-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Journal of Health Science
p-ISSN: 2166-5966 e-ISSN: 2166-5990
2016; 6(5): 67-73
doi:10.5923/j.health.20160605.01

Knowledge and Practice of Personal Hygiene among Primary School Students in Sharjah-UAE
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMohammed Ghanim1, Nihar Dash2, Bashayer Abdullah1, Hiba Issa1, Rasha Albarazi1, Zaid Al Saheli1
1Department of Community and Family Medicine, College of Medicine, University of Sharjah, United Arab Emirates
2Department of Clinical Sciences, College of Medicine, University of Sharjah, United Arab Emirates
Correspondence to: Mohammed Ghanim, Department of Community and Family Medicine, College of Medicine, University of Sharjah, United Arab Emirates.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Proper knowledge and practices of personal hygiene plays critical role in avoiding communicable diseases and benefit the primary school children to enjoy healthy and productive school life. The present study evaluated the knowledge and practices related to personal hygiene among primary school children in Sharjah.This cross-sectional study involving 428 primary school children was conducted in Sharjah, United Arab Emirates. Out of 428 students, 155 were from grade 1 (27%), 164 from grade 3 (38%) and 149 from grade 5 (35%). The mean age for students was 8.61 years (SD=1.91). The ability to define personal hygiene was significantly higher among girls (95%) (N=194) as compared to boys (82%) (N= 183). Parents and teachers were the most common source of knowledge providers about personal hygiene to the participants. With the existing knowledge and practices related to personal hygiene among the students, parents and teachers can play positive and significant role to improve it further.
Keywords: Personal hygiene, Hand hygiene, Hand washing, Primary school children
Cite this paper: Mohammed Ghanim, Nihar Dash, Bashayer Abdullah, Hiba Issa, Rasha Albarazi, Zaid Al Saheli, Knowledge and Practice of Personal Hygiene among Primary School Students in Sharjah-UAE, Journal of Health Science, Vol. 6 No. 5, 2016, pp. 67-73. doi: 10.5923/j.health.20160605.01.
Article Outline
1. Introduction
- The increased burden of communicable diseases among school children due to poor personal hygiene practices and inadequate sanitary conditions remains a concern on the public health agenda in developing countries [1]. School children are particularly vulnerable to neglect of basic personal hygiene due lack of knowledge and practice [2]. Poor knowledge, practice of and attitudes to personal hygiene such as hand washing play major roles in the high incidence of communicable diseases and therefore has negative consequences for a child’s long term overall development [3].Improved awareness and hand hygiene practices especially among children have effectively reduced gastrointestinal and respiratory tract infections by up to 50% the two leading causes of childhood morbidity and mortality around the world [4-6]. In addition, studies have also shown that school children with better knowledge and practices of personal hygiene have fewer sick days and absenteeism in school and achieve higher grades [2, 7].School is the place where health education regarding important aspects of hygiene, environment and sanitation, as well as social customs is being imparted [8]. Health is a key factor in school entry, as well as continued participation and attainment in school. The teacher is the guardian of the child in school and plays a pivotal role in the whole process of primordial prevention [9]. Bearing in mind that school children have been consistently implicated in the spread of communicable diseases and that the school has been recognized as a vital setting for health promotion [10], this study was planned to assess personal hygiene in primary school children in Sharjah, United Arab Emirates. The aim of this study was to investigate existing knowledge and practices related to personal hygiene among primary school children between grade 1 and 5. The results from the study will help to understand the factors influencing the personal hygiene behaviors in primary school children and to overcome barriers in acquisition of proper knowledge and practices.
2. Methods
- This is a cross sectional study involving 428 primary school students in Sharjah, United Arab Emirates (UAE). The students were selected based on the stratified random sampling technique, in which the schools were divided into male and female schools, and from each stratum we applied the systematic random sampling technique to choose the appropriate number. A questionnaire containing 35 questions was used to collect data including information about knowledge and practices related to personal hygiene. In addition to that, subjective observations of variables related to personal hygiene were performed. The study used SPSS (21) was used to enter and analyze the data using Chi-square and ANOVA statistical tests.
