-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Journal of Health Science
p-ISSN: 2166-5966 e-ISSN: 2166-5990
2017; 7(5): 96-100
doi:10.5923/j.health.20170705.02

Average Length of Stay (ALS) of under Five Years Hospitalized Children: A Study on Bangladesh
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAfsana Yesmen Aurthi1, Arafatur Rahaman2
1Department of Public Health, State University of Bangladesh, Dhaka, Bangladesh
2School of Business Studies, Southeast University, Dhaka, Bangladesh
Correspondence to: Arafatur Rahaman, School of Business Studies, Southeast University, Dhaka, Bangladesh.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

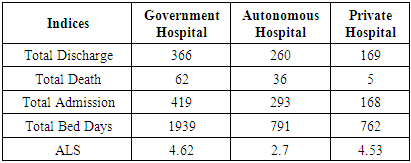
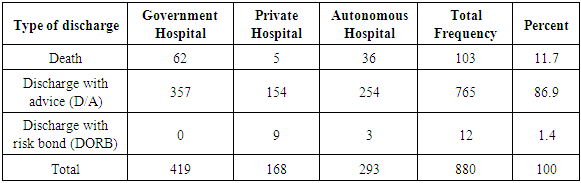
This paper aim was to measure Average Length of Stay (ALS) of under five years child to ensure proper utilization of hospitals resource and to facilitate quality health care. Parents of children had to face daunting experience as if most of the hospitals are not concern about the vulnerability of child health. Children under five years old are usually more prone to various infectious diseases leading to frequent hospitalization that causes high mortality and morbidity. To conduct this study, a total 880 records of the discharged patient of targeted population has taken into consideration and data was analyzed by both descriptive and inferential statistics. Average Length of Stay in the hospital was found 4.62 days, 4.53 days and 2.7 days for govt., private and autonomous hospital respectively. Findings of the study will help hospital administration to increase their efficiency, to find out patients inflow and disease pattern with the average length of stay period which will also help the health sector policymaker to take corrective actions to improve service.
Keywords: Average Length of Stay (ALS), under five year's child, Healthcare efficiency, Bangladesh
Cite this paper: Afsana Yesmen Aurthi, Arafatur Rahaman, Average Length of Stay (ALS) of under Five Years Hospitalized Children: A Study on Bangladesh, Journal of Health Science, Vol. 7 No. 5, 2017, pp. 96-100. doi: 10.5923/j.health.20170705.02.
Article Outline
1. Introduction
- The average length of stay (ALS) refers to the average number of days that patient’s spend in the hospital. It is measured by dividing the total number of days stayed by all inpatients during a period by the number of admissions or discharges during the same period. The health status of developing countries of the world is far from acceptable. In developing countries, a large segment of the population is deprived of access to basic health care, and medical service provider is not conscious about the clients perception and need. Bangladesh is the 9th largest populated country in the world with more than 16 core people on which nearly 80% of total population lives in rural areas, and a majority of them are poor. Unfortunately, it has no notable achievement for child care. No-one wants to be hospitalized their child for illness and any injury. It is a big concern for all parents, carers, and relatives if any of their child having to attend hospital as a patient. Most of the time we have nothing to do with the concern, but we can improve the way of childcare of hospital by improving the service of hospitals. That means designing the service by prioritizing child care as if children are not the same as adults. That is why we need to establish the Children’s National Service Framework standard for hospital services [1].If we can reduce the factors influencing the average length of hospital stay of under 5-year child, it will reduce the health care costs as well as enhance the efficiency of healthcare providers. Hospitals are the most important hospitals for all people to get treatment and medical services. However, only a few percentage of G.N.P is spent on local health services. Out of total 20800 functioning Govt. hospital beds 8230. So, there is a misallocation of both funds and health facilities between the district and national or metropolitan areas [2]. All hospital beds should typically be counted; including for the acute care and for the chronic/long-term care; in both the public and private sectors. The reported for ALS are for the average length of stay for the acute care only. This refers to the number of days (with an overnight stay) that patients spend in an acute-care inpatient institution. It is generally measured by dividing the total number of days stayed by all patients in acute-care inpatient institutions during a year by the number of admissions or discharges [3]. Hospital stay terminated by death is a vital outcome event, with death usually reflecting the severity and burden of disease. Hospital ALS has been the subject of investigation over the past few decades. Previous studies showed that a significant number of factors influence ALS, mainly patient demographics such as age and socioeconomic status, and hospital characteristics [4, 5]. Some studies have reported that low socioeconomic condition can be used to predict longer ALS (on average, longer by 5.9 days in a study by Stelianides et al.) [6]. However, ALS is influenced to varying degrees by various other factors, such as clinicians’ style of practice, the size of the hospital, hospital ownership, teaching status and other hospital characteristics [7, 8]. A patient’s ALS is also highly correlated with their injury or illness severity. The ALS is high for many diseases including cancer, mental diseases, renal diseases and others [9].
