-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Journal of Health Science
p-ISSN: 2166-5966 e-ISSN: 2166-5990
2015; 5(1): 1-5
doi:10.5923/j.health.20150501.01
An Evidence of Socio-Demographic Effects on Child’s Diarrhoea in Bangladesh
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMd. Rafiqul Islam , Md. Kamal Hossain , Md. Nuruzzaman Khan , Md. Raihan Ali
Department of Population Science and Human Resource Development, University of Rajshahi, Bangladesh
Correspondence to: Md. Rafiqul Islam , Department of Population Science and Human Resource Development, University of Rajshahi, Bangladesh.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
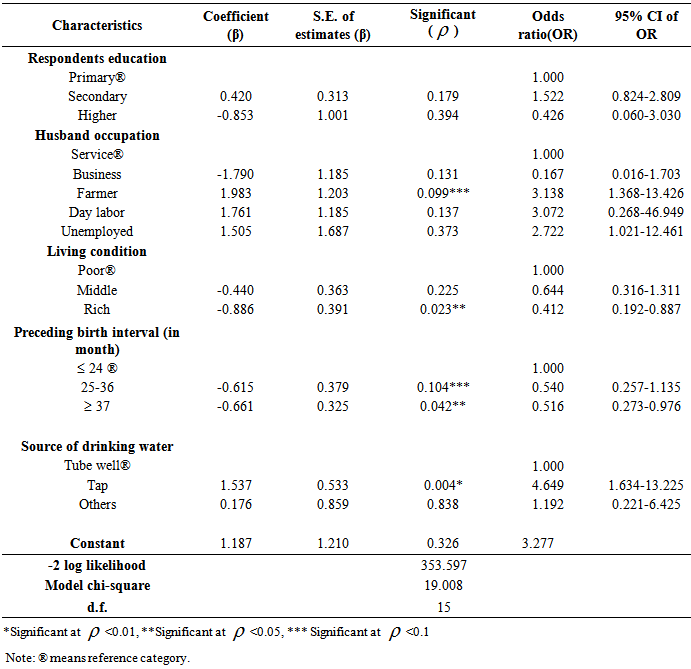
Background: Children are the most vulnerable and high risk group in the prevalence of diarrhea in low income countries like Bangladesh. This can lead to the higher rate of child morbidity and mortality. Achievement of Millennium Development Goal’s (MDGs) at a target period, it is important to comprise the issue first. Therefore, the purpose of the present study is to find out the risk factors of diarrhea in the childhood. Methods: Data and necessary information of 485 women were obtained from the Bangladesh Demographic and Health Survey (BDHS), 2007. These 485 women were extracted from 10,996 women whose children had experienced an episode of diarrhea in the two weeks before the survey. The chi-square test and binary logistic regression analyses have been used as the statistical tools. Results: Majority of the women (76.9%) reported their child had experienced diarrhea in the last two weeks. Respondent’s educational level, husband occupation, living condition, birth interval and the sources of drinking water were found to be significantly associated (p<0.05) with the disease of diarrhea. Finally, binary logistic model identified that respondents’ husband occupation, their living condition, birth interval and the source of drinking water were significant factors. Conclusions: The prevalence of diarrhea disease is more common in Bangladeshi children. So, it is necessary to educate general people about the possible living arrangements for avoiding diarrhea and its termination.
Keywords: Diarrhoea, Children, Morbidity, Binary logistic model, Bangladesh
Cite this paper: Md. Rafiqul Islam , Md. Kamal Hossain , Md. Nuruzzaman Khan , Md. Raihan Ali , An Evidence of Socio-Demographic Effects on Child’s Diarrhoea in Bangladesh, Journal of Health Science, Vol. 5 No. 1, 2015, pp. 1-5. doi: 10.5923/j.health.20150501.01.
