-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Journal of Health Science
p-ISSN: 2166-5966 e-ISSN: 2166-5990
2017; 7(3): 57-66
doi:10.5923/j.health.20170703.04

Trauma and Conjunctivitis Override any Other Acute Conditions for Professional Health Care Seeking in Rural Bangladesh
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLShabareen Tisha1, S. M. Raysul Haque1, Farhana Habib2
1School of Public Health, Independent University Bangladesh, Dhaka, Bangladesh
2Freelance Researcher, Dhaka, Bangladesh
Correspondence to: Shabareen Tisha, School of Public Health, Independent University Bangladesh, Dhaka, Bangladesh.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

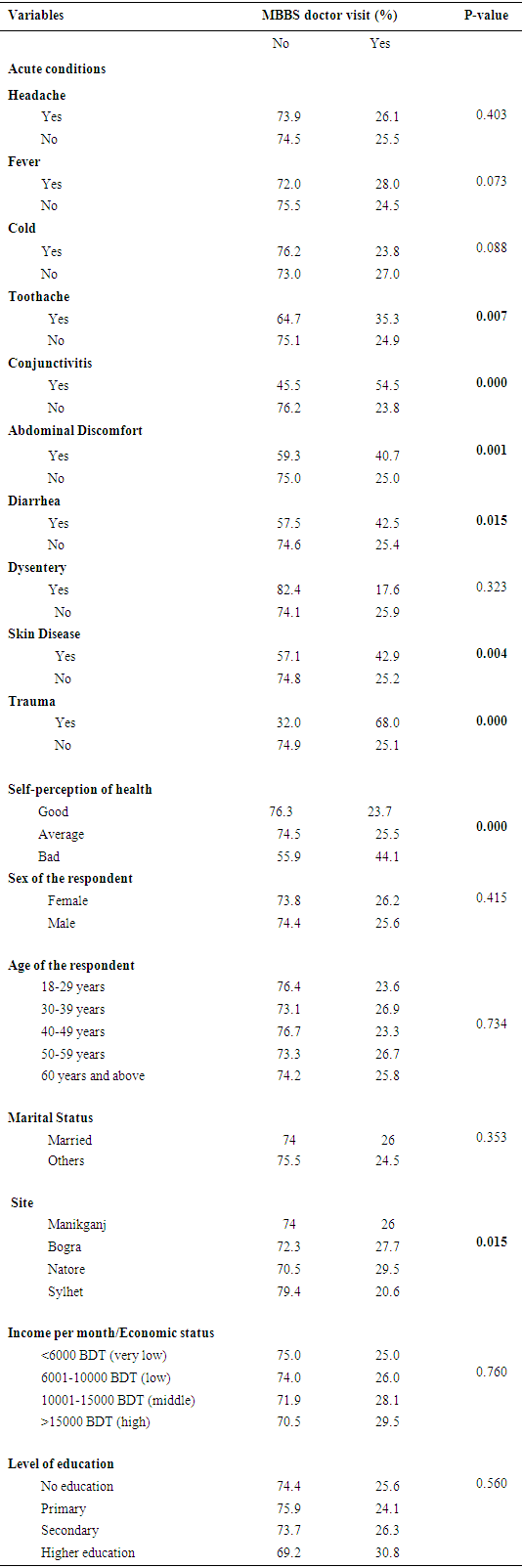
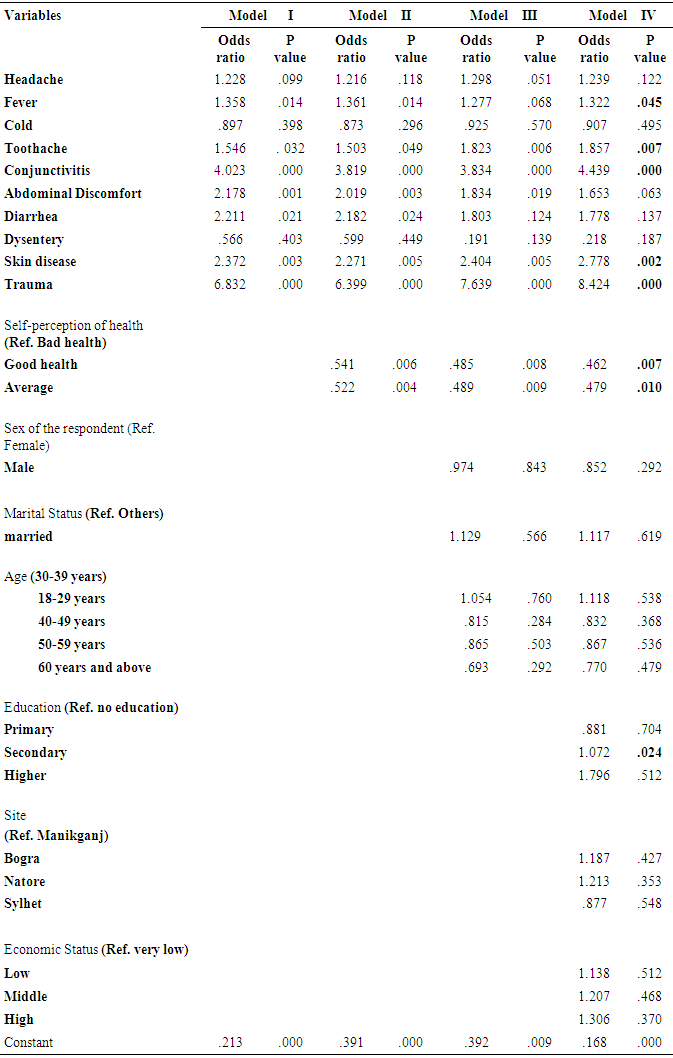
For betterment of health people use to seek health care. Previous researches have revealed that for seeking help only socio demographic variables are responsible. The aim of this study is to reveal the determinants other than socio demographic factors that are responsible for taking decision regarding professional health care. This is a cross-sectional population-based study that used data from the “IUB Health and Socio Economic Survey-2013”. The survey was performed under the authority of Independent University Bangladesh (IUB). The sample size for this study was 1548 adults which were randomly selected from four districts of the country (Manikganj, Bogra, Natore and Sylhet) and they had the history of suffering of any one of mentioned 10 acute conditions, 30 days prior the survey. Frequency distribution, chi square and stepwise logistic regression analysis were done. We find that only 25.8% respondents went to professional