-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Journal of Health Science
p-ISSN: 2166-5966 e-ISSN: 2166-5990
2014; 4(4): 89-93
doi:10.5923/j.health.20140404.02
Socio-Demographic Characteristics and Pattern of Morbidity among Patients Attending the Infant Welfare Clinic of a Tertiary Health Institution in South Western Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJames Olusegun Bamidele, Eyitope Oluseyi Amu, Olusola Olugbenga Odu
Department of Community Medicine, Ekiti State University Teaching Hospital, Ado-Ekiti, 360001, Nigeria
Correspondence to: Eyitope Oluseyi Amu, Department of Community Medicine, Ekiti State University Teaching Hospital, Ado-Ekiti, 360001, Nigeria.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Infant Welfare Clinics are established to carry out mainly preventive and promotive health services. However, some carry out curative services. This study was carried out to identify the socio-demographic characteristics of ill infants brought to the Infant Welfare Clinic of Ekiti State University Teaching Hospital (EKSUTH), Ado Ekiti, Nigeria, a centre which also offers curative services; the common illnesses they presented with on their scheduled date of immunization and the treatment pattern of these illnesses. A pre-tested, interviewer-administered, semi-structured questionnaire was used to elicit information from all (650) mothers of infants who presented ill at the Infant Welfare Clinic of EKSUTH, Ado –Ekiti, Ekiti State, Nigeria from January 2010 to December 2012. The study covered only children that presented ill on their scheduled day of immunization. The results showed that 53.2% of the respondents were males while 48.2% were females, 26.0% were neonates, 48.2% were 2-3 months while 25.9% were 4-12 months. Majority of the mothers were aged 25-39 years (74.3%), had tertiary education (89.9%), were civil-servants (48.4%) and were Christians (93.8%). The commonest disease presentations were respiratory tract infections (34.8%), skin infections (13.1%) and neonatal jaundice (7.8%). The commonest drugs prescribed were antibiotics (66.7%), haematinics (24.3%) and anti-malarials (7.4%). Most infants presenting ill at the infant welfare clinic were between 1-3 months of life, the commonest presentation were respiratory tract infections while antibiotics were the most commonly prescribed drug.
Keywords: Morbidity patterns, Infant welfare clinic, Nigeria
Cite this paper: James Olusegun Bamidele, Eyitope Oluseyi Amu, Olusola Olugbenga Odu, Socio-Demographic Characteristics and Pattern of Morbidity among Patients Attending the Infant Welfare Clinic of a Tertiary Health Institution in South Western Nigeria, Journal of Health Science, Vol. 4 No. 4, 2014, pp. 89-93. doi: 10.5923/j.health.20140404.02.
Article Outline
1. Introduction
- A child's health during the first five years of life is largely set by events occurring during the prenatal, intranatal and post-neonatal periods [1, 2]. The first year of life is the most dangerous as children are most likely to die at this time more than at than at any other period of their lives [3]. Even though most of the diseases that affect their health are amenable to simple inexpensive interventions and corrections, infant mortality rates in most developing countries are still unacceptably high [3]. In order to decrease child morbidity and mortality and ensure their survival globally, the childhood survival strategies were introduced by the United Nations Children’s Fund (UNICEF), the World Health Organization (WHO) and partners [4].The Infant Welfare Clinics emerged to implement many of these childhood survival strategies at health facility level [4, 5, 6, 7]. Even though children are usually brought to Infant Welfare Clinics for routine immunization and growth monitoring, they can however present with varying forms of illnesses for treatment. These illnesses include diarrhoea, malaria, acute respiratory infections, malnutrition, skin infections and infestations. Others include traumatic injury and even life- threatening conditions such as neonatal jaundice [8, 9, 10, 11, 12, 13].Populations served by Infant Welfare Clinics and public health care centres vary widely in respect of personal and family characteristics and behavioural patterns [14]. However, very little has been done since then about the socio-demographic characteristics of those attending Infant Welfare Clinics. Furthermore, most mention made about infant welfare clinics in the academic literatures have been mainly about infant nutrition, and hardly anything about the disease presentation. This study therefore aimed to describe the socio-demographic characteristics, disease presentation and treatment pattern at the Infant Welfare Clinic of University of Ado Ekiti Teaching Hospital, Ado-Ekiti, South-Western Nigeria. Hence, this study is unique.
