-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Journal of Health Science
p-ISSN: 2166-5966 e-ISSN: 2166-5990
2015; 5(3): 58-64
doi:10.5923/j.health.20150503.03
Epidemiological Study on Admissions and Discharges in the Surgical Intensive Care Unit of Misurata Central Hospital, Libya
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJune II A. Kiblasan 1, Ismail Mohamed Salah Alsakair 2, Mary Grace G. Villaruz 1, Gerilyn V. Briones 1, Ma. Daisery N. Garcia 1, Jane P. Fabian 3, Jersica P. Calderon 3
1Faculty of Nursing, Misurata University, Misurata, Libya
2Surgical Intensive Care Unit, Misurata Central Hospital, Misurata, Libya
3Faculty of Nursing, University of Tripoli, Tripoli, Libya
Correspondence to: June II A. Kiblasan , Faculty of Nursing, Misurata University, Misurata, Libya.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
A retrospective cohort design was applied in the accomplishment of this study to all patients admitted and discharged at the Surgical Intensive Care Unit (SICU) of Misurata Central Hospital, Misurata, Libya over a 7-months period (February – August 2011). This period marks the peak of revolution that made Libya chaotic. The purpose of this study is to describe the pattern of admission of patients into the SICU, stressing the reasons of patients’ admission and their discharge remarks. Most of the admitted patients in the SICU had gunshot wounds as the reason of admission and that they were transferred to other department of the health facility, in the surgical ward in particular as the top ranked discharge remark. Moreover, there is a strong relationship between the reasons of admission and the discharge remarks of patients. Despite of minimal number of health care professionals, equipment and supplies, nearly excellent performance was considered due to low mortality rate.
Keywords: Surgical Intensive Care Unit (SICU), Epidemiology, Admission, Discharges, Misurata Central Hospital, Libya
Cite this paper: June II A. Kiblasan, Ismail Mohamed Salah Alsakair, Mary Grace G. Villaruz, Gerilyn V. Briones, Ma. Daisery N. Garcia , Jane P. Fabian, Jersica P. Calderon, Epidemiological Study on Admissions and Discharges in the Surgical Intensive Care Unit of Misurata Central Hospital, Libya, Journal of Health Science, Vol. 5 No. 3, 2015, pp. 58-64. doi: 10.5923/j.health.20150503.03.
1. Introduction
- Recent advances and increasing complexity of modern medicine in patients with a high level of physiological compromise and significant co-morbidities led to the development of ICU during the last 50 years. [1, 2] However, this advancement in the care of critically ill patients has been associated with a huge increase in health expenditure. As health resources become increasingly constrained, it is imperative that efficient utilization of expensive resources such as intensive care becomes a priority and should be optimized without compromising the quality of care delivered to critically ill patient. [3] An intensive care unit (ICU) is a continuously busy ward in which critically ill patients are on life support treatment under intensive monitoring. Doctors, nurses and technicians vigilantly work on the patients and handle the life support equipment, pipeline and monitors. [4, 5] Intensive care is a kind of health care rendered to patients in a close monitoring and continuous treatment admitted in the intensive care unit (ICU), which is a specially equipped hospital unit that provides a highly specialized care to patients who suffer from severe and life-threatening illnesses and injuries supported by a special equipment in order to ensure normal bodily functions. This area in the hospital is also known as intensive therapy unit or intensive treatment unit (ITU) or critical care unit (CCU) that is staffed by highly trained doctors and nurses who are specialized in caring for seriously ill patients that made this to be distinguished from normal hospital wards by a higher staff-to-patient ratio and access to advanced medical resources. Common conditions that are treated within ICU include acute respiratory distress syndrome (ARDS), trauma, multiple organ failure and sepsis. [6] Patients may be transferred directly to an intensive care unit from an emergency department if required, or from a ward if they rapidly deteriorate, or immediately after surgery if the surgery is very invasive and the patient is at high risk of complications. [7]Usual diseases which are faced in the ICU concern the following: the confrontation and recovery of each type of shock, the acute respiratory failure, multiple trauma patients, and failure from various organic systems (cardiovascular, acute kidney failure, poisonings, environmental