health care providers. Respondents mostly suffered from headache and fever (54.8% and 38.6% respectively). About 55.6% respondents believed that they possess good health and 37.2% had average health and rests (7.2%) were in bad health group. People who had self-perceived bad health were more to visit doctors rather than those who had average or good health condition. Toothache, conjunctivitis, abdominal discomfort, diarrhea, skin disease and place of residence had a significant association with MBBS doctor visit (p<.05). Step wise logistic regression analysis was applied to examine the influence of acute conditions on MBBS doctor visits as well as other relevant variables such as self-perception of health, sex, marital status, age, economic status, place of residence, level of education, etc. Throughout the models, the results of the analysis showed that presence of some specific acute conditions such as trauma, conjunctivitis, skin disease were positively and statistically significantly [(P=0.000 & odds ratio = 8.424), (P=0.000 & odds ratio = 4.439) (P=0.002 & odds ratio = 2.778) respectively] associated with the likelihood of an adult person to go to MBBS doctor after controlling for all other potential factors. Type of acute condition is the key determinant for seeking professional healthcare in rural Bangladesh.
Keywords: Acute condition, Professional health care, Health seeking behaviour, Bangladesh
Cite this paper: Shabareen Tisha, S. M. Raysul Haque, Farhana Habib, Trauma and Conjunctivitis Override any Other Acute Conditions for Professional Health Care Seeking in Rural Bangladesh, Journal of Health Science, Vol. 7 No. 3, 2017, pp. 57-66. doi: 10.5923/j.health.20170703.04.
