-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Journal of Health Science
p-ISSN: 2166-5966 e-ISSN: 2166-5990
2016; 6(4): 53-56
doi:10.5923/j.health.20160604.01

Chest Pain: Walking through a Common Symptom
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLPaulo Dinis1, M. Carmo Cachulo1, Luís Paiva1, 2, Lino Gonçalves1, 2
1Cardiology Department, Coimbra’s Hospital and University Centre, Coimbra, Portugal
2Faculty of Medicine of the University of Coimbra, Portugal
Correspondence to: Paulo Dinis, Cardiology Department, Coimbra’s Hospital and University Centre, Coimbra, Portugal.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

A 35-year-old man presented with persistent chest pain. The patient had no known cardiovascular risk factors and an uneventful physical examination. The electrocardiogram showed a biphasic T wave in precordial leads. His echocardiogram revealed an echogenic mass of irregular appearance in the ventricular apex. A more detailed patient interview uncovered a past history of a skin lump. We continued our investigation with thoracic computed tomography and nuclear magnetic resonance, followed by cardiac biopsy that established the diagnosis of cardiac metastasis of a previous skin melanoma. His hospitalization complicated with intense and persistent chest pain refractory to treatment with conventional analgesics, nonsteroidal anti-inflammatory drugs and colchicine. Merely, adjuvant corticosteroid was able to control the incapacitating pain, although for a short period of time. This case illustrates a common symptom associated with a dismal cause, where time to diagnosis his critical and treatment of patient’s symptoms is sometimes challenging.
Keywords: Chest pain, Pericarditis, Melanoma
Cite this paper: Paulo Dinis, M. Carmo Cachulo, Luís Paiva, Lino Gonçalves, Chest Pain: Walking through a Common Symptom, Journal of Health Science, Vol. 6 No. 4, 2016, pp. 53-56. doi: 10.5923/j.health.20160604.01.
1. Introduction
