-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Journal of Health Science
p-ISSN: 2166-5966 e-ISSN: 2166-5990
2016; 6(6): 87-89
doi:10.5923/j.health.20160606.01

Clear Cell Acanthoma on Top of Pre-Existing Psoriatic Plaque: A Rare Case Report
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhalid Al Hawsawi1, Najlaa Alnfaiai1, Nouf Al-Muawad1, Rawa’a Al maghrabi2, Enas Alahmadi1, Dalia Alansari1
1King Abdul Aziz Hospital, Makkah, Saudi Arabia
2Umm Alqura University, College of Medicine, Makkah, Saudi Arabia
Correspondence to: Khalid Al Hawsawi, King Abdul Aziz Hospital, Makkah, Saudi Arabia.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Clear cell acanthoma (CCA) is an uncommon benign tumour of epithelial cells of the epidermis that usually develops slowly over a period of years. Herein, we present a 50 year old Saudi male who is a known case of psoriasis vulgaris presented with asymptomatic solitary skin lesion on top of one of his psoriatic skin lesions for 18 months. Skin examination showed solitary non scaly blackish soft nodule on top of psoriatic plaque on the right side of the trunk. Punch skin biopsy showed psoriasiform acanthosis that is composed of enlarged pale keratinocytes with presence of melanin pigmentation within the keratinocyes. Periodic-acid–Schiff (PAS) staining was positive. On the basis of the above clinicopathological features, the diagnosis of pigmented variant of CCA was made. The lesion was removed by surgical excision. The pigmented variant of CCA and its occurrence on the trunk as well as its occurrence on top of pre-existing psoriatic plaque are unusual presentation of CCA.
Keywords: Clear cell acanthoma of Degos, Degos acanthoma
Cite this paper: Khalid Al Hawsawi, Najlaa Alnfaiai, Nouf Al-Muawad, Rawa’a Al maghrabi, Enas Alahmadi, Dalia Alansari, Clear Cell Acanthoma on Top of Pre-Existing Psoriatic Plaque: A Rare Case Report, Journal of Health Science, Vol. 6 No. 6, 2016, pp. 87-89. doi: 10.5923/j.health.20160606.01.
Article Outline
1. Introduction
- Clear cell acanthoma (CCA) was first described by Degos as ‘acanthome à cellules claires’in 1962. [1] CCA is an uncommon benign tumour of epithelial cells of the epidermis that usually develops slowly over a period of 2–10 years. [1, 2] It is characterized clinically by asymptomatic solitary dome-shaped erythematous papule or plaque with ‘stuck on’ appearance, ranging in size from 3 to 20 mm although larger and multiple lesions have been rarely reported. [2] There may be mild erosions and a serous exudate on the surface of the lesion. It occurs frequently on the lower limbs. However, lesions on the inguinal region, scrotum, face, vermilion mucosa, scalp, palm, trunk, nipple, buttock, forearm, head and toe have been reported. [1, 2] It is common in the middle-age, with no sex predominance. The pathogenesis is not clear. It may be regarded as a variant of seborroheic keratosis (SK) in which there are abundant glycogen-containing keratinocytes. Immunohistochemical and ultrastructural findings are more consistent with interfollicular epidermis. The etiology CCA is unclear. Although it was once thought to be induced by crude coal tar and UV light, researches have failed to demonstrate such link. A recent hypothesis, suggests that CCA is a localized, reactive inflammatory dermatosis. CCA shares a cytokeratin staining pattern similar to that seen in psoriasis. [3-5] Differential diagnosis includes pyogenic granuloma, malignant melanoma, pigmented basal cell carcinoma, squamous cell carcinoma, eccrine poroma, clear cell hidradenoma, metastatic cancer, and dermatofibroma. [6] The histopathological differential diagnosis includes clear cell hidradenoma, hidroacathoma simplex, large cell acanthoma, and eccrine carcinoma. The pigmented variant of CCA and its occurrence on the trunk as well as its occurrence on top of pre-existing psoriatic plaque are unusual presentation of CCA.