damage, serious infections, decay, chirurgical orthopedic / neurosurgical and urgent neurological incidents, post-surgical complications, heart operation, transplantations etc. [8]In relation to the intensive care rendered, it is a must to consider that the ICU is an ethically charged environment: life and death decisions are made daily, in acute, highly emotional situations that often involve legally incompetent patients and their family. Indeed, admission should be dependent on the ethics of ICU, particularly when medical criteria alone are insufficient in deciding what the right thing to do is. So far, little is known about the views of healthcare professionals involved in the case of a patient to be admitted. There is a dearth of research that includes all relevant perspectives – physicians and nurses from both the ICU and the general ward – and uses qualitative methods to explore these views in depth. Information about the attitudes of healthcare professionals about this process can be used to improve decision-making about resource allocation in intensive care. ICU can be considered as hospital in a hospital for its functions depend according to what type of illness and what particular health care a patient needs. This special unit in a hospital is distributed according to hospital department, Neonatal Intensive Care Unit for neonates, Pediatric Intensive Care Unit (pediatric patients), Maternal Intensive Care Unit (OB-Gyne), Medical Intensive Care Unit (medicine), and Surgical Intensive Care Unit (surgery). Admissions to Surgical Intensive Care Units (SICU) have great demands in terms of resources and with general desire in all fields of medicine in terms of auditing. ICU admissions are costly in human terms as well as resources. [9] Misurata Central Hospital is the biggest health care facility in Misurata, Libya with departmentalized health care service but due to some problems related to the building structure and its plan to construct much better systematized and centralized health system, departmental health services were distributed to smaller health care facilities owned by private proprietor or the local government in 2006. As the improvement started, here comes the revolution in the middle of February 2011 that brings the place into turmoil where plenty patients were catered. As such, it is the objective of this work to provide up-to-date information on admissions in the surgical intensive care unit from February to August 2011and what particular discharge remarks for those admitted patients after treatment.
2. Method
- A retrospective cohort design was employed in this study and was conducted in Misurata Central Hospital of Misurata, Libya. This health care facility is a departmentalized teaching hospital but has no specific ICU policy or protocol. The retroactive review included all admissions and discharges at the surgical intensive care unit from February to September 2011 purposely to identify what particular illness or health related problems are on top of the list during the peak of revolution. Descriptive statistical treatment to which frequency count or number (percentage) per illness or group of same/similar illnesses were tallied and ranked. Statistical Package for Social Sciences Version 20.0 (SPSS) employing Pearson product-moment correlation coefficient (PPMCC) was also used to test if there is significant relationship between the reasons of admission and discharge remarks of patients in the SICU.
3. Results
- Reasons for admission and the discharge remarks are the focus of this study. Over the period of data gathering, there were 524 admissions recorded and they had been monitored until discharged from the surgical intensive care unit. During the time of record review, there were 9 reported reasons of admission to the surgical intensive care unit based on physician’s initial assessment in which some were grouped according to organ or system affected as shown in figure 1. Generally, most of the admitted patients in the surgical intensive care unit was due to “gunshot wound” with 317 cases or 60.5% of the total admissions followed by post-surgery patients with 75 (14.31%). Traumatic injuries of other types garnered the third numerous patients with 45 cases or 8.59% of the total admissions and unidentified reasons of admission comes next with 75 cases or 5.92% of the total. Non-Surgical Intensive Care Unit cases were the fifth with 21 admissions which covers 4.01% of the total, then by emergency case with 18 or 3.44%. The third from the least numbered admission is burn with 8 cases or 1.53% followed by acute abdomen with 6 cases or 1.15% and lastly, hemorrhages with 3 or 0.57%.