3. Results
- A total of 428 students participated in this study, 224 boys (52.3%) and 204 girls (47.7%). 155 students were from grade 1 (26.9%), 164 were from grade 3 (38.3%) and 149 were from grade 5 (34.8%) The mean age for students was 8.6 years (SD=1.91). Two hundred seventy eight students (65%) had adequate perception about personal hygiene, but only 27% (N= 116) mentioned that personal hygiene was important to fight diseases (figure 1). The ability to define personal hygiene was significantly higher among girls (95%) (194 of 204) as compared to boys (82%) (183 of 224). Based on a quiz out of five, the average knowledge related to basic personal hygiene recorded among girls (4.45) was significantly higher than among boys (3.83) (p<0.005). Taking shower (62%) (N=265) and washing of hands (60%) (N=257) were the two top ranked hygiene practices reported by the students. Before meals, after using toilets and after playing were the major episodes for washing of their hands (figure 2) and 71% (182 of 257) used soap and water regularly to wash their hands. The use of a hand sanitizer was reported by 38% (N=162) of the students however, the frequency of usages differ widely. The most common reasons for not washing their hands were forgetfulness and lack of time (N=235, 55% and N=77, 18% respectively). Brushing of teeth as a component of personal hygiene was realized only among 23% (N=98) of the students. After waking up in the morning and before going to bed were the two most common times when the students brushed their teeth (N=304, 71% and N=265, 62% respectively). Parents and teachers were the most common source of knowledge providers about personal hygiene to the participants (figure 3).
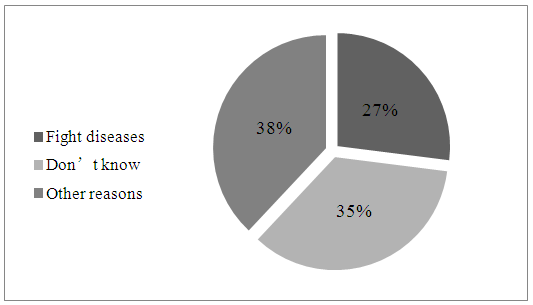 | Figure 1. Students’ perception about the importance of personal hygiene |
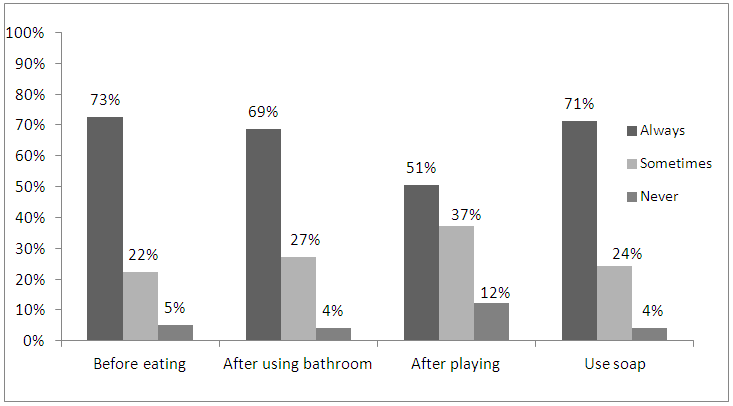 | Figure 2. Hand washing practices as reported by students |
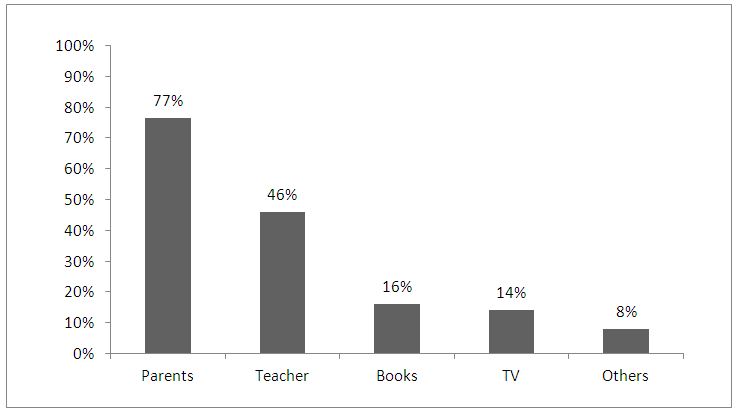 | Figure 3. Information sources of personal hygiene |
4. Discussion
- In this study we assessed the knowledge and practices of personal hygiene among 428 primary school students in grade 1, 3 and 5. To begin with, 65% (N=278) of students (figure 1) had some perceptions about the importance of personal hygiene and could spell it out when interviewed. This was very encouraging finding as we know that hygiene practices are heavily influenced by individual’s awareness, knowledge and attitude [2]. Schools are the right place to initiate this behaviour early in the childhood. In addition, the study observed that around half (46%) (N=197) of the students mentioned their teachers as a source of information regarding personal hygiene (fig 3). These observations clearly demonstrated that the schools and its teachers can play a vital role in imparting the knowledge and practices of personal hygiene very early in the Childs’ life. It is well known that children are more receptive to learning and are very likely to adopt healthy behaviours at a younger age. Furthermore, they have also demonstrated that they can also be agents of change by spreading what they have learned in school to their family and community at large [2, 3].We have observed that knowledge and practices of hygiene was well correlated with students wearing clean cloths and presentable appearance. We also found out that girls showed better knowledge and practices, related to personal hygiene, than boys. Based on a quiz out of five, the average knowledge related to basic personal hygiene recorded among girls (4.45) was significantly higher than among boys (3.83) (p<0.005). Strikingly, the finding of the mean score for girls (4.15 ± 0.98) was significantly higher than that for boys (3.2 ± 1.4) [P<0.05] in an Indian study as well [9]. This finding was expected as girls take care of themselves, and care about their self-image more than boys. It was also noted that the knowledge and practices of personal hygiene was correlated to their academic achievements. This interesting observation goes with the notion that clean hands possess clean books that achieves better grades. [7, 11, 16]Showering was the most important aspect of personal hygiene (62%) (N=265), as ranked by the students. This observation was unique to this study. We believe that the local hot, dry and dusty desert climate and adequate water availability might have influenced in ranking showering or bathing to be the most important hygiene practice among the students. This is in contrast to studies from Africa and Asia where the researchers have reported bathing and washing of hair are the least common practices of personal hygiene [2, 11] and the reason was due to inadequate water availability.When it comes to hand washing, our results are consistent with previous studies [12, 13]. Just bbefore eating, after using toilets and after playing were the major episodes when the students washed their hands and a great proportion of the study population (71%) used soap. As we know that hand washing with soap is the simplest cost effective health prevention technique; it was reassuring to observe this hand washing behaviour in majority of our students. Also, adequate hand hygiene is great deterrent to the spread of gastro intestinal and respiratory tract infections especially in children. Previous studies have shown that washing of hands using soap can prevent these infections and in turn reduces the absenteeism in the schools [14-16]. It was also interesting to note that hand sanitizer usages is also being encouraged as a practice of hand hygiene among the primary school children. The current study had several potential limitations including inappropriate responses from children and relying on subjective observations by the researchers.