Article Outline
1. Introduction
- Health care seeking decision is a particular aspect of help seeking behavior. Good health is an asset to all. To maintain that health we need health care. Access to health care in developing countries is often quite limited, especially in rural areas. However, less is known about how different factors, such as household structure, household income and education, media exposure, place of residence, awareness modify such access to care. It is clear that people differ in their willingness to seek help from health care services. Some go willingly for treatment, others only when in great pain and in advanced stages of ill health. There are certain factors that help people to take the decision regarding health care. Studies have exemplified that the decision process regarding healthcare seeking for a symptom is complex and depends on a variety of different factors. It has been disputed that women are to pay more attention to their wellness and tend to seek more medical advice than men [1]. Increased income may also promote health by enabling the poor to purchase better health services [2, 3]. From a public health perspective people’s decision about healthcare seeking is important. Awareness about symptoms and healthcare seeking decisions delivers an arena for understanding the edge between the healthcare system and the population. Symptoms potentially indicative of serious disease should preferably lead to healthcare seeking. Further, the awareness regarding some specific symptoms could be a factor for healthcare seeking. This need to be reconnoitered in large-scale studies in a general population. An enhanced understanding of the symptoms and subsequent consequences in the population may improve policy interventions pursuing healthcare seeking. Exploration of self-reported symptoms and health care seeking behavior is therefore very much needed. According to Ahmed et al (2001) there were some illnesses for which people will choose traditional healers, village homeopaths or untrained allopathic doctors above formally trained practitioners [4]. Yamasaki Nakagawa et al (2001) found that women in Nepal were more likely than men to seek help from traditional healers first [5]. The similar finding was obtained in a study in rural Bangladesh where Rahman et al (2000) found that 86% of women received health care from non-qualified health care providers [6]. This has the association with delay in disease diagnosis. Needham et al (2001); Yamasaki-Nakagawa et al (2001) revealed that women have been found to have significantly longer delays to diagnosis than men. In Bangladesh there is a large and growing sector of non-qualified allopathic providers [5, 7]. They are to some extent very easily accessible and cheap in costing. This therefore results bad and unregulated health care practices. Incorporating these unqualified providers into more formal training may therefore be beneficial was suggested by Ahmed et al, (2001) and Uzma et al (1999) [4, 8]. At present in Bangladesh there are 64,434 registered doctors, 6,034 dentists, 30,516 nurses and 27,000 nurse, midwives. The contribution of the health workforce in both public and private sector has increased over the years. The formal health workforce (doctors, dentists, nurses) is mostly concentrated in the urban areas, with variation among regions [9]. As a part of efforts to provide basic preventive and curative health services to all, government and non-governmental organizations (NGOs) have been expanding their health services in rural Bangladesh. [10]. It is to be believed that health systems are inequitable, providing more and higher quality services to the well-off than to the poor, who are unable to obtain them [11]. In this particular study our aim is to explore the factors those are responsible for professional healthcare seeking. There are many more studies that had already explored the determinants for healthcare seeking in different aspects such as gender, specific age group, specific place of residence, definitive occupations or a definitive disease pattern. But we want to give the emphasis on acute conditions only. A disease or disorder that lasts a short time, comes on rapidly and is accompanied by distinct symptoms is known as acute disease. As acute disease lasts for a shorter period of time so there is less possibility to seek healthcare. Not only that in our country people seek help from unprofessional when their suffering is not that much significant. So keeping it in mind we have aimed to find out the acute diseases that led them to seek help from professionals.
2. Research Hypothesis
- Symptoms are the basic predictor for seeking professional healthcare. When people feel sick their economic condition, sex, age, education or place of residence doesn’t play any role for seeking healthcare. Only the nature of acute condition is the key factor for seeking help from professional health care.
3. Data and Method
- This is a cross-sectional population-based study that used data from the “IUB Health and Socio Economic Survey-2013”. The survey was under the authority of Independent University Bangladesh (IUB). The study was performed in four districts (Manikganj, Bogra, Natore and Sylhet) of Bangladesh. Initially those four districts were purposively selected, then three villages from each district were randomly selected and then again 100 households were selected randomly from each village of those four districts. For this study inclusive criteria were age above 18 years and had the history of suffering of any of the mentioned acute conditions. Total numbers of participants were 1548 adults. Demographic, economic and clinical information were obtained by face-to-face interviews conducted at the participants' residence from 5th January -12th January, 2013 using a pre-tested questionnaire. The overall aim of this study was to estimate the prevalence of symptoms based acute morbidity among individuals in the adult population and to explore related factors influencing the decision to contact the professional health care providers. We had also considered the self-perception of general health as a contributor for health care seeking. A comprehensive questionnaire was based on 10 different symptoms that signify different acute conditions. These items were selected based on a review of literature. Followings are the conditions we had considered in our study- Headache, Fever, Cold Toothache, Conjunctivitis, Abdominal discomfort, Diarrhea, Dysentery, Skin disease and Trauma. Items regarding each specific symptom were phrased: “Have you experienced any of the following symptoms or discomfort within the past 30 days?” Those reporting at least one of the abovementioned conditions was labeled as sufferer of acute condition. With regard to health care provider contact, the question was worded for each selected symptom: “To whom did you seek healthcare for this specific health problem?” The questionnaire was pilot- and field-tested. For this specific study, professional health care providers are those who are nonetheless M.B.B.S degree. Rather than these all are categorized as non-professional health care provider as for example community health workers (government and nongovernment), medical assistants or sub assistant community medical officers (SACMO), medicine shop keepers or traditional healers [12]. The analysis was done into multiple steps. Firstly, a univariate analysis was done for both dependent and independent variables. Then, bivariate analysis was done by the Chi-square test to examine the association between the dependent variable and all other independent variables separately. Finally, multivariate analysis was done by fitting the logistic regression model for MBBS doctor visit to examine the impact of acute disease condition after controlling the other potential factors. This was done by following a step-by-step logistic regression model. In first step, we had considered only the acute conditions for MBBS doctor visit. In second step along with acute conditions, we also included self-perception of health where good and average health were in reference to bad health. In the third model along with model II we included sex, marital status and age. The last model had all the independent variables. Here in addition to model III we added education, site of residence and economic status.