1.1. Objectives of the Study
- The specific objectives of the study are outlined below-ü Measuring Average Length of Stay (ALS) of under five years hospitalized children.ü Find out the way of admission and discharge pattern with duration of hospital stay of Under 5 children treated in the study hospitals during the study period. ü Explore the pattern of sickness of the admitted patientsü To find out the demographic characteristics of the admitted patients
2. Justification of the Study
- Under five years age is a sensitive period and more prone to various infections. Child sickness put the parents in severe emotional distress and staying more in hospitals aggravates their distress. The reductions of time spent in the hospital will reduce costs without compromising patient outcomes quality of care. If we can reduce the factors influencing the average length of hospital stay of under 5-year child, it will reduce the health care costs as well as enhance the efficiency of healthcare providers. Hospital beds are most costly out of all facilities in the hospital. In Bangladesh, the doctor population ratio is 1:4869 and estimated populations per hospital bed are 3500 which is inadequate as compared to the standard of developed countries. In this study, researcher' tried to find out the way of admission and discharge pattern with duration of hospital stay of under five years children treated in the study hospitals during the study period.
3. Methodology
- This study was conducted based on retrospective cross-sectional analysis and carried out from three types of hospitals (government, private & autonomous). The average length of stay (ALOS) is calculated by dividing the number of days stayed (from the date of admission to a hospital or other in-patient institution) by the number of discharges during the year in a quantitative form. The total number of days divided by the number of admissions and discharges during a specified period, which results in an average number of days in the hospital for each person admitted. Primary data of this study were collected from pediatric department of selected three hospitals where 880 records of discharged patients of under five years were taken as samples, and the samples considered for the study were the documents of three months from January to March 2013. The secondary data of the study were collected from different international medical journals and scholarly articles. Researcher uses purposive sampling technique for the study. For the analysis, a descriptive statistical test was applied by using Microsoft Excel by presenting the result in simple and compound tables.
4. Results and Analysis
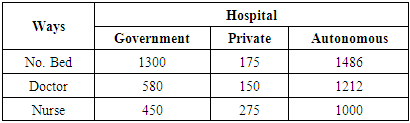
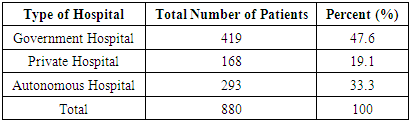
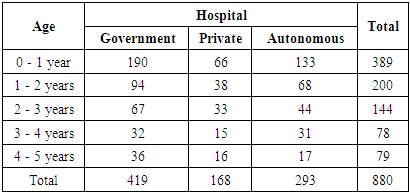
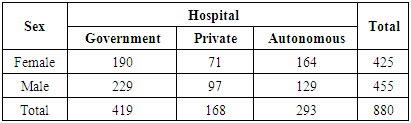
- A retrospective cross-sectional study was conducted among under five-year child in three hospitals (one government, one autonomous and one private). The data were collected from record office & registered documents. A total 880 records of discharged under five years child patients were reviewed. The findings are presented as follows---
|
|
|
|

|
|
|
5. Limitation of the Study
- In this study, the main constrain faced by the researcher is the unavailability of data due to inadequate health information system of hospitals. Additionally, the records of patients are kept in the handwritten document that is really difficult to understand. Data were taken from only Dhaka city. To get the more exact scenario, further study can be done by considering all divisional private, autonomous and govt. medical college hospitals.
