-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Journal of Health Science
p-ISSN: 2166-5966 e-ISSN: 2166-5990
2015; 5(1): 18-23
doi:10.5923/j.health.20150501.04
Comparison of Body Fat Percentages in Nigerian Obese Females Using Field Methods
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAntoninus O. Ezeukwu 1, Chioma G. Ezeoranu 1, Afamefuna V. Egwuonwu 2, Uche M. Ugwoke 3, Nelson E. Ekechukwu 1, Maduabuchukwu J. Nwankwo 2
1Department of Medical Rehabilitation, University of Nigeria, Enugu Campus, Nigeria
2Department of Medical Rehabilitation, Nnamdi Azikiwe University, Nnewi Campus, Nigeria
3Department of Community Medicine, Nnamdi Azikiwe University Teaching Hospital, Nnewi, Nigeria
Correspondence to: Antoninus O. Ezeukwu , Department of Medical Rehabilitation, University of Nigeria, Enugu Campus, Nigeria.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Objective: Assessment of correlation and agreement among three different field methods of determining Percent Body Fat (PBF) in obese University females. Methods: Convenience and snowball sampling technique were used to recruit 30 obese females for the study. PBF were obtained from each participant using three field methods of bioelectric impedance analysis (BIA), skinfold calliper (SC) and body adiposity index (BAI) respectively. Data were analysed using Pearson correlation, independent t-test and Bland-Altman plot. Alpha level was set at 0.05. Results: There was no significant relationship (r=0.376; p=0.30) between methods of assessing percentage body fat using SC and BIA. There was significant relationship (r=0.196; p=0.041) between BAI and BIA methods of assessing percentage body fat. There was no significant relationship in the results obtained between each of the other methods and skinfold calliper. Conclusions: There was a poor level of agreement amongst the methods despite the evidence or lack of relationships.
Keywords: Bland-altman, Percent fat, Field, Obese, Females
Cite this paper: Antoninus O. Ezeukwu , Chioma G. Ezeoranu , Afamefuna V. Egwuonwu , Uche M. Ugwoke , Nelson E. Ekechukwu , Maduabuchukwu J. Nwankwo , Comparison of Body Fat Percentages in Nigerian Obese Females Using Field Methods, Journal of Health Science, Vol. 5 No. 1, 2015, pp. 18-23. doi: 10.5923/j.health.20150501.04.
Article Outline
1. Introduction
- WHO [1] has identified the transition from high school to college as a critical period for the development of obesity. The rate of obesity for females is reported to be five times higher than that of males in developing countries [2, 3]. Recent evidence shows that nutritional, lifestyle and socioeconomic transitions are occurring in many developing countries [4] and participation in exercise is known to decrease significantly between adolescence and adulthood, the age range of most University students [5, 6]. Consequent upon this is an increasing craves for junk food among young females and a superimposition of less physically active lifestyle to meet the changing socioeconomic challenges. Recent intermittent public health education campaigns warning of the health consequences of excess weight have created concerns on the health risks of obesity among female students. Percent body fat (%BF) rather than amount of excess weight is known to determine the health risks of obesity [7] and is a useful indicator for optimum health and physical fitness in health and disease state. Many females now want to regularly know their percent body fat. This has created dilemma of accuracy and feasibility of percent body fat measurements as most measurements taken in this environment use the field methods. The importance of accurate assessment of percent body fat in monitoring obesity class, nutritional status, training performance and health status has a pivotal role in sports/exercise science and public health issues [8]. Exercise scientists and public health professionals have continued to endeavour to assess this parameter in the most accurate methods peculiar to the populations of interest. Generally, there are laboratory and field methods of measuring percent body fat. Field method enjoys the advantage of safe, non-invasiveness and speed of administration when compared to laboratory methods [9]. Many laboratory methods of assessing body fat percentage are sophisticated and only suitable for the research [10]. The accuracy of these measurements can have far reaching implications on research findings and public health policies on percent body fat measurements in obese females, as there has been controversy over the methods of assessing percentage body fat [11].Many laboratory methods of assessing body fat are sophisticated and usually suitable for the research setting [10]. For purposes of cost, most researchers in developing countries have accessibility to field methods. For cosmetic and beauty reasons, female population in the society tend to seek assessments of their percent body fat frequently in this environment. Most of the field methods usually used are skinfold calliper [12], body adiposity index [13] and bioelectric impedance analysis [14]. These devices have been used frequently despite dearth of researches establishing their levels of relationship and agreements in obese females, hence, the need for the present study. The study aimed at comparing the relationship and levels of agreement among bioelectrical impedance analysis (BIA), skinfold calliper (SC) and body adiposity index (BAI) methods of assessing percentage body fat of Nigerian young obese females.