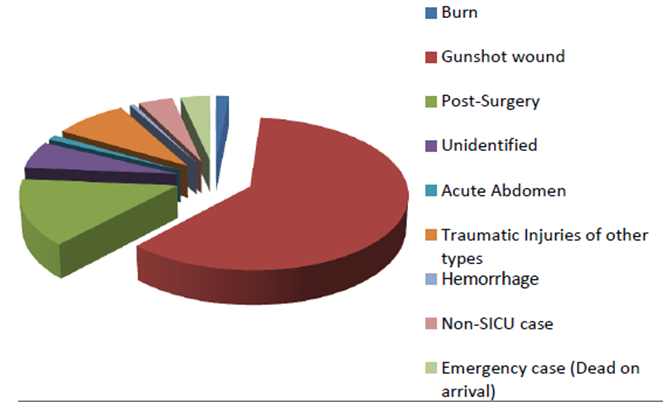 | Figure 1. Reasons of admission |
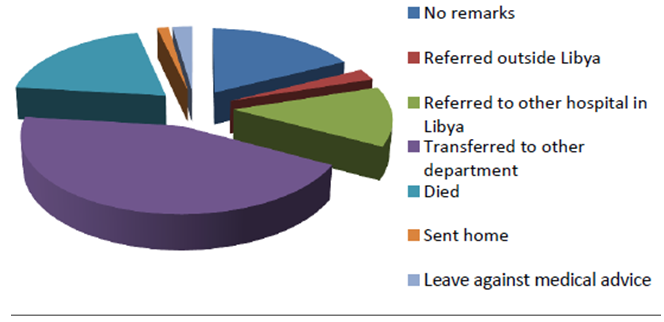 | Figure 2. Discharge remarks |
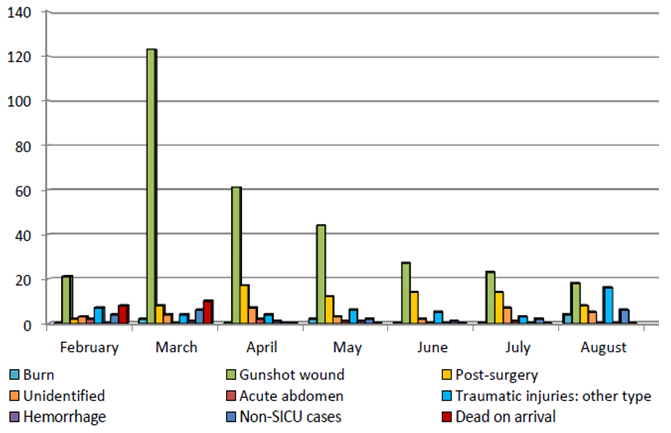 | Figure 3. Distribution of patients’ reasons of admission by month |
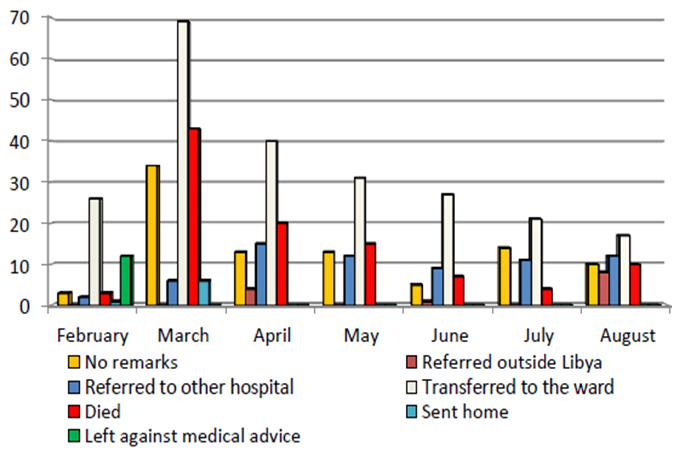 | Figure 4. Distribution of patients discharge remarks by month |
|
4. Discussion
- Epidemiology is a branch of medicine that deals with the incidence, distribution, and possible control of diseases. It is a mean of identifying the prevalence of health related problem for the purpose of planning actions to control such disease or illness in a manner that all cases can be catered. In the face of the increasing demand of intensive care services, as well as the high cost of such services, systematic steps must be undertaken in order to ensure optimal utilization of these resources. Admission to an intensive care facility is premised on the view that technologically advanced, competent care made available to the critically ill favorably influences the outcome of such illness. [10] The delivery of intensive care is an interventional treatment that is appropriate to a patient admitted to expect that there is reasonable likelihood of an acute, potentially reversible clinical condition that is likely to allow the patient to survive. With this, it was the goal of this study to provide up to date information on incidence and distribution of admissions in the SICU of Misurata Central Hospital and how admissions were discharged after management. It was in 2006 that the local government of Misurata, Libya planned to improve and expand the structure of its biggest hospital in the city. With this plan, the ministry of health of the local government distributed each department to nearby small private or government hospital in which SICU was temporarily transferred to Al Hikma polyclinic, an emergency and trauma health facility owned by private proprietor as sign of his dedication and loyalty to Libyans. The SICU has 4 beds and located near the emergency department with three Libyan and four foreign nurses. Ideally, 5-6 nurses are required per bed space. [11] Only one resident physician as the consultant was assigned at that time and the rest were all visiting. Initially, the facility has only 3 functional mechanical ventilators plus the portable one to make it four. With the composition of this facility, it is expected that there should be minimal numbers of patients being catered as per standard of intensive care units that the minimum ratio of nurse to patient should be one is to one together with additional nurses according to patient needs, training requirements, the total number of beds, and the geographical arrangements within the unit. [12] But during the revolution, the admissions exceeded to maximum number of patients to be catered. There were total of 524 admissions for 7 months that affects the whole structure and functions of the unit to which almost all admissions were males from the age bracket of 20 – 50 year old. Most of them are fighters who are trying to protect their families and their country as well. Other admissions if not fighter were victims of the chaotic situation that some are females, younger than twenty and beyond 50 year old. Taking into consideration the total admission, the standard operational protocol of this unit was not followed for the head of the department concentrated between life and death of incoming admissions. That even the patient’s length of stay was not recorded accurately due to turbulent flow-like scenario of the unit.Moreover, Gunshot wound, post-surgery and other traumatic injuries were the three leading causes of admission with 60.5%, 14.31% and 8.59% respectively. Gunshot wound outnumbered the other reasons of admissions because the period of record review was during the time that revolution