6. Recommendations
- The length of stay is frequently used as an indicator of efficiency which can be explained by determining the relationship between input and output. From a perspective, a measure of stay reduction may increase efficiency by increasing the output or decreasing the inputs. Both may be realized by reducing waiting days during a hospital stay or by minimizing the time between consultations, examinations, and procedures. If the reduction of lengths of stay results in increased intensity of care, the efficiency improvement may be smaller. Also, the reduction of hospital days will mainly be a reduction of ‘low care' days. The more intensive and expensive patients remain in the hospital. From the health system perspective, efficiency also depends on the effectiveness of other sectors and the clinical outcomes. When ALS reduction is realized by quicker transfer to follow-up care, the costs of care may be passed.More Instantaneous discharge may increase the pressure on the healthcare sectors, and consequently, the efficiency of the health care system may not improve. Additionally, more insight into the relationship between ALS and quality of care in the hospital needed. If quality improvement leads to shorter ALS and shorter ALS have better outcomes than hospitals with a longer of stay. The connection between ALS and quality of work needs to be investigated. Researchers on clinical epidemiology regarding the disease pattern and average length of stay should be conducted not only in the study hospitals but also all the hospitals in Bangladesh.
7. Conclusions
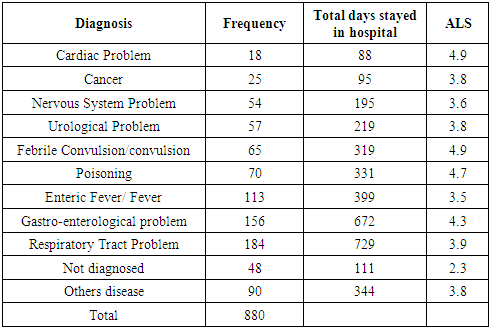
- Health is a fundamental human right and basic human need. The government should be responsible for providing health care to all people in equal measures and to ensure the fulfillment of the health requirements of the population. Under 5 years age is a sensitive period and more amenable to various infections. Child sickness put the parents in severe emotional distress and staying more in hospitals aggravates their distress. In the study, Average Length of Stay (ALS) was found among the under 5 year's child patients in Government Hospital was 4.62 days, and in the autonomous hospital, 2.7 days and Private hospitals were 4.53 days respectively. Children admitted in hospital shows that patients mostly admitted with Respiratory Tract Problem, Gastro-entomological problem, Enteric Fever/Fever, Poisoning and Febrile Convulsion/convulsion. The average length of stay was more of the patients with Febrile Convulsion/convulsion, Cardiac Problem, Poisoning, Gastro-enterological problem and Respiratory Tract Problem. Hospital beds are more costly rather than out of all facilities in the hospital. In Bangladesh, the doctor population ratio is 1:4869 and estimated populations per hospital bed are 3500 which is inadequate as compared to the standard of developed countries. If we can reduce the factors influencing the average length of hospital stay of under 5-year child, it will reduce the health care costs as well as enhance the efficiency of healthcare providers. Declines of time spent in the hospital will reduce costs without compromising patient outcomes quality of care.
ACKNOWLEDGEMENTS
- The author would like to express sincere gratitude to Major Gen. (RTD) M Shahjahan and Prof. Harun-Ar-Rashid for their noteworthy advice, guidance, support and constructive criticism in carrying out of this study.