Article Outline
1. Introduction
- Diarrhoea is the passage of three or more loose or liquid stools per day from the body of human. It is usually a symptom of gastrointestinal infection and entero toxigenic Escherichia coli (ETEC), Shigella, Salmonella, and Campylobacter bacteria have been reported as a causative agent [1, 2]. It can be recognized by four clinical features, each reflecting the basic underlying pathology and altered physiology. These clinical features are acute watery diarrhoea, acute bloody diarrhoea, persistent diarrhoea and diarrhoea with severe malnutrition of which 50% of worldwide cases of the condition present with watery diarrhoea [3, 4]. Approximately, 35% are persistent diarrhoea and 15% dysentery diarrhoea with blood stains [5]. It is one of the major factors that contribute significantly to high child morbidity and mortality in the world. Annually, there are about two billion cases of diarrheal disease worldwide and 1.9 million children younger than 5 years of age suffer from diarrhea each year, mostly in developing countries [3]. More than 5000 children are dying every day as a result of diarrheal diseases [6]. It is well known that diarrhoeal disease is one of the leading causes of illness and death in children in Bangladesh. One third of the total child death and an average of 4.6 children suffers in rural areas from which 2,30,000 children death due to diarrhea in each year of Bangladesh [7].Insufficient facility of safe drinking water, sanitation and hygiene, as well as poorer overall health and nutritional status in Bangladesh lead to the more prevalence of Diarrhoea. According to the latest available figures, an estimated 2.5 million people lack improved sanitation facilities, and nearly one million people do not have access to safe drinking water [8]. These unsanitary environments allow diarrhoea-causing pathogens to spread more easily [9]. Although food contamination is another major route for the transmission of diarrhea especially, under the hygienic conditions prevailing in a rural setting [1]. Various studies reported that the source of diarrhoea transmission was either water or food [10]. Children are the leader of the future and their growth and development has strong reflection on the future of a country [11]. But, they are considered as the most vulnerable worldwide because they are prone to common illnesses and are likely to get repeated infections due to their weak immune systems. Their health care considered as the integral part of a country’s overall development and health system. This awareness had reflected the large number of growing researches in the country [12-14]. An improvement of child health and reduce mortality under five children in Bangladesh are more important for the fulfillment of MDGs. This issue can lead the researchers to identify as well as what factors are associated with child morbidity and mortality due to diarrhoeal epidemic. This study also helps policy planners and interest persons in national and international levels. Therefore, in present study, an attempt has been made to investigate the differentials pattern of diarrhoea according to socio-demographic variables and find out the most important determinants.
2. Data and Methods
- The study had been used a representative set of cross-sectional data extracted from the Bangladesh Demographic and Health Survey (BDHS), 2007 [15]. The survey was conducted under the authority of National Institute of Population Research and Training (NIPORT) of Ministry of Health and Family Welfare, Bangladesh. It was designed to produce representative results for the country as a whole, for both urban and rural areas separately, and for each of the six administrative divisions of country. Primary sampling units (PSU) for the survey was based on enumeration areas (EAs) from the population census 2001. Data collection took place over a five month period from March, 24 to August, 2007 and total of 10,996 respondents were interviewed. Among of these only 485 respondents were included in this study based on the experienced an episode of diarrhoea in the last two weeks before the survey. In this study, frequency distribution, contingency analysis and binary logistic analysis had been employed. For binary logistic model, dependent variables were coded women whose children are affected by diarrhoea as one (1) and if not then coded as zero (0). This study includes five explanatory variables with categories shown in the parenthesis, viz. respondents education (1=primary, 2=secondary, 3=higher), husband occupation (1=service, 2=business, 3=farmer, 4=day labor, 5=unemployment), living condition (1=poor, 2=middle, 3=rich), preceding birth interval (1= ≤24 month, 2=25-36 month, 3= ≥37 month), sources of drinking water (1=Tubewell, 2=tap, 3=pond, 4=others. The Statistical Package for Social Sciences version 16.0 (SPSS Inc, Chicago, IL, USA) was used for statistical analysis.
