-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Journal of Health Science
p-ISSN: 2166-5966 e-ISSN: 2166-5990
2014; 4(4): 79-88
doi:10.5923/j.health.20140404.01
Strategies for Transformational Change in the Health Care System: Challenges Facing an Aging Population
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMing-Jye Wang1, Hung-Yu Yang2, Chien-Chang Yang3, Yi-ting Lo1
1National Taiwan University Hospital Hsin-Chu Branch, Hsinchu City, Taiwan
2Institute of Health Industry Management, Yuanpei University, Hsinchu City, Taiwan
3Far Eastern Memorial Hospital, New Taipei City, Taiwan
Correspondence to: Ming-Jye Wang, National Taiwan University Hospital Hsin-Chu Branch, Hsinchu City, Taiwan.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Reforming the health care system is a challenge for every country in the world in the 21st century. What is beneficial for an individual condition may not be good for patients with multiple conditions. Based on the actual medical records of a population age 55 and older as outpatients and inpatients, this study used a person-based longitudinal analysis to investigate the trends in healthcare seeking and the consumption of medical care resources. Amonga cohort comprised of 300,000 patients randomly chosen from the National Health Insurance Research Database of Taiwan, 48,836 persons aged 55 and older were then followed longitudinally 10 years. The results clearly demonstrated that there were gender and age differences, as men had a lower frequency of consultation but a greater frequency of admissions and consumption of medical care resources than women. Age 75 was a key point in healthcare utilization. Since population aging is inevitable and continues to increase rapidly, it is important to establish a new health care system, raise awareness of health risks, strengthen preventive health services, especially for men, and plan health manpower resources to train enough professionals in the care of the elderly.
Keywords: Aging population, Healthcare seeking behavior, Consumption of medical care resources, Health care system
Cite this paper: Ming-Jye Wang, Hung-Yu Yang, Chien-Chang Yang, Yi-ting Lo, Strategies for Transformational Change in the Health Care System: Challenges Facing an Aging Population, Journal of Health Science, Vol. 4 No. 4, 2014, pp. 79-88. doi: 10.5923/j.health.20140404.01.
Article Outline
1. Introduction
- Given that the population is rapidly aging, health care system reform has become a challenge for every country in the world in the 21st century. According to the World Health Organization, between 2000 and 2050, the proportion of the world's population over 60 years of age will double from about 11% to 22%. The absolute number of people aged 60 and over is expected to increase from 605 million to 2 billion over the same period [1]. In Taiwan, the percentage of the population aged 65and older was 10.9% in 2011 [2], and will be 20.0% by 2025and 36.5%by 2050 [3]. As a result of this demographic change, the prevalence of chronic diseases, and health care needs and utilization will increase substantially [4, 5]. Medical expenditures are also expected to increase [6]; however, the design for the acute care system currently in use will not be appropriate for these complex chronic conditions [7]. In general, the elderly also have greater susceptibility, their metabolism is different from younger people, and they simply get frailer as they age [8]. From the perspectives and needs of older people, rethinking strategies for the health care system is an important issue.In order to safely and effectively care for the elderly, there is a growing consensus that we must evaluate how the health services are delivered and received, along with how to improve the health care system to better meet the healthcare needs of an aging population [5]. This will require the development of mechanisms to deliver more need-based and quality services, while thoughtfully considering users’ concerns and perspectives [9]. Previous research has shown that healthcare seeking behaviors and healthcare utilization patterns were influenced by many factors such as, age, gender, severity of illness, and economic status [10, 11]. Age and gender are associated with health related behaviors and beliefs [12]. They are the fundamental dimensions in the study of utilization of services, yet are rarely taken into account when planning service provision [13]. They play an important role in influencing health and the utilization of healthcare services by older people [14, 15]. Therefore, understanding the differences and trends by age and gender in healthcare seeking behavior and healthcare utilization by the elderly is essential in order to provide need-based healthcare delivery [16-18] and the initiation of reform measures in the health care system [15, 18].In terms of clinical practice, what is beneficial for an individual condition may not be good for patients with multiple conditions [19, 20]. Ignoring the existence of multiple conditions, and adhering solely to the clinical practice guidelines for single disease may lead to harm for patients [21, 22]. With regard to research, a literature review demonstrated that research agendas varied widely in terms of subject, problem, purpose, scope, and organizational framework. Most agendas were developed based on expert opinion guided by an explicit process and criteria for prioritization [20]. Thus, in order to resolve healthcare needs of and service utilization of seniors, regardless of clinical experience and research findings, it is increasingly important to shift our traditional focus on diseases and syndromes as if they were independent of each other to an understanding of the healthcare needs and healthcare seeking behaviors of the elderly by means of a person-centered approach [23]. Such findings may then provide credible and adequate information as the basis for health policy changes and clinical decision making. However, to date most research has utilized cross-sectional studies, questionnaires, or self-reported healthcare experiences rather than a person-based longitudinal analysis to investigate healthcare seeking behavior through medical databases. This study was based on the actual medical records obtained from the national health insurance research database (NHIRD), avoiding possible subjective self-reports and recall biases. This person-based longitudinal study followeda population of age 55 and older as outpatients and inpatients to investigate the trends in healthcare seeking and the consumption of medical care resources during a 10-year period, and was more responsive to the dynamic behavioral and resource changes than previous studies.The aims of this study were: (1) to investigate the trends in healthcare seeking behaviors by elderly outpatients and inpatients, (2) to compare differences and trends in the frequency of healthcare seeking behavior by gender and age, and (3) to analyze the impact of and trends in the consumption of outpatient and inpatient medical care resources by gender and age in this population. These findings may then influence the government in making health policy decisions, creating models of health services, and determining priorities for medical resource allocation in order to develop an effective health care system that met the needs of the elderly.
2. Methods
2.1. Data Sources
- The data used in this study were taken from the NHIRD which was constructed by the National Health Research Institutes (NHRI). The process is described as follows: each year, the National Health Insurance Administration (NHIA) collects data from the National Health Insurance (NHI) program and sorts it into data files, including registration files and original claim data for reimbursement. These data files are de-identified by scrambling the identification codes of patients or care providers, including medical institutions/facilities and physicians, and then sent to the NHRI to form the original files of NHIRD. Each researcher is required to sign a user agreement declaring that she/he has no intention of attempting to obtain information that could potentially violate the privacy of patients or care providers and acknowledge the NHIRD in their publications [24].This study was approved by the review board of National Taiwan University Hospital Hsin-Chu Branch.
2.2. The Method of Sampling
- According to the NHIRD, a cohort of 1,000,000 beneficiaries was randomly sampled from the NHI registry of beneficiaries from March 1, 1995 to December 31, 2000 (from a total of approximately 23,753,407 persons). Using linear congruent random number generation to randomly sample the cohort, the patients were followed longitudinally unless they were lost due to death or emigration, and the data were updated annually. There were no significant differences in age, gender, or expense distribution between the sample and the general population.The subjects analyzed in this study were 300,000 beneficiaries selected from the cohort of 1,000,000 in databases which contained registration files and all the original claims data.48,836 persons who were55 and older among the sampled were followed longitudinally from 2001 to 2011.
2.3. Study Variables
- To investigate the impact of aging on healthcare seeking behavior and the depletion of medical care resources, the