2. Materials and Methods
- The study took place at the Infant Welfare Clinic of Ekiti State University Teaching Hospital, Ado–Ekiti. Ado-Ekiti is the capital of Ekiti State, one of the six states in the South-Western geo-political zone of Nigeria. The clinic runs twice a week, on Tuesdays and Thursdays, alongside the nutrition and immunization clinics. At the nutrition and food demonstration sections, growth monitoring and promotion takes place. Those with challenges are counselled by the nutritionist or referred to the doctor. Immunization of children 0-11 months takes place at the immunization section; thereafter mothers whose children are ill are attended to at the clinic by the doctor.
|

3. Results
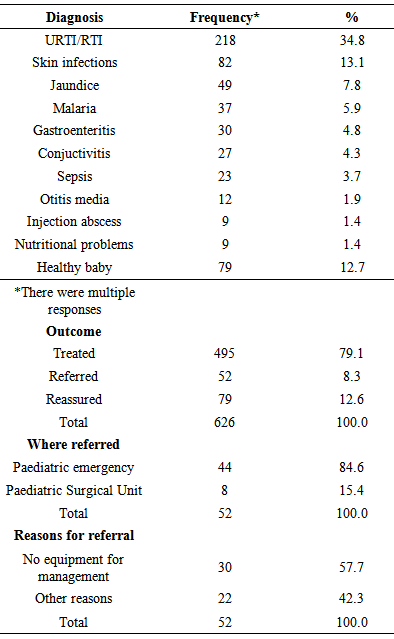
- A total of 626 out of 650 questionnaires administered were correctly filled and fit for analysis (response rate of 96.3%). Five hundred and sixty four (90.1%) of the respondents’ mothers were aged between 25-39 years; 553 (89.9%) had tertiary education; 587 (93.8%) were Christians; 572 (91.4%) were Yorubas; while 610 (97.4%) resided within Ado-Ekiti. Two hundred and seventy (43.1%) of the respondents presented in 2010; 195 (31.1%) presented in 2011, and 191 (25.7%) presented in 2012 (Table 1). There were 585 (93.5%) new and 41 (6.5%) follow up cases all of which were attended to by doctors.The commonest diagnosis made were respiratory tract infections 218 (34.8%), skin infections like impetigo, furunculosis, e.t.c. 82 (13.1%) and neonatal jaundice 49 (7.8%). Seventy nine (12.7%) of the respondents were found to be healthy. The least common diagnosis were injection abscess 9 (1.4) and nutritional problems 9 (1.4%). Four hundred and ninety five (79.1%) of the respondents were treated, 52 (8.3%) were referred, while 79 (12.6%) who were found to be healthy were counselled and reassured. Forty-four (84.6%) of the referrals were to the Paediatric Emergency Ward and most of them were referred because of lack of equipment to adequately manage them at the Infant Welfare Clinic as most of them needed more than outpatient care (Table 2).
|
|
4. Discussion
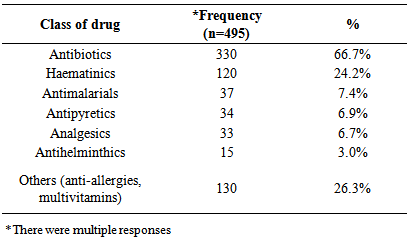
- The study examined the socio-demographic characteristics and morbidity patterns of patients attending the Infant Welfare Clinic, Ekiti State State University Teaching Hospital, Ado-Ekiti, Nigeria. The male to female ratio was 1.13 to 1. This is similar to that reported by a study conducted in Ilesa, Nigeria in which the ratio of male to females was 1:1 [9]. Eighty-five percent were aged below 6 months, 14.4% were between 6-11 months while only 0.6% were above 12 months. This contrasts with that of the Ilesa study in which those below six months constituted 22.7%; those aged 6-12 months constituted 18.9% and those above 12 months constituted 58.2% of the respondents. The disparity in the ages can be explained by the fact that this study was conducted at a clinic designated mainly for infants even though those above 12 months could attend, whereas the other study was conducted among children less than five years of age. Hence it had fewer respondents who were below 6 months and more who were older than 12 months of age [9].Five hundred and sixty four (90.1%) of the respondents’ mothers were aged between 25-39 years. This is expected as most of the mothers are within the reproductive age group. Almost all the mothers (99.3%) were educated, with 553 (89.9%) having tertiary education, this is high in comparison with other studies conducted within the country. For example, in the 2004 Nigerian Demographic health survey (NDHS) only 58.0% of the mothers were educated while only 5.9% had tertiary education [15]. In addition, a study on complementary feeding practices conducted among mothers of under-five children in Satellite town, Lagos Nigeria reported that while 91.1% of the mothers were educated, only 64.9% had tertiary education [16].It is also a reflection of the type of people that patronize the Teaching Hospital and the part of Nigeria that the people came from, Ekiti State. Ekiti State is known for the high level of literacy among the indigenes. It is also reflective of the urban nature of the study location. Had the study been conducted in a rural PHC setting, even though the literacy rate may be high, the proportion of those with tertiary education might not be this high. Almost all the mothers 610 (97.4%) resided within the urban community. This is in keeping with the National Policy on Immunization that clients that come for immunization must be within the catchment area of the health facility.Close to half of the respondents presented in 2010; about one third in 2011, while the rest presented in 2012. That the number of patients seen declined over time might be due to the fact that mothers also patronized the children clinic which is run daily by the Paediatrics Department and on the other hand, the illness episodes of the infants might not have coincided with their immunization clinic appointments (the immunization/Infant welfare clinic is only run twice in a week). In addition, there was a state-wide strike of all health workers at primary and secondary levels in 2010 and part of 2011. During these periods, all the patients accessed health care services at the tertiary level (Teaching