2. Methods
2.1. Participants
- The study involved 30 obese (BMI≥30 kg/m2) female students of University of Nigeria, Enugu campus, aged 18-35 years. Convenience and snowball sampling technique was used to recruit the participants.
2.2. Instruments
- 1. Stadiometer- A calibrated long wooden ruler with a flat wooden base in which the subject climbed barefooted, was used to determine the subject’s height measured in cm. 2. Body fat monitor/hydration monitor scale (Model: 7032497) was used for foot-to-foot bioelectrical impedance analysis of percent body fat. It was also used to measure the weight of the participants.3. Lange skin fold calliper (Cambridge Scientific Industries, Cambridge, MD): was used to assess the percent body fat using the three-site skinfold thickness method for females as described below.4. Inelastic Tape measure was used to take girth measurements
2.3. Procedure for Data Collection
- This study employed a cross sectional study research design. Ethical approval was sought and obtained from the Institutional Ethical Committee before commencement of the study. Informed consent of the participants was obtained before commencement of data collection. Weight of the participants were measured in kilograms with the subject standing bare feet with minimal clothing and with their pockets free of objects that might add to their weights such as mobile phones, purse, keys and rings. The reading was taken over the weighing scale from the centre point to avoid error due to parallax. The subject’s height was taken from a stadiometer, subjects were barefooted and without headgear or cap standing against the stadiometer with the heels, gluteus and occiput touching it. A pointer was firmly pressed against the scalp and was read off on the stadiometer in centimetres. This was converted to the nearest metre by dividing with 100.Three different clinicians competent in anthropometric measurements were involved in the measurement of the respective %BF. They were blinded to the purpose of the study. The foot-to-foot bioelectric impedance measurement was done by setting the parameters of the individual on the automated bioelectric impedance analysing machine scale while the participant stood on it and the level of percentage body fat, muscle mass, muscle mass and hydration percent was shown on the screen. The body adiposity index was obtained by using the following formula [13]: BAI = (hip circumference in centimetres / (height in metres)1.5 - 18. Percent fat using the skinfold calliper was obtained using the three-site formula (triceps, suprailiac, abdominal) method [15]: Body density = 1.089733 - 0.0009245 (sum of three skinfolds) + 0.0000025 (sum of three skinfolds)2 - 0.0000979 (age). Population-Specific Formula for black females was used for conversion of Body Density (Db) to Percent Body Fat [15, 16]: (4.85/Db)–4.39. All measurements were taken after a 12 hour fast and no particular order was observed in taking the measurements. Percent fat measurements were taken thrice and the average of the 3 readings for the particular method (provided <1% difference) was recorded.
2.4. Data Analysis
- Statistical analysis was performed using SPSS (Version 15) and Analyse-it software. Values were reported as mean ± standard deviation. Pearson Correlation was done to determine the relationship among the methods. Independent t-test was used to compare the means of the groups. Bland-Altman analysis was used to determine absolute limits of agreement between the percentage body fat assessed by skin fold calliper method, bioelectric impedance analysis method and body adiposity index method. α level of p<0.05 was considered statistically significant.
3. Results
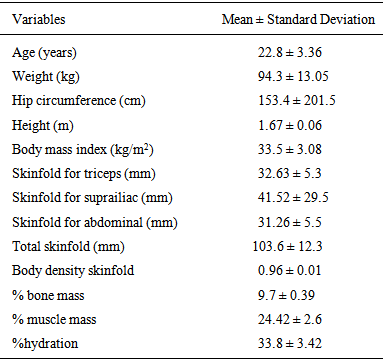
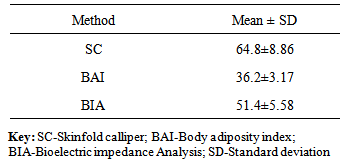
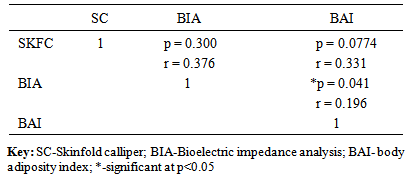
- Table 1 showed the anthropometric characteristics of the participants. The weight and body mass index of obese females were 94.3±13.05kg and 33.5±3.08kg/m2 respectively. There is an outlier as found in the hip circumference of obese females (153.4 ± 201.55cm). Table 2 showed that the least mean % body fat (36.2%) was measured by BAI. Percent body fat measured by BIA was 51.4±5.58% and the highest %BF (64.8±8.86%) was measured by SC. Table 3 shows that there is statistically significant relationship (r=0.196; p=0.041) between %BF measured using BAI and BIA in obese females. There was no significant relationship (r=0.331; p=0.0774), in percent body fat measured between skinfold caliper and body adiposity index methods. There was no significant relationship in %BF between SC and BIA (r=0.376; p=0.300).