4. Results
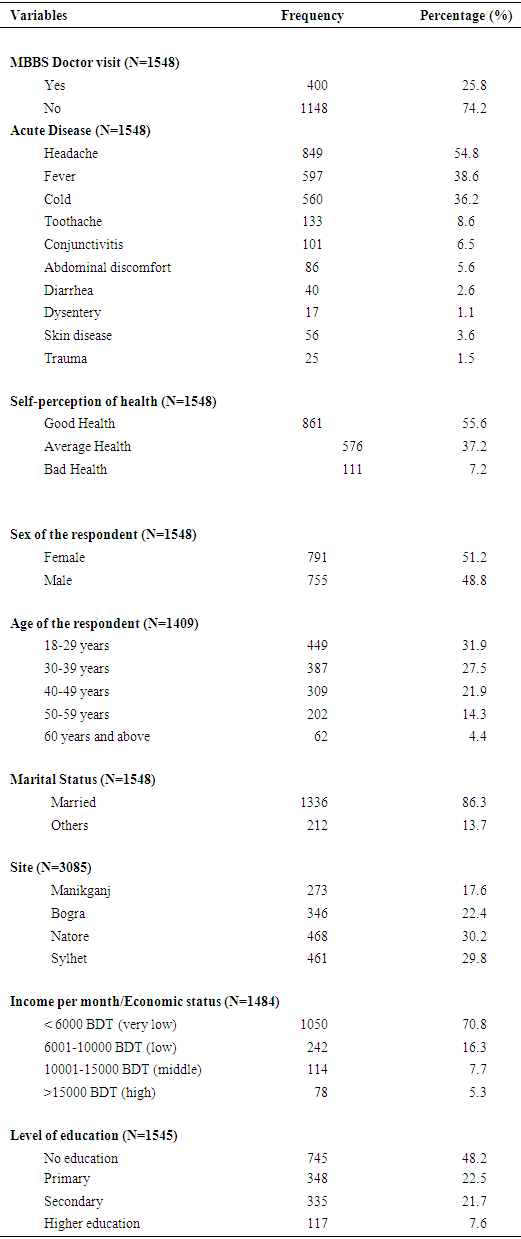
- Table 1 shows frequency distribution of selected independent and dependent variables of the total respondents. We find that 25.8% respondents went to professional health care providers, rest were not. Respondents mostly suffered from headache, fever and cold (54.8%, 38.6% and 36.2 respectively). About 55.6% respondents believed that they possess good health and 37.2% had average health and rest had bad health (7.2%). However, most respondents were females (51.2%), male were 48.8%. Most of them (31.9%) were from the (18-29) years’ age group 27.5% were from 30-39 years’ age group, 40-49 years’ age group were 21.9%, 14.3% were of 50-59 years’ group and rest were (only 4.4%) above 60 years’. Considering marital status 86.3% were married and 13.7% were in the group others like unmarried, widow etc. Considering the site of residence 30.2% were from Natore district, 29.8% were from Sylhet, 22.4% were from Bogra and 17.6% were from Manikganj. Most of the respondents (70.8%) had very low income (below 6000BDT), 16.3% had low income (6001-10000BDT), 7.7% were from middle income group and only 5.3% were from high income group (>15000BDT). 48.2% were uneducated, 22.5% had completed primary education, 21.5% had the history of completion of secondary education and only 7.6% had higher education.