2. Case Report
- A 50 year old Saudi male who is a known case of psoriasis on topical steroids and calcipotriene for years, otherwise healthy, presented with 18 months history of new asymptomatic solitary skin lesion on top of one of his psoriatic skin lesions. Skin examination revealed solitary, non scaly, dark brownish soft nodule with stuck on appearance, on top of one of the psoriasis plaque on the right side of his trunk measuring 1.5 x1.5 cm (Figure 1). There is no lymphadenopathy in inguinal, axillary, cervical, submandibular, and occiputal areas. The main differential diagnosis includes pyogenic granuloma, malignant melanoma, eccrine poroma, porocarcinoma, clear cell hidradenoma, and metastatic cancer. Punch skin biopsy showed psoriasiform acanthosis that is composed of enlarged pale keratinocytes with presence of melanin pigmentation within the keratinocyes. The dermis showed sparse perivascular mononuclear lymphohistiocytic cellular infiltrate in the upper dermis (Figure 2). Periodic-acid–Schiff (PAS) staining was positive confirming it is glycogen containing keratinocytes. On the basis of the above clinicopathological findings, a diagnosis of pigmented variant of clear cell acanthoma was made. The patient was reassured. The lesion was removed by surgical excision. He was followed up after surgical excision of the lesion with no recurrences until time of this report.
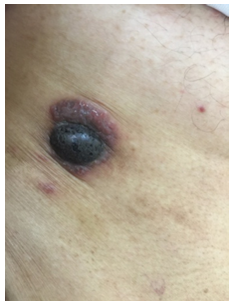 | Figure 1. Trunk of the patient showing blackish soft nodule surrounded by psoriatic plaque |
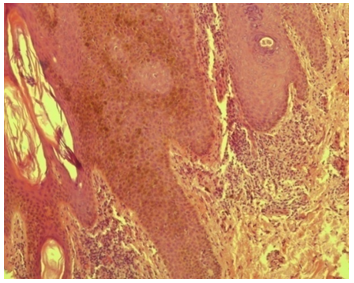 | Figure 2. Histopathological features of the skin lesion showing psoriasiform acanthosis that is composed of enlarged pale keratinocytes with presence of melanin pigmentation within the keratinocyes. The dermis showed sparse perivascular mononuclear lymphohistiocytic cellular infiltrate in the upper dermis |
3. Discussion
- CCA is a rare benign epidermal tumor that originates from epidermal keratinocytes. It presents as an erythematous, rounded papule or plaque with “stuck on” appearance similar to SK. The main differential diagnosis of CCA includes pyogenic granuloma, malignant melanoma, eccrine poroma, porocarcinoma, clear cell hidradenoma, and metastatic cancer. However, each one of these diseases has characteristic histopathological findings. A psoriasiform acanthosis that is composed of enlarged pale keratinocytes with positive PAS staining is characteristic for CCA. A pigmented CCA, like in our case, is a variant of CCA that has been reported rarely in the literatures. It results from presence of dendritic melanocytes containing abundant melanin granules. [7] Other variants of CCA include cystic, and polypoid variants. [8] CCA has been reported rarely to develop on top of pre-existing dermatoses. CCA in our patient developed on top of pre-existing psoriatic plaque. This raises the notion that there are similarities in the histopathologic features between psoriasis and CCA suggesting that there is a common abnormality in the maturation of keratinocytes. However, CCA does not develop following trauma and do not exhibit koebnerization, suggesting they are not simply a variant of localized psoriasis. [6] Treatment options include surgical excision, curettage, electrofulguration, cryotherapy and carbon dioxide laser. There are only a few reported cases of recurrence after excision. [8] Our case did not show any recurrence after surgical excision of the lesion until time of this report.
4. Conclusions
- CCA is a rare benign tumor of epidermal origin. A solitary dome-shaped erythematous papule or plaque with ‘stuck on’ appearance on extremities that develops slowly over a period of 2–10 years is characteristic for CCA. Malignant melanoma, eccrine proma, pyogenic granuloma, and clear cell hidradenoma are the main differential diagnosis. The diagnosis of CCA is confirmed by skin biopsy findings that show psoriasiform acanthosis composed of enlarged pale keratinocytes with positive PAS staining. Our patient showed pigmented variant of CCA, occurrence of CCA on the trunk as well as occurrence of CCA on top of pre-existing psoriatic plaque, all of these are unusual presentations of CCA. Treatment of CCA includes patient reassurance, surgical excision, curettage, electrofulguration, cryotherapy and carbon dioxide.
ACKNOWLEDGMENTS
- No sources of funding were used to assist in preparation of this manuscript. The authors have no conflicts of interest that are directly relevant to the content of this review.
Consent Statement
- Consent has been taken from the patient for purpose of using patient's photographs for publication in print or on the internet.