3. Results
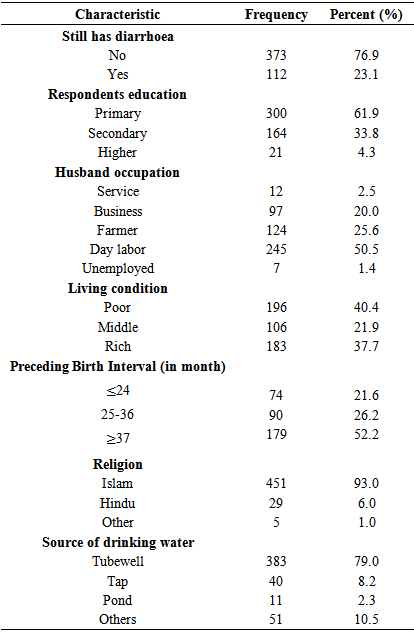
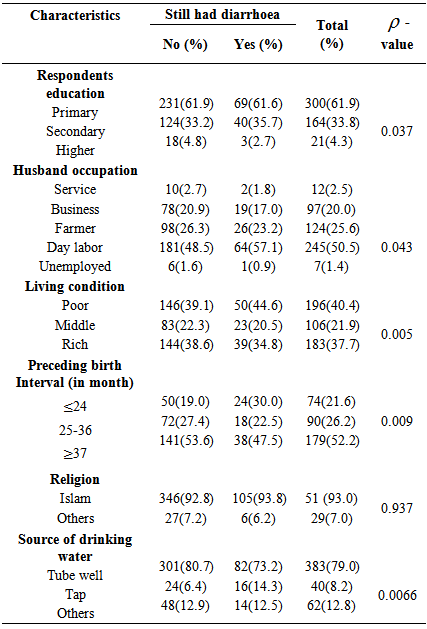
- The frequency distribution of the child still have diarrhoea or not by some selected socio-demographic and economic characteristics of the respondents are presented in Table 1. Results revealed that more than three fourth (76.9%) of the total child had diarrhoea. Most of the respondents were primary educated (61.9%) and day labour (50.5%). About 40.4% of the children grew up with poor living condition and about half of them (52.2%) born with more than three years interval (≥37 month). Three fourth of the respondents used Tubewell (79.0%) and only 2.3% used pond as a source of daily used water.
|
|
|
4. Discussion
- Diarrhoea is one of the most important causes of death among infants in developing countries like Bangladesh [16]. A systematic review of the research suggested that such an association is more likely to occur among low socio-economic groups, less empowered and under-nutrized infants of women. Educational attainment of the respondents is an important item in the study of child’s still has diarrhoea. The prevalence of diarrhoea was more among the child whose mother was uneducated or only primary educated. Some others previous studies also had demonstrated the similar result [16, 12]. Similarly, occupation of husband is one of the vital events of child’s still has diarrhoea. As a religious restricted country, family income status in Bangladesh mainly depends on husband income [17]. If the income is sufficient than obliviously life style will be more improved and lower prevalence of diarrhoea. By supporting the previous study [18, 12, 19], it had concluded that higher percentage of diarrhoea prevalence among the family with earning sources were day labour. It was notified that upper qualities of the asset index, which represents children in families in the group of highest living status had the low prevalence of diarrhea [18, 12]. Preceding birth interval is the key item in the study of child’s still had diarrhoea. Children who were born with more preceding birth intervals were physically more cable to prevent the morbidity [18]. Present study and similar others previous studies also supported this argument [20, 21, 12]. Another major cause of diarrhoea is the sources of drinking water. By supporting the previous many others studies, the present study revealed that safe water reduce the chance of having diarrhoea [22, 21, 12].
5. Conclusions
- In our study, high prevalence of diarrhoea are suspected and reported in Bangladesh. The authors recommend that the frequent nutritional surveys and targeting persons are displaced to better understand the causes of diarrhea. In addition, higher birth interval, increasing the female education, living condition, community health facilities and ensure the sources of safe drinking water are also important to reduce the prevalence of diarrhoea.
ACKNOWLEDGEMENTS
- The Ministry of Health and Family Welfare (MOHFW), Bangladesh has supported data and reports to perform this study. The authors are very grateful to MOHFW, Bangladesh for this support. The authors gratefully acknowledge to the Department of Population Science and Human Resource Development, Rajshahi University; Bangladesh where the study has been conducted.