|
|
|
5. Discussion
- In this study we have explored the factors that are responsible for professional health care seeking with a key attention to acute conditions. According to our study the key factor for professional healthcare is the presence of some specific acute conditions that have overridden all the socio demographic variables. Trauma, conjunctivitis and skin disease are such conditions that led people to seek professional care. These conditions are so grave to the sufferers’ that they don’t even think of their socio economic condition or any other associated factors. Our study has the similar findings with the study that had revealed that for acute problems, people focus on the symptoms. The worse they are, the more therapeutic effort occurs was the finding of Verbrugge and Ascione’s study in 1987 [13]. In this study they had said that, how miserable a person feels is the main stimulus to take the action that is seeking proper medical care. Socio-demographic groups scarcely differ in their responses to musculoskeletal injury or trauma. The situation is similar with our study. In addition to this we also get some other acute conditions such as conjunctivitis, skin disease, toothache, abdominal discomfort and fever that are also stimulus for action. Another study conducted by Sumon K. Das revealed that the primary reasons for not seeking health care in Bangladesh were maternal perception about the specific illness and the high cost of treatment [14]. Solome K Bakeera et al explored that lack of wealth is the barrier for health care utilization in Uganda [15]. Income source, transport ownership, and health literacy were reported as centrally useful in overcoming these barriers. These two studies have some similarities with our findings. Though according to Sumon K. Das maternal perception is the vital factor not seeking health care but we found that patient’s perception about the illness is a vital factor. When they feel bad they used to go for treatment otherwise not. On the other hand Solome K Bakeera had also found that community perception was an influencing factor for health care utilization in Uganda which has similarity with our study. On the other side Sumon K. Das had talked about treatment cost in his research. As we don’t have such variable but we’ve used wealth index as a proxy to this so we differ from him, that is for our country context we can say that health care seeking in case of acute disease is dependent on severity of the disease pattern rather than the treatment cost. For almost 2/3rd of the reported symptoms, no gender differences were found concerning the proportion leading to GP contacts was found in a study by Sandra Elnegaard [16]. Our study is also similar to this. Many developing countries, including Bangladesh, recognize MBBS doctors as the highest level of care, but consider them unreachable [17-19]. Accessibility and care seeking are influenced by cultural biases, education, economics, gender, and transportation constraints [20-23]. Syed Masud Ahmed et al in his study found that socioeconomic status was the single most pervasive determinant of health seeking behavior among the study population, overriding age and sex [24]. Our findings differ with it because they had only considered the socio demographic variables not the disease condition. In another study conducted by Ruhul Amin, a principal finding was that a household’s wealth quintiles, was a major determinant in health-seeking behavior [25]. Mothers in the highest wealth quintile were significantly more likely to use modern trained providers for their child health care than those in the poorest quintile. Their main target group was only mothers and their child. But we have studied on adult groups. So the finding of our study varies with it. Ali Arazeem Abdullahi, in his study stated that in Nigeria treatment of malaria in children were largely influenced by the socio-cultural patterns [26]. The study found that the first line of treatment for children with malaria was usually home treatment using traditional herbal medicines. The use of modern health care facilities is the last resort. Their main target group was malaria cases which were quite different from our target group. Rabbani and Alexander found in their study that parental education and income were related to household decisions to seek medical care [27]. They had studied on children which was different from our study population. According to Paul Andrew Bourne the determinants of health care-seeking behavior of Jamaicans were age, area of residents, consumption, marital status, and social class [28]. They had conducted both for urban and rural residents but we have only the rural group. Not only that they had collected the information of self-medication but we haven’t done so. For a specific complaint that is chest symptom, age is the vital factor for seeking health care and next comes site of residence and socio economic condition [29]. The main dissimilarity with this study we have is they went for only a single symptom but we didn’t. Our study has revealed the key determinant for professional health care seeking in acute diseases. According to this study the key determinant is the nature of the acute condition that helps them to seek professional medical care. Trauma and conjunctivitis are the diseases that led them towards MBBS doctors. More and more research is needed to explore other factors those are responsible for health care seeking in acute conditions. Our study constrains are we had explored only four districts of Bangladesh that’s why we couldn’t generalize it. On the other hand our target people were rural only. If we could compare the rural people with urban then we would be able to get more interesting results.
6. Conclusions
- We can conclude by saying that the nature of the acute condition is the key determinant for professional help seeking, in spite of all other socio demographic variables. When someone feels sick his perception regarding his illness is very much important. It’s not always necessary that only the rich or highly educated will seek proper help. There are certain acute conditions like trauma, conjunctivitis or skin disease that lead people towards MBBS doctors. These specific conditions can override other variables like socio economic status, sex, age or education. The type or nature of the disease condition is the basic factor for decision making regarding professional health care seeking. In this regard we should implement different awareness programs. Awareness is one of the best perspectives to prevent and combat acute conditions.
ACKNOWLEDGEMENTS
- We would like to thank Prof. M. Omar Rahman, Vice Chancellor Independent University Bangladesh and Dr. Dipak Mitra, Head, School of Public Health Independent University Bangladesh for permitting us to use the “IUB Health and Socio Economic Survey-2013” and also for their inspiration and motivation for the study.