is on its peak. Post-surgery referring to patients with major operation and complications such as post exploratory laparotomy, peritonitis and alike as the second on rank most likely similar but lower than the study where exploratory laparotomy constituted over half (59.9%) of post-operative admissions into the ICU. [13] Other traumatic injuries includes post fighting (war), fall down, stab wounds, due to explosion, head injury and road traffic accident constituted the third reasons of admission to the SICU. In this study, head injury due to road traffic accident was the common among the other traumatic injuries which is with similar finding but lower than the study that head injuries, accounting for 11.2% of ICU admissions in which all resulted from road traffic accidents. [13] The figure of this study is also much lower than the one recorded by Oyegunle et al [14] (73.4%) in a city that links major highways in South-Western Nigeria. With the study conducted in the United Kingdom, it was estimated that 7.6 of general surgical beds were occupied by head injury patients, despite considerable pressures on financial resources of these units. [15]. It is must and should not be taken for granted that people be aware the effect and complications of unsafe activities for it brings them at risk not only to physical but also to other types of injuries. It should be emphasized that head injuries are expensive and demanding in human terms and resources. [15] Trunkey [16] states that 50% of all individuals who die following civilian trauma do so within 30 minutes of the event, due to complex and severe injuries. In this study, there were admissions with reasons that are unidentified. This is maybe due to speedy manner of admissions as patients are flocking from time to time most especially in the month of March. On the other hand, there were admissions that are not suited to be admitted at the SICU. This includes cardiac related conditions (arrest of unknown origin, sinus ventricular tachycardia and myocardial infarction), hypoglycemia; gas poisoning; and respiratory related conditions (obstruction in the respiratory tract, chest pain, asthma attack, acute bronchitis and pneumothorax). Though this unit or department is meant to cater surgical patients, it is still the aim of a health care facility to cater health needs of clientele. With this and due to current situation (war) of the place and the medical intensive unit of the health facility is located a little bit far than the SICU, and for humanitarian reason, these classification of patients were accommodated. Dead on arrival (DOA) is quite unusual to be admitted in the surgical intensive care unit but should be accommodated in the emergency department initially then to the morgue but due to lack of staff nurses; lack of space; and insufficient equipment and supplies in the emergency department, some DOA patients were attended at the surgical intensive care unit which is just few steps from the emergency department. Furthermore, burn due to petrol or kerosene explosions was one of the reasons of admissions to the SICU which is analogous to a study that 26 cases of burns admitted to ICU where twenty two (84.6%) cases resulted from petrol or kerosene explosions, 3(11.5%) resulted from cooking gas explosion and 1(3.9%) from chemical burns. [13] In contrary, the pattern seen in the developed world where majority of burn injuries occur in the home and frequently involve children aged 1-5 years who are scalded by hot liquids. [17] Inhalation injury may occur in as many as 20% of patients admitted into burns centers. [18] Acute abdomen and hemorrhages were the rare admissions to the SICU. Acute abdomen in an instance that it is due to the complication of surgery done within 48 hours and hemorrhage is due to trauma. On the other hand, the process of discharge from critical care to less