5. Conclusions and Recommendations
- The study concluded that personal hygiene knowledge and practices are satisfactory among the school children in Sharjah. Personal hygiene is not an isolated behaviour; instead it varies from person to person according to different factors. Intervention programs raising the awareness and importance of personal hygiene among school children through coordinated education measures by parents, teachers and media will be beneficial to impart these early in life. Based on our research finding we believe that the educational authorities in the country can develop and adopt policies and guidelines that will make way to have adequate access to resources, items and opportunities to maintain personal hygiene at school and home. Schools should provide hygiene education to kindergarten and early grade school children to supplement the training provided by parents and guardians, to ensure that all children learn at an appropriate age how to protect themselves and others from preventable exposure to illness and other hygienic hazards.
ACKNOWLEDGEMENTS
- We would like to extend our sincere thanks to Dr. Anwar Khursheed and Mrs. Amal Hussain and all the principals, headmasters, teachers and supervisors of the participating schools for helping us in completion of the study.
Appendix
- RESEARCH PROPOSAL DETAILSWhat is the research question?What are the knowledge and practices related to personal hygiene among primary school students in Sharjah?Outline, briefly, the background to the research rationale, clarifying its significance.The increased burden of communicable diseases among school children due to poor personal hygiene practices and inadequate sanitary conditions remains a concern on the public health agenda in developing countries. Health is a key factor in school entry, as well as continued participation and attainment in school. School is the place where health education regarding important aspects of hygiene, environment and sanitation, as well as social customs, is being imparted. The teacher is the guardian of the child in school and plays a pivotal role in the whole process of primordial prevention. (Soumya Deb et al, 2010). Poor knowledge and practice of and attitudes to personal hygiene such as hand washing play major roles in the high incidence of communicable diseases and therefore has negative consequences for a child’s long term overall development.School children are particularly vulnerable to neglect of basic personal hygiene (Postma et al, 2004; Oduntan; 1974; Enahoro and Orok; 1986). The consequences in terms of morbidity and mortality are also more severe in them compared to adults. The hands are probably the single most important route for transmission of infection in the home and community, as they are often in direct contact with the mouth, nose and conjunctiva of the eyes). They also come in contact with food and water that is consumed. Studies have revealed a strong and consistent causal link between poor hand hygiene and gastrointestinal infection. Certain respiratory infections (common cold, influenza virus infection, etc) have also been linked to poor personal hygienic practices. Bearing in mind that school children have been consistently implicated in the spread of communicable diseases (Monto AS, 2002) and that the school has been recognized as a vital setting for health promotion (Catalina Lopez-Quintero et al, 2009), we are planning to assess personal hygiene in primary school children in Sharjah.Objectives • How much do primary school students in Sharjah know about personal hygiene?• What are the hand washing habits of primary school students in Sharjah?• What are the teeth brushing habits of primary school students in Sharjah?• What are the showering habits of primary school students in Sharjah?• What is the source of knowledge of primary school students in Sharjah about personal hygiene? • Is personal hygiene affected by gender?• Is personal hygiene affected by academic achievement?