|
|
|
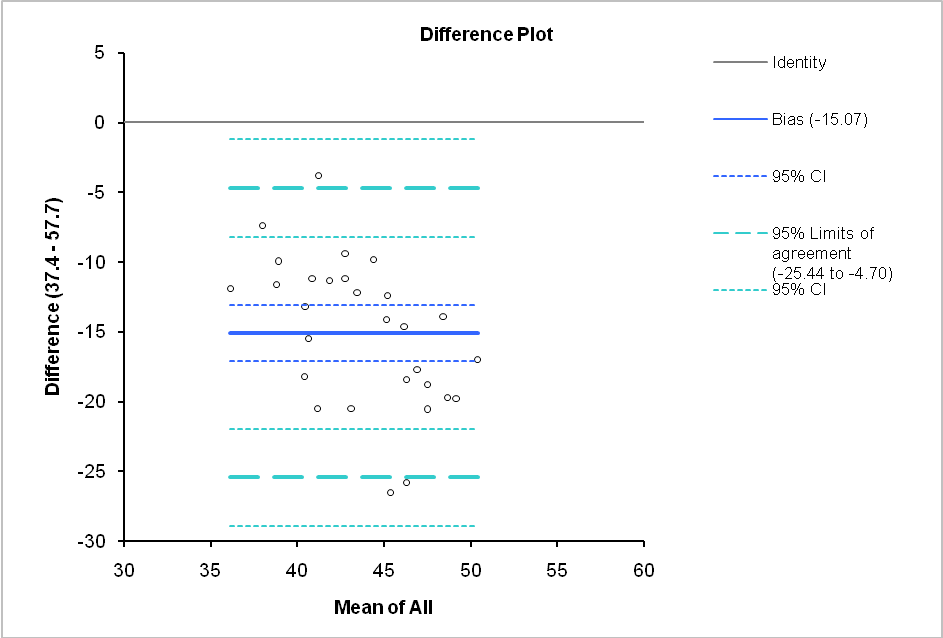
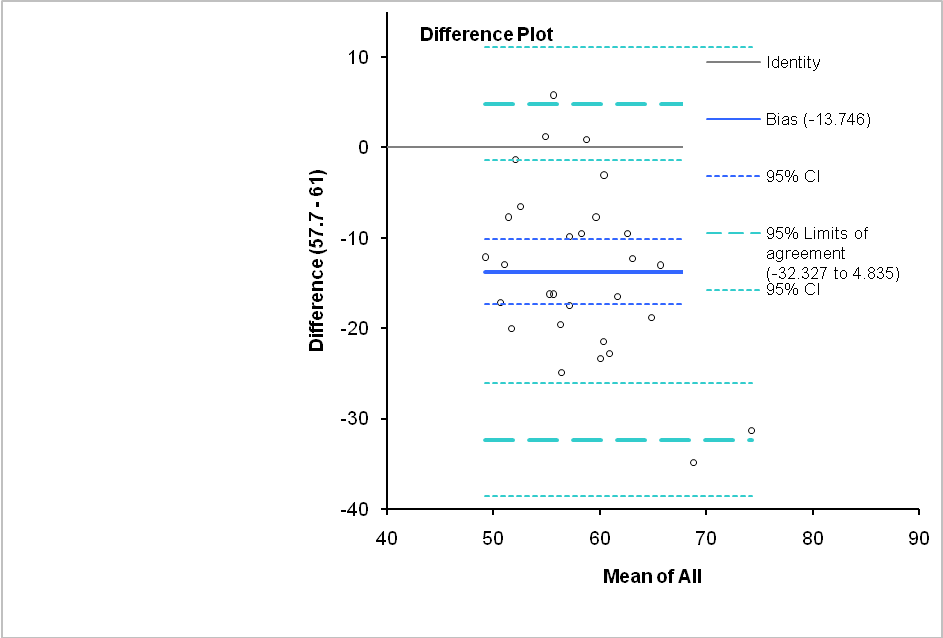 | Figure 1. Bland-Altman plot showing the limits of agreement between BIA and SC methods of assessing percent body fat in obese females |
 | Figure 2. Bland-Altman plot showing the limits of agreement between BIA and BAI methods of assessing percent body fat in obese females |
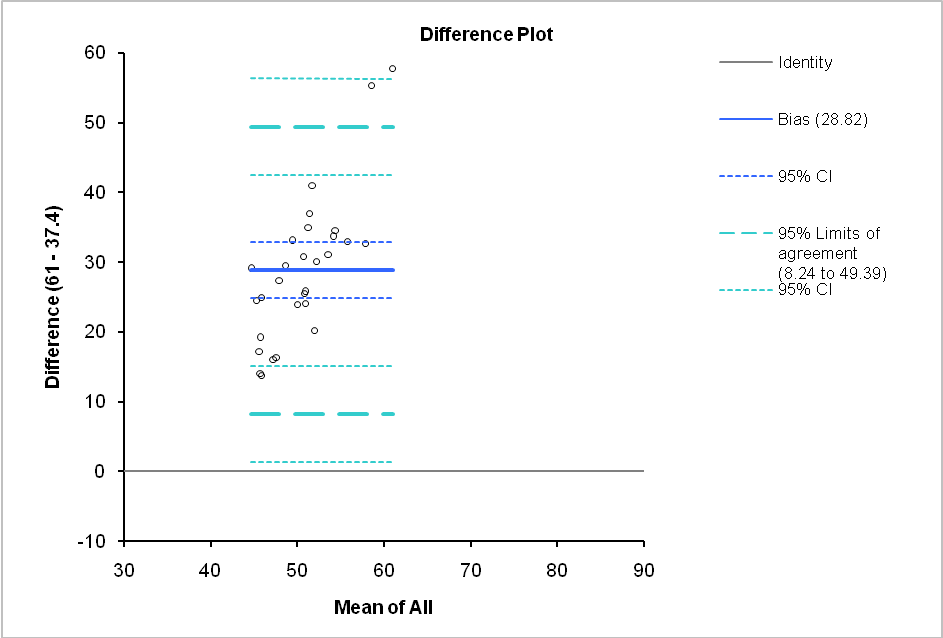 | Figure 3. Bland-Altman plot showing the limits of agreement between SC and BAI methods of assessing percent body fat in obese females |
4. Discussion
- This study investigated the relationships and levels of agreement of percent body fat obtained using three different field methods among Nigerian obese undergraduate females. The findings showed that there is no relative agreement between skin calliper methods and the results obtained using each of the other methods. This was indicated by no significant relationship between the readings obtained by the skin calliper and each of the other methods. However, the BAI showed weak agreement with BIA. These findings are not in agreement with McNeil et al [17] who reported that the skinfold thickness method was as good as the bioelectric impedance analysis in lean and overweight groups of women. However, when compared with laboratory methods BIA have been shown to underestimate percent body fat in overweight and obese women [18, 19].The findings also showed that, in absolute terms all the methods had wide limits of agreement between them. Skin fold calliper method overestimated percent fat by 13.75% when compared to bioelectric impedance analysis. Similar studies in other populations have reported conflicting results. Some authors suggest that BIA is preferable over skinfold caliper due to the ability of evaluating hydration status and minor inter-operator error [20]. Valerio et al [21] suggested that BIA may not be suitable for measurement of body composition in overweight and obese women. Skin Fold measurement is argued to be suitable for population, but difficult to get reliable measurements with obese people [22]. The practice of using the skinfold method has previously been discouraged in obese individuals [23]. These suggestions necessitate caution in interpreting the findings of the present study, as the models of instruments used in this study were not the same with those used in the researches mentioned. It is possible that other inter and/or intra participant/researcher factors may have influenced the findings of this study. Williams [24] suggested that other unexplained variance in percent fat readings may be due to a reduced reliance of the method on the assumptions of fat distribution. Findings of the present study show that bioelectric impedance analysis of percent body fat overestimated that of body adiposity by 15.07%. Maria et al [25] suggests that BAI estimates body fat with higher accuracy than for anthropometric measures and bioelectric impedance analysis. Skin calliper method overestimated body adiposity method by 28.8%. Lohman [26] considered an error of 4% points of body fat percent as reasonable. This may suggest the need to validate field methods commonly used in this environment with other laboratory criterion measures of percent fat measurement.The findings of this study suggests that in the use of these methods of measuring percent fat, clinicians/exercise scientist should be consistent in their reporting of methods or equipment used to avoid wrong interpretation of findings. There may be a need for professional bodies involved in percent fat measurements to declare positions statements on best practices peculiar to the ethnic and individual characteristics of our environment. It may also necessitate the need for regression equations to correct for any such inter/intra individual or equipment differences peculiar to the locality.The main strength of this study is that, apart from highlighting the relative and absolute levels of agreement among commonly used field methods of percent fat in our environment, it has stressed the need for caution in the interpretation of findings of similar studies as there may be peculiar unexplored difference in population studied. A limitation of the study is the non-comparison with laboratory criterion measures of percent fat analysis. The findings of this study should also be interpreted with caution as it may not be generalised to other models of the devices used.
5. Conclusions
- Percentage fat of obese females obtained using bioelectric impedance analysis correlated significantly with that obtained using body adiposity index. No significant correlation was observed between the other methods. There is weak level of agreement among the various field methods of accessing percent fat commonly used in this environment. There is need to replicate this study among obese females in the general population involving larger samples. There may also be need for position statements by relevant bodies based on research evidence among these populations to guide clinicians/exercise scientists in making more accurate computations of percent fat peculiar to the locality.
ACKNOWLEDGEMENTS
- The authors appreciate the assistance of staff of the Laboratory unit, Department of Medical Rehabilitation, UNEC.