intensive levels of care or referrals to other hospitals and or outside the country for further management is important as the process for admission to critical care in which the patients should be discharged by consultant decision that is when clinically ready and appropriate at an appropriate time of day to an appropriate choice of clinical area and receiving/supervising medical team with full handover of clinical information. In this study, it is of good news though the facility is in great need for additional staff to cater the fluctuating patients for admission and at the same time admitted patient is for discharge because the most common discharge remark that was recorded is the patients were transferred to other department with 231 number or 44.08%. This signifies that no matter what factors that can affect the structure and function of the facility, available staff able to manage this tremendous scenario for the sake of human survival and health maintenance. This is in contrary with the study that early discharges from ICU contributed to high mortality rates [19, 20] however, this is congruent with the next on rank finding of this study in which 102 (19.47%) of the total discharges were dead. Furthermore, referrals of critically ill patients to other health care facility is inevitable most especially if the referring health facility is not capable to meet the health needs of critically ill patients though they are at high risk of morbidity and mortality during transport. In our study, it is supposedly not to be done due to the risk factors that may happen to critically ill patients to be referred but it is a need and should have to because of no available medical staff to furtherly manage the case, insufficient equipment and supplies, and no enough space to accommodate the fluctuating patients. These are the main reasons why sixty seven (67) or 12.79% of the discharged patients were referred to other hospital within Libya 13 or 2.48% were referred outside Libya. Leaving the hospital premise which is either conducive to the health of patient or not is a big deal need to be considered. The goal of a health facility is to treat or manage ill patients until recovery but because the request of family members and for the protection of the patients themselves, 12 (2.29%) of the discharged patients leave the health facility against medical advice and 7 (1.34%) discharged patient went home in favor of their health status.
5. Conclusions
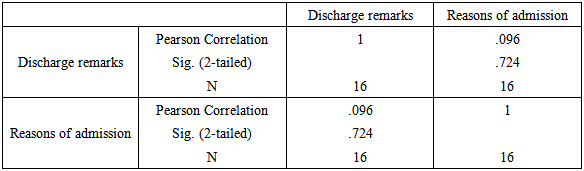
- Documentation is essential in monitoring status of such situation. It is important in a way that it provides necessary data for planning and other purposes. In this retrospective note, we have endeavored to consider aspects related to the reasons of admission and the discharge remarks of patients catered at the SICU of Misurata Central Hospital during the fracas in February to August 2011 at Misurata, Libya paying particular attention to the cause of admission, its outcome and the relationship in between. As per statistical survey that was carried and findings made on the admissions and discharges, The following conclusion were made: (1) Month of March, April and May have the highest admissions to the SICU respectively; (2) The three most common reasons on admission to the SICU are gunshot wound, post-surgery and traumatic injuries that is all related to the present situation of Libya; (3) Endorsing patient to other department in the hospital is the common discharge remark then referral to other health facility within Libya and to the other country; (4) There is strong relationship between the reasons of admission and the discharge remarks of the patients; and (5) Though minimal number of health professionals were assigned in this area, it is considered that the performance of the whole department is nearly excellent due to its low mortality rate.