- Chest pain is a major reason for hospital admission. There are several clinical entities that can cause this symptom, both cardiac and non-cardiac. Although, coronary heart disease is one of the leading causes of death in developed countries, there are several other conditions that can initially present with chest pain. The clinical history and physical examination are crucial to guide clinical investigation and establish the correct diagnosis. We report a case of a patient complaining of intense and progressively frequent chest pain.
2. Case Report
- A 35-year-old black male was admitted to the hospital complaining of progressively frequent chest pain that irradiates to both arms. He had this symptom in the last two months with maximum duration of a few minutes. He denied worsening pain on deep inspiration. Previously treated with nitroglycerin transdermal patch, aspirin and proton pump inhibitor by his family doctor. He had no cardiovascular risk factors, and no family history of heart disease. At presentation, he was apyretic, the physical examination revealed no significant abnormalities, and he didn’t have friction rub in cardiac auscultation. The electrocardiogram (ECG) showed a biphasic T wave in precordial leads (fig.1).
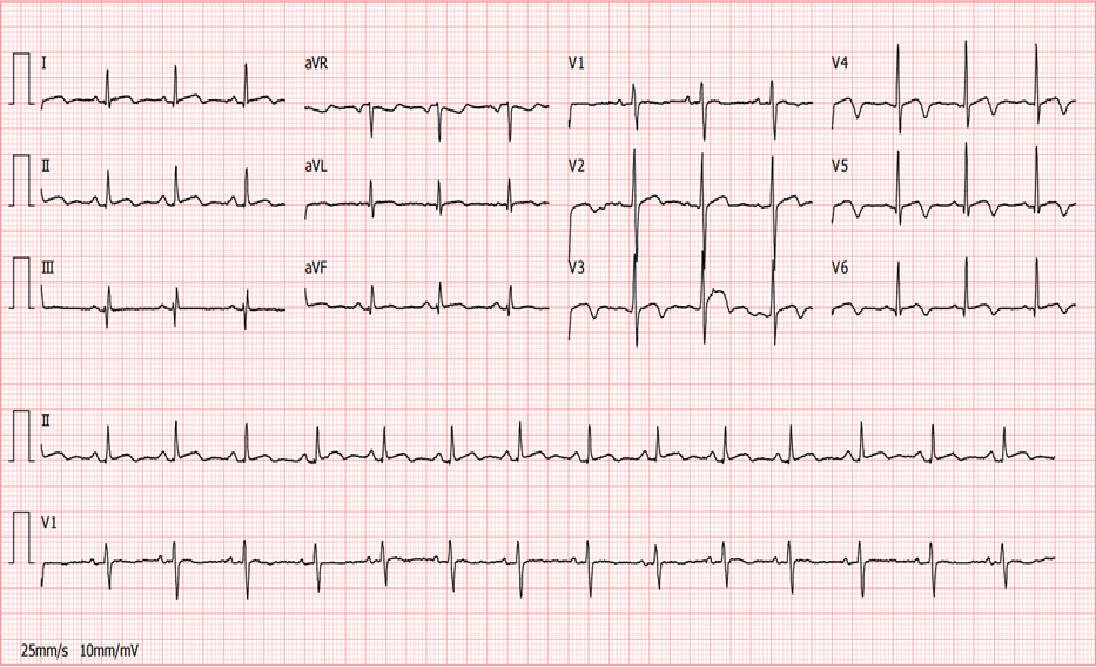 | Figure 1. ECG with biphasic T wave in precordial leads |
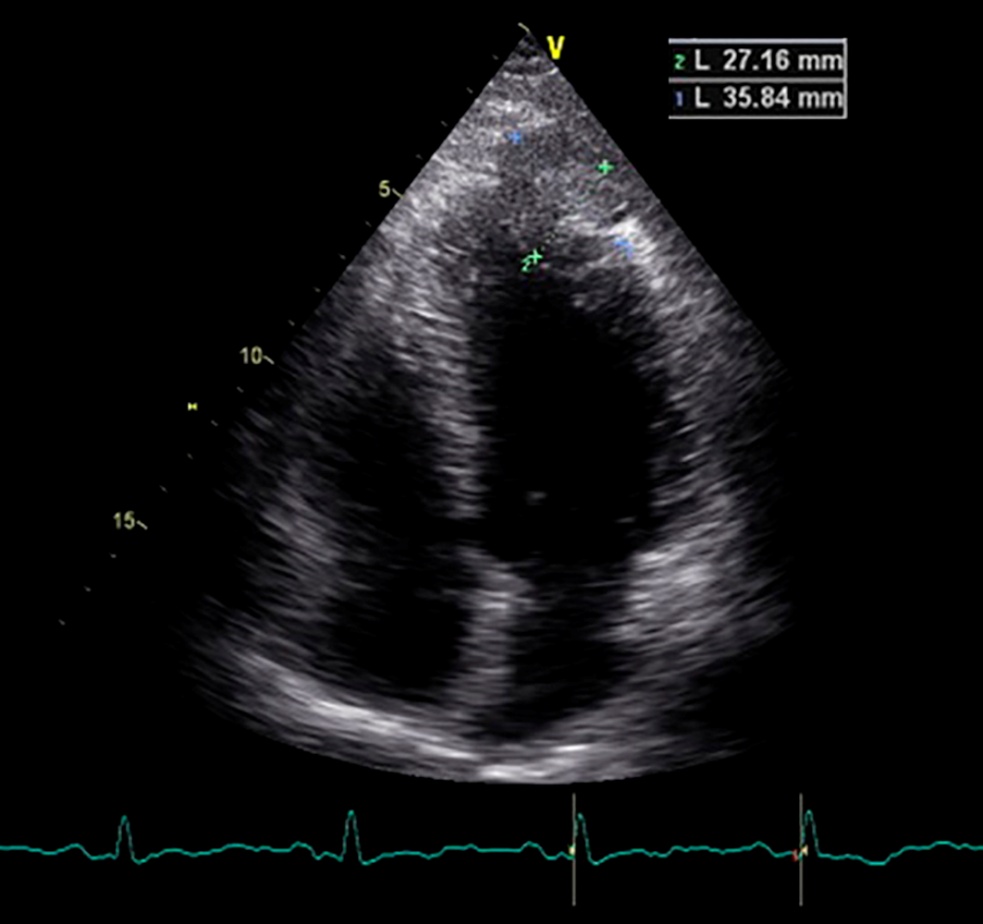 | Figure 2. Echocardiogram revealed an echogenic mass of irregular appearance in the left ventricular apex |
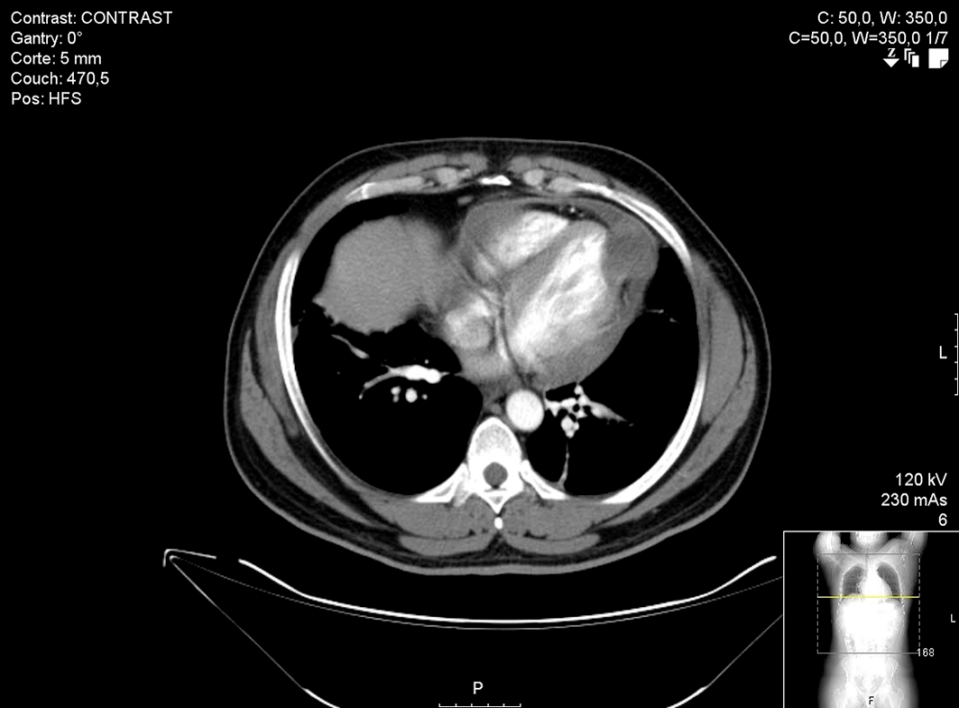
 | Figure 3. Thoracic CT revealed a lesion of soft density measuring 40x38x38 mm |
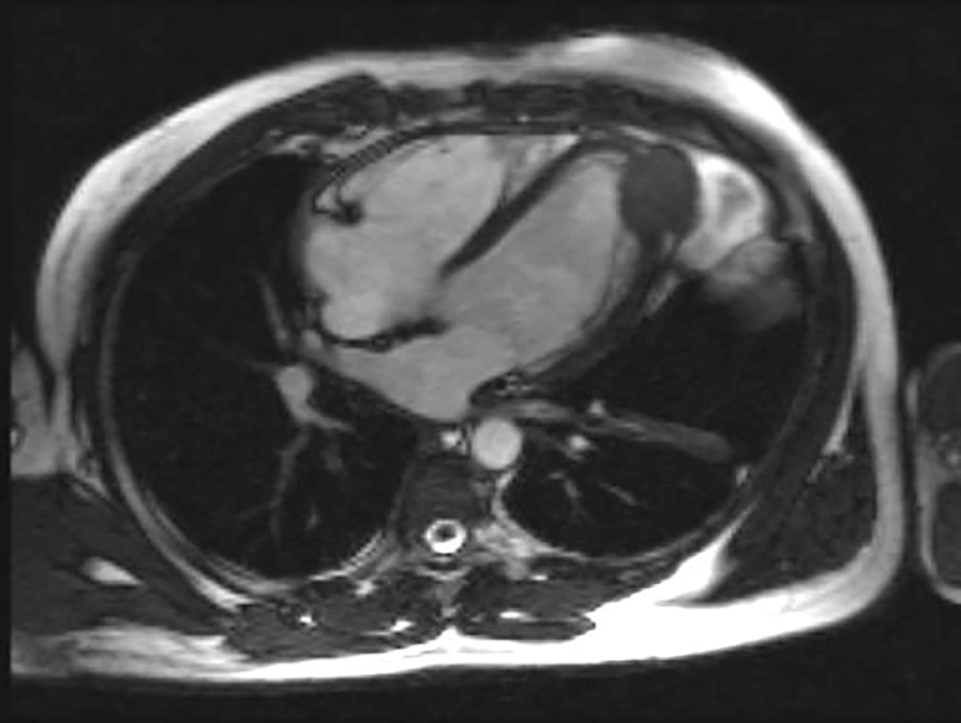
 | Figure 4. Cardiac NMR identified a nodular lesion and located it in the cardiac apex |
3. Discussion
- Chest pain is a common symptom, clinical history and systematic physical examination are fundamental to guide diagnostic strategy and patient management [1]. Pericardial diseases are relatively common in clinical practice and secondary metastatic tumors are a possible etiology of pericarditis [2]. Our patient presented with incessant pericarditis, defined as chest pain lasting for > 4 weeks [2]. He had typical ECG changes of pericarditis and elevation of inflammation markers. TTE was the crucial diagnostic test, enabling the documentation of an echogenic mass in the left ventricle, as a form of melanoma metastasis.Primary cardiac tumors are rare, and secondary tumors with cardiac involvement are more common and have a poor prognosis [3]. A particularly high incidence is observed in patients with preceding squamous cell lung carcinoma, urinary tract tumors and melanomas [4, 5].Melanoma is a tumor with poor prognosis, both for the precocity of oligosymptomatic metastatic disease and the frequency in which it affects the heart [6]. Metastatic melanomas to the heart have a high incidence, reaching 50% in post-mortem studies [3, 5], and may appear decades after the initial diagnosis of primary tumor [7]. The pericardium is often involved, followed by myocardium and endocardium [8]. In case of metastases, therapeutic options are limited due to diffuse involvement and poor response to chemotherapy [9].There are some aspects of this clinical case that makes it noteworthy. First the persistent chest pain due to incessant pericarditis mimicking stable angina pectoris. Although in pericarditis chest pain can irradiate to the arms like in our case, more frequently irradiates to one or both trapezius muscle, because the phrenic nerve that innervates these muscles traverses the pericardium. Moreover, it had none of the other typical characteristics of pericarditis: sudden in onset, pleuritic and exacerbated by inspiration [10]. Second the etiology of cardiac metastasis of melanoma with an atypical pattern; only one tumor located in the left ventricle apex. It is known that melanomas have high propensity to generalized hematogenous spread, and it is assumed that the right side of the heart is more frequently involved than the left, although in most cases diffuse bilateral spread is found [3]. When the left side is affected, the ventricular free wall and the ventricular septum are the most common sites for myocardial lesions [11]. Finally, the refractory chest pain that did not subside with the usual care. Despite the medical treatment has been properly implemented with NSAIDs and colchicine, it was not effective because this treatment works best in idiopathic or viral pericarditis [10]. In order to control pain, we initiate corticosteroids therapy. Although not the first line of treatment, corticosteroids have different anti-inflammatory properties of NSAIDs and should be considered as an alternative option, in selected cases [2, 12]. Even so, it was difficult to control symptoms, because pericarditis in this case had a secondary neoplastic cause. Target treatment at etiology is the key to success. Systemic chemotherapy or local radiotherapy can be effective. Invasive treatment is mostly confined to palliative measures. Pericardiectomy should be considered in patients with severe recurrent pericarditis that do not respond to adequate medical treatment. Surgical resection is only indicated in exception cases of solitary intracavitary heart metastasis [10]. Our patient had a lesion with intra and extra-cardiac components and lung infiltration, so the decision was to start chemotherapy. Nivolumab, an anti-programmed death 1 (PD-1) monoclonal antibody, is a relatively new drug and has shown longer progression free survival in patients with advanced melanoma [13]. In this type of complex patients, it is essential to involve a multidisciplinary team in the evaluation and treatment management.
4. Conclusions
- This case illustrates a common symptom, here associated with a dismal cause, where time to diagnosis is critical and treatment of the patient’s symptoms is sometimes challenging. In case of past malignancy it is imperative to consider cardiac metastasis. Cardio oncology liaison is important to achieve rapid prognosis assessment and tailored treatment management.
ACKNOWLEDGEMENTS
- No sources of funding were used to assist in preparation of this manuscript. The authors have no conflicts of interest that are directly relevant to the content of this review.