-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Journal of Health Science
p-ISSN: 2166-5966 e-ISSN: 2166-5990
2015; 5(1): 6-10
doi:10.5923/j.health.20150501.02
Of What Value is Screening for Hypertension in Ophthalmic Practice?
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLIyiade A. Ajayi 1, Ebenezer A. Ajayi 2, Olusola J. Omotoye 1, Kayode O. Ajite 1, Christianah O. Fadamiro 1
1Ophthalmology Department, Ekiti State University Teaching Hospital, Ado-Ekiti, Nigeria
2Medicine Department, Ekiti State University Teaching Hospital, Ado-Ekiti, Nigeria
Correspondence to: Ebenezer A. Ajayi , Medicine Department, Ekiti State University Teaching Hospital, Ado-Ekiti, Nigeria.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
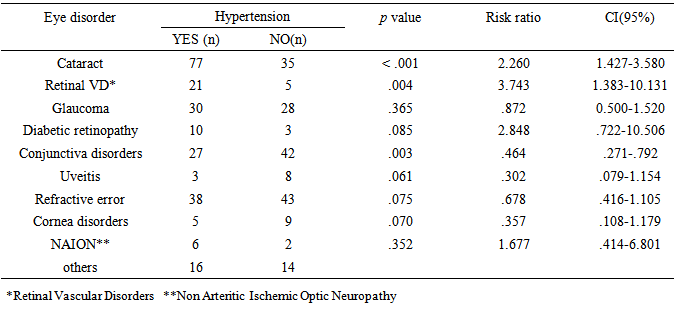
Background: Hypertension is a non-communicable disease with an increasing burden in the developing countries where low awareness rate is a major determinant of widespread gaps in its treatment and control. We carried out this opportunistic screening survey at the eye clinic of the Ekiti State University Teaching Hospital Ado Ekiti, in southwest Nigeria. All consecutive adult new patients seen in the clinic were recruited into the study. A questionnaire was administered to all the patients after obtaining a verbal consent to document participants’ bio-data and historical clinical information related to hypertension. Data were entered into SPSS version 20 and analysed. Results: The respondents whose ages ranged between 18years and 95years with a mean of 54.2 ± 18.2years had a male to female ratio of 3.5:5. The systolic blood pressure ranged between 90-240mmHg while the diastolic blood pressure ranged between 40-160mmHg. Blood pressure in the hypertensive range was observed in 54.9% of the study population. Suboptimal blood pressure control was observed in 72% of those who had been previously diagnosed hypertensive before their eye clinic visit. Cataract (RR 2.26), retinal vascular disorders (RR 3.74), diabetic retinopathy (RR 2.85) and non arteritic ischemic optic atrophy (RR 1.68) were found to have a higher risk of occurrence among the hypertensive subjects. Twenty four percent (24%) of the respondents could not recollect ever having blood pressure checked all their lifetime preceding their visit to the eye clinic. Conclusion: The visually disabling nature of eye disorders and the increased probability of seeking assistance in an eye care facility provide a unique avenue for picking previously undiagnosed hypertensive by routine blood pressure check and detecting patients with poor routine check practices and suboptimal BP control during eye care service delivery.
Keywords: Blood pressure check, Undiagnosed hypertension, Eye clinic
Cite this paper: Iyiade A. Ajayi , Ebenezer A. Ajayi , Olusola J. Omotoye , Kayode O. Ajite , Christianah O. Fadamiro , Of What Value is Screening for Hypertension in Ophthalmic Practice?, Journal of Health Science, Vol. 5 No. 1, 2015, pp. 6-10. doi: 10.5923/j.health.20150501.02.