• Is personal hygiene affected by whether their parents work or not?MethodologyStudy DesignChoose the design that conforms to your research proposalo Qualitativeo Ethnographico Grounded theoryo Historicalo Case studieso Focus Groupso PhenomenologicalüOthers, specify: Cross Sectional (Quantitative)How does the selected design relate (is appropriate to) fulfilment of study objectives?Cross-sectional studies involve data collected at a defined time. The use of routinely collected data allows large cross-sectional studies to be made at little or no expense. This is a major advantage over other forms of epidemiological studies. Hence, our research design best fits to our study objectives. Study Population Target populationPrimary school students in SharjahSample population (from sample will be chosen)Primary school students in Sharjah studying in the public sectorStudy population (actual sample selected)As will be explained later, we are going to pick 6 schools (3 males and 3 females) to be the actual samples. This will be done after making the sample frame, after we get the list of public primary schools in Sharjah from the Ministry of Education.Sampling Sampling Method(s)After getting a list of public primary schools in Sharjah from the Ministry of Education, we are going to create a sampling frame. We are going to apply the stratified random sampling technique, in which we will divide the schools for male and female schools, and from each stratum we will apply the systematic random sampling technique to choose the appropriate number of schools.Sample Size NeededUsing the formula n = [4 p (1 - p)] / ME^2, and assuming that the expected prevalence is 50% and the margin of error is 5%, ‘n’ will be 385. Hence, our sample size is 400 students, after adding 15 to the 385 as a margin for non-response.Sample JustificationThe 400 students will equally be divided to 200 boys and 200 girls. As we picked grades 1, 3 and 5 to present the population, the 200 students divided by 3 will give approximately 67 students for each grade. Assuming that each class has between 20-25 students, we need to visit 3 schools for each gender. In other words, 22 students multiplied by 3 grades are 66, multiplied by 6 schools gives 396 students. Inclusion/Exclusion CriteriaThere are no inclusion/exclusion criteria; because there are no special requirements, socioeconomic status, geographic location or disease characteristics in our study, i.e it includes all students.Research Instrument (Questionnaire filled by us as we interview the subjects) Demographics: 1) Gender:1. Boy 2. Girl 2) How old are you?.....................................3) In which grade are you?1. Grade 12. Grade 33. Grade 54) Does your mum work?1. Yes2. NoIf yes, specify………………………………5) Does your dad work?1. Yes2. NoIf yes, specify………………………………6) Academic achievement: ………………….Knowledge: 7) What does personal hygiene mean?………………………………………………………………………………………………………………8) What does personal hygiene include?………………………………………………………………………………………………………………9) Is it important?1. Yes2. No 10) If yes, why? ………………………………………………………………………………………………………………
 16) From where did you get the knowledge about personal hygiene? (you can choose more than one)1. Parents2. Teacher3. TV 4. Books5. Others: Please specify ………Practices: Hand hygiene:
16) From where did you get the knowledge about personal hygiene? (you can choose more than one)1. Parents2. Teacher3. TV 4. Books5. Others: Please specify ………Practices: Hand hygiene: 22) Do you have a hand sanitizer?1. Yes2. No23) How often do you use hand sanitizer instead of hands washing in school?1. Always 2. Sometimes3. Never24) What is the main reason for skipping hand washing?1. Far from the sink2. No time3. No need4. Keep forgetting5. Others ………………………….Oral hygiene:
22) Do you have a hand sanitizer?1. Yes2. No23) How often do you use hand sanitizer instead of hands washing in school?1. Always 2. Sometimes3. Never24) What is the main reason for skipping hand washing?1. Far from the sink2. No time3. No need4. Keep forgetting5. Others ………………………….Oral hygiene: 31) How often do you brush your teeth?1. Every day 2. Every other day 3. Two times per week 4. Once per week 5. Less than once per week32) Do you visit the dentist?1. Yes 2. No33) If yes, how often do you visit the dentist?1. Once a year 2. Twice a year 3. More than twice a year 4. When having pain only Showering:34) How often do you shower? 1. More than once daily 2. Once per day 3. Every other day 4. Twice per week 5. Once per week 6. Less than once per week35) Do you shower alone?1. Yes2. No36) If no, who helps you showering? 1. Mum2. Dad 3. House maid4. Others ……………..Observation:Objectively observed personal hygiene characteristics:
31) How often do you brush your teeth?1. Every day 2. Every other day 3. Two times per week 4. Once per week 5. Less than once per week32) Do you visit the dentist?1. Yes 2. No33) If yes, how often do you visit the dentist?1. Once a year 2. Twice a year 3. More than twice a year 4. When having pain only Showering:34) How often do you shower? 1. More than once daily 2. Once per day 3. Every other day 4. Twice per week 5. Once per week 6. Less than once per week35) Do you shower alone?1. Yes2. No36) If no, who helps you showering? 1. Mum2. Dad 3. House maid4. Others ……………..Observation:Objectively observed personal hygiene characteristics:  (End of Questionnaire)
(End of Questionnaire)