. More participants (38) in the quadriceps strengthening and infrared radiation group completed the study when compared with the other three groups (Table 1). The result revealed that least number of patients (26) who completed the study was in the control group. The mean age of 54.23±5.68years of the participants in the control group was more than the mean age of participants in the other groups. The participants in the quadriceps strengthening and infrared radiation group had a higher mean BMI (30.05±1.60kg/m2) and weighed more (89.52±5.78) than the participants in the other groups. The difference in the mean weight and mean BMI were statistically significant (p< 0.05).Table 2 shows the means of the knee pain intensity scores of the participants in the four groups at the beginning and at the end of the study. At the end of seven weeks of treatment, the result revealed that there was significant reduction in the knee pain intensity of the participants in groups 1, 2 and 3, (p< 0.05). The control group did not show any significant reduction in knee joint pain intensity, (p > 0.05).The values of the means of the quadriceps strength at beginning and end of study are presented in Table 3. The result revealed that there was significant increase in the quadriceps strength of the participants in groups 1 and 2 at the end of seven weeks of treatment (p< 0.05). There was no significant increase in the quadriceps muscle strength in groups 3 and 4 (p> 0.05).The values of the means of the 30.4 meter walk-time at beginning and end of the study showed that there was a significant reduction (p< 0.05) in the 30.4m walk-time in all the groups except for the participants in the control group (Table 4). However, participants in groups 1 and 2 demonstrated superior reduction in 30.4m walk time to those in group 3.
|
|
|
|
6. Discussion
- The results of the study revealed that there was significant reduction in knee pain intensity in all the groups except the control group suggesting that quadriceps strengthening and infrared radiation alone and diclofenac sodium alone reduced knee pain intensity. The pain relieving effects of diclofenac sodium is documented in the literature by two researchers and this is as a result of its analgesic and anti-inflammatory properties. [18, 19] The pain relieving effect of infrared radiation therapy has also been reported in other studies. [16, 17] Quadriceps strengthening exercises are effective in improving pain, function and quality of life in patients with osteoarthritis of the knee as reported by Imoto et al. [29] Roddy et al [30] and Lankhorstet al [31] in their studies that quadriceps weakness is common in patients with OA of the knee which correlates with pain and strengthening the quadriceps muscles reduced pain intensity as confirmed in this study. Infrared radiation therapy and quadriceps strengthening exercises increase blood flow and tissue metabolism, relax the muscles and improve stability in the knee joint; properties capable of significantly contributing to reduction in pain intensity. In essence, the sum of the effects of the three therapies on pain could then be a reason for the superior reduction in knee joint pain intensity score in the combined group when compared to the other groups. This further supports the recommendation by the American College of Rheumatology [6] that the medical management of OA of the knee should include a combination of NSAIDS, quadriceps strengthening exercises and other physical modalities. Although the three modalities of treatment significantly reduced knee joint pain intensity in the participants, the results showed that the combination of the three therapies was superior to oral diclofenac sodium alone and quadriceps strengthening and infrared radiation alone. However participants in the diclofenac group showed superior improvement when compared with participants in the quadriceps strengthening and infrared radiation therapy group. There was no significant reduction in knee joint pain intensity in the control group.The participants in groups 1 and 2 demonstrated increased quadriceps muscle strength after performing supervised quadriceps muscle strengthening exercises for seven weeks. The stability and the functional capacity of the knee joint are largely dependent on the quadriceps muscle strength. [32] Thus the affected quadriceps muscles were put through a strengthening exercise regimen during the study in the two groups and increased in strength. This is consistent with the findings of other researchers [30, 33]; that judicious quadriceps strengthening exercises to an osteoarthritic knee improved the quadriceps muscle strength. Participants in the diclofenac sodium group had no significant improvement in quadriceps muscle strength. The study showed that oral diclofenac sodium did not have any significant effect on quadriceps muscle strength. To the best of the researchers’ knowledge, there are no previous studies that have reported on the effect of NSAIDS on quadriceps strength. There was also no significant change in muscle strength in the participants in the control group.There was reduction in the 30.4m walk-time in all the groups except in the placebo group. This could be due to the fact that reduction in pain intensity and increased muscle strength all contributed to improved function and performance of the affected joints. This is consistent with previous studies by Shekelle et al [34] and Barnes [35] and corroborates the findings of Stiskal [36] that exercises improve functional capacities of patients with symptomatic OA of the knee. The reduction in walk-time in the diclofenac group was mainly due to the reduction in pain intensity as a result of its anti-inflammatory and analgesic properties. This is consistent with findings in previous studies by Walker-Bone et al, [37] and Moore et al. [38] however the result also revealed that the combined group and quadriceps strengthening and infrared radiation therapy group showed superior reduction in 30.4m walk-time when compared with the diclofenac group. Quadriceps strengthening exercises and infrared radiation therapy enhance dynamic stability of knee OA joints as reported by Hicks et al. [39] Thus including quadriceps muscle strengthening exercise program and infrared radiation therapy in the management of patients with OA of the knee lead to better functional outcome.
7. Conclusions
- The combination of quadriceps strengthening, infrared radiation and oral diclofenac sodium was superior to oral diclofenac sodium alone in all parameters used for comparison. The combination of quadriceps strengthening, infrared radiation and oral diclofenac sodium was superior to quadriceps strengthening and infrared radiation alone in reducing knee joint pain intensity. However quadriceps strengthening and infrared radiation alone was superior to diclofenac sodium alone in all outcome measures except reduction in knee pain intensity. The placebo group did not show any significant improvement in all the outcome measures at the end of seven weeks of treatment. It is recommended that quadriceps strengthening exercises and infrared radiation therapy be routinely combined with oral diclofenac sodium in the management protocol of patients with symptomatic osteoarthritis of the knee but when oral diclofenac sodium is contraindicated, quadriceps strengthening exercises and infrared radiation therapy may be prescribed.