1. Introduction
- Hypertension is a non communicable disease with increasingly important medical and public health implications. [1] It is a major cause of morbidity and mortality among Nigerians with an age adjusted prevalence of 14.5%. [2] It has been ranked the first among cardiovascular diseases with its complications constituting 25% of emergency medical admission in urban hospitals according to the report of a multicentre study in Nigeria. [3] It has also been found to be responsible for an estimated 45% of deaths due to heart disease and 51% of deaths due to stroke globally. [4] In the United States approximately 30% of adults have been reported to be unaware of their hypertension, 40% of individuals with hypertension are not on treatment and 2/3rd of hypertensive patients are not being controlled to BP levels <140/90mmHg. [4] A far less level of detection, treatment and control of hypertension have been reported in Sub-saharan Africa [5] and Nigeria [6] when compared with the results obtained in developed countries with consequent widespread gaps in hypertension treatment and control. Routine opportunistic screening for hypertension in formal medical setting such as the ophthalmic practice may provide reliable way to increase hypertension awareness and detection rate. This is because hypertensives have been reported to be at greater risk of certain eye diseases largely retinal vein occlusion, retinal artery occlusion; modestly glaucoma, retinal detachment, age related macular degeneration, and even cataract. [7] This could suggest that patients with high blood pressure may pass through the eye clinic at one point in time or the other in view of the visually disabling nature of some eye conditions. We therefore decided to carry out this survey to determine the blood pressure pattern and prevalence of newly diagnosed hypertension among first-time eye patients as well as the pattern of eye disorders in those with abnormal blood pressure. We are not aware of any of such study in our practice area so far. The result of this study may help us to know if routine check of blood pressure among eye patients is indeed of any value in the detection of hypertension and perhaps secondary prevention of potential complications of this condition by early referral of patients to the internists.
2. Main Body
- Materials and methodsA survey observational study was carried out between February and June 2014 at the Ophthalmology Department of the Ekiti State University Teaching Hospital Ado Ekiti in Southwestern Nigeria. The authors observed that blood pressure check was a routine practice by the nurses at the department for all first time patients, old patients who required surgeries and other patients on request from the managing eye-care givers. We therefore decided to carry out this study to find out the benefits derivable from this procedure in order to determine if there were evidences to justify this practice. Every consecutive consenting first time adult eye patients were included in the study. All patients had their blood pressure and visual acuity checked according to standard practice by the ophthalmic nurses after they had registered to be seen in the eye clinic. A pre-tested questionnaire was administered to each patient while being seen by the attending Consultants. Information elicited from the questionnaire included the demographic characteristics, blood pressure(BP) at first eye visit, practice of routine BP check, past history of hypertension, duration of hypertension and use of antihypertensive as well as regularity on drugs. Final eye diagnosis was also recorded. Patients who were found to have hypertension (defined as previous physician diagnosis of hypertension or systolic blood pressure (SBP) of ≥140 mmHg and/or diastolic blood pressure (DBP) ≥90 mmHg for adults 18years and older) [4] were referred for further evaluation and treatment by the Physician. In the case of patients with diabetes and nephropathy the cut off for diagnosis and referral was set at 130/80mmHg [4]. Patients whose ages were below 18years were excluded from the study. All patients who were follow up eye patients of the department were also excluded from the study. Data was entered and analysed for simple frequency using SPSS (Statistical Package for Social Science) version 20. Mean and Standard deviation were obtained for categorical variables while the chi square test was utilized for intergroup frequencies with p<0.05 considered statistically significant.
3. Results
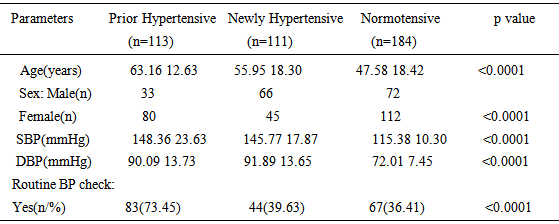
- A total of 408 patients were included in this study. The age range was between 18years and 95years with a mean of 54.2 ± 18.2 years. Females were 245(58.3%) and males were 175(41.7%) with a male to female ratio of 7:10. Figure 1 shows that a large percentage (83.6%) had varying levels of formal education while 67(16.4%) had no formal education.