Hospital) where the staff members were not on strike. The upward surge in patient attendance during those months made it seem as if the trend of illness is decreasing whereas it is not.The commonest diagnosis made were respiratory tract infections 218 (34.8%), skin infections 82 (13.1%) and neonatal jaundice 49 (7.8%). The commonest cause of morbidity in this study is similar to that reported in other studies among infants in which respiratory tract infections and diarrhoea were parts of the main cause of mortality and morbidity in infants aged less than one year [17, 18]. It is also similar to the WHO report that acute respiratory infection is one of the five diseases that are responsible for seventy-five percent of childhood illnesses [8]. It however differs from these other reports in that diarrhoea, malaria, measles and malnutrition did not play significant roles as causes of infant morbidity in this study. It also differs from that of a study conducted in Ilesa South West Nigeria in which malaria was reported as the commonest morbidity for which patients presented [9].Malaria, diarrhoea and nutritional problems were ranked fourth, fifth and tenthrespectively in the order of frequency; while there was no reported case of measles. In this study, majority of those that presented with complaints were below three months old. Cases of malaria, diarrhoea and nutritional diseases are usually less in this group of infants due to the fact that they are still being breastfed. After the age of six months however, the incidence of these diseases rises due to problems associated with weaning and decreasing maternal antibodies.Skin infections and neonatal jaundice were ranked second and third as causes of morbidity in this study. Bacterial skin infections like impetigo and fungal ones like cutaneous candidiasis are common among infants in the first few months of life due to their poorly developed immune system and exposure to microorganisms during or after delivery. Bacterial skin infections can lead to other severe life threatening infections like pneumonia and meningitis if not promptly treated. Neonatal jaundice which can be physiological or pathological affects 50-60% of infants in the first week of life. Timely presentation and investigation of the underlying cause and prompt treatment helps to reduce the risk of bilirubin encephalopathy (kernicterus) with its attendant sequelae. The fact that 26% of the respondents in this study were neonates can probably account for skin infections and neonatal jaundice ranking high on the list of morbidities for which they presented at the clinic.Though the mothers came with one complaint or the other, 79 (12.7%) of the respondents were found to be healthy after being interviewed and examined. They were thereafter counselled and reassured. Being an infant welfare clinic, most of the mothers came for immunization but some also used the opportunity to express their anxieties to the doctors. These were commoner among mothers who gave birth for the first time. It is better for mothers to present at the hospital and be reassured that all is well with their babies rather than to sit at home assuming that all is well or take wrong counsel from their fellow mothers whose children might have experienced such symptoms.Majority of the infants (79.1%) were treated but those that required further investigations and treatment (8.3%) which was not available at the Infant Welfare Clinic were referred to the Paediatric Emergency Ward. Most of the jaundice cases were referred. The three commonest drugs prescribed were antibiotics (66.7%), haematinics (24.2%) and anti-malarials (7.4%). The antibiotics commonly prescribed were amoxicillin, amoxicillin + clavulanic acid, and cephalosporins. That antibiotics had to be prescribed most often is not far-fetched: most of the conditions for which the infants presented were infective and bacterial in origin. These included complicated upper respiratory tract infection, lower respiratory tract infection, conjunctivitis, sepsis, otitis media and injection abscess. Heamatinics were sometimes prescribed along with the antibiotics or anti-malarials. Even though less than 10% of the patients presented with malaria, antimalarials ranked third on the list of the drugs prescribed. This is because some of the patients were referred while others were just counselled. The antimalarials most commonly prescribed were Arthemether – Lumefantrine combinations.
5. Conclusions
- This study concludes that of all the infants brought to the Infant Welfare Clinic of EKSUTH, those with complaints were mostly between the ages of 1-3 months. The commonest diseases seen were respiratory tract infections, skin infections and neonatal jaundice. The commonest drugs prescribed were antibiotics, heamatinics and antimalarials.
Study Limitation
- The disease pattern shown in this study might not represent the true morbidity pattern of the infants during this period as only those respondents who came for immunization and had one complaint or the other were seen. On days which did not coincide with the immunization clinics, they were seen at the Paediatric under-five clinic.
ACKNOWLEDGEMENTS
- The authors would like to acknowledge the respondents who were interviewed and the residents who collected the data.