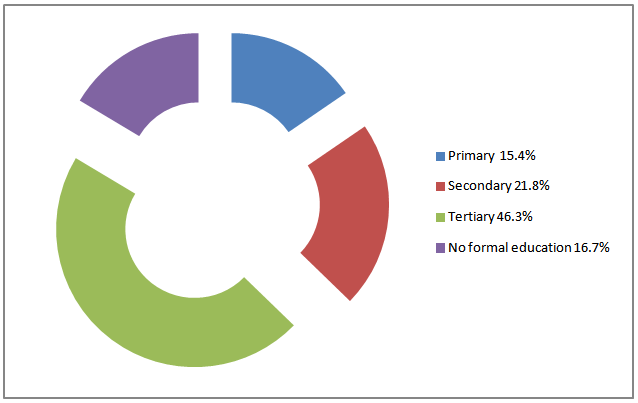 | Figure 1. Educational Status of Respondent |
|
|
|
4. Discussion
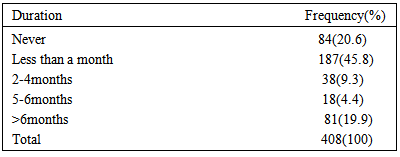
- Hypertension is the commonest non communicable disease in Nigeria with over 4.3million Nigerians above age 15years classified as being hypertensive. [8] Hypertension is mostly asymptomatic except there are symptoms of target organ complications of hypertension like stroke, renal failure, retinopathy among others. On the other hand patients with ocular challenges are likely to present to an eye clinic either because of the visually disabling nature of eye disorders or due to the cosmetic blemish that could result from some eye abnormalities.Majority of the respondents in this study are either elderly or adults in the working age group considering the mean age of the study population. This suggests that the respondents are a likely appropriate group for this kind of study. There were more females than males among the respondents. The reason for this could be because of the previous observations that women are more likely to seek eyecare than men. [9, 10]In this study, more than half of the patients had abnormal blood pressure with a little more than a quarter (27.7%) being previously known hypertensive. This large number of patients with high blood pressure may not be unrelated to the mean age of our study population. In Nigeria, as in most parts of the world, the most likely determinant of blood pressure and presence of high blood pressure is age. Blood pressure has been shown to increase steadily with age from the youngest to the oldest age brackets, irrespective of gender. It was observed in this study that blood pressure control among those previously known to be hypertensive was poor as about 72% had suboptimal blood pressure control. This is despite the fact that about two-third of them claimed to use their antihypertensive medications as prescribed. Previous reports from Nigeria and other parts of the world showed that most people with hypertension are not effectively treated and controlled to the recommended blood pressure targets [11, 12].The newly diagnosed hypertensives in this opportunistic screening survey were almost of equal proportion to that of the previously diagnosed hypertensives. This is synonymous to those who were unaware that they had high blood pressure. As in many populations of the world, the awareness of hypertension is low in Nigeria. In some studies, the reported awareness rates were 14.2% in rural areas by Oladapo et al [13], 29.4% and 30.0% in semi-urban and urban populations [14, 15]. One way to improve the awareness rate of hypertension among the populace is through opportunistic screening like this one: screening that occurs in places where large population of patients is expected. This allows for continuous exercise. The cooperative manner in which these patients have been handled by their referral to the hypertension clinic of the hospital should also be encouraged to add values to the obvious benefits of this type of screening. We observed that less than half of the screened population had a regular frequency of checking their blood pressure. More worrisome is that a fifth had never had their blood pressure checked prior to coming to this eye facility. It is important to educate the populace on the importance of regular blood pressure check to improve blood pressure awareness. Additionally, hypertensives have been reported to be at increased risk of certain eye diseases. The proposed mechanisms for this include hemodynamic injury and /or cellular actions induced by hypertension-related hormones or growth factors [16]. Cataract had a high risk of occurrence among hypertensives in our study similar to a finding of a study in Ghana where 10.4% of self reported cataract patients were found to have hypertension [17]. From this study the greater occurrence of retinal vascular disorders like retinal vein occlusion and branch retinal vein occlusion among hypertensive subjects is in agreement with reports from various studies [18-20].Hypertension has also been found to be a risk factor for some eye diseases like diabetic retinopathy and age related macular degeneration [16]. Diabetic retinopathy was found to be higher in occurrence among the hypertensive subjects in this study. Thupa et al [21] in a study done in Nepal had similarly reported increased risk of incidence and progression of diabetic retinopathy among hypertensive- diabetics. An increased risk of non-arteritic anterior ischemic optic neuropathy was observed among the hypertensive subjects in this study. Hypertension has been reported to be the commonest vascular risk factor for non-arteritic anterior ischemic optic neuropathy [22]. For instance, hypertension was found to be one of the main systemic risk factors accounting for 55.5% of cases with non-arteritic anterior ischemic optic neuropathy in a study in Malaysia [23].Other eye disorders found among the patients in this study were refractive error, uveitis, glaucoma, cornea disorder and allergic conjunctivitis. These did not have higher risk of occurrence in hypertensives in this study. Cataract has remained the world’s leading cause of blindness. [24, 25] Diabetic retinopathy and retinal vascular disorders have also been found to have an increasing trend in the developing countries. The visually disabling nature of these eye disorders, the characteristic peak age of incidence and the increased probability of seeking assistance in an eye care facility provide a unique avenue for picking previously undiagnosed hypertensives by routine blood pressure check among patients who present at the facility. Patients with poor routine check practices and suboptimal BP control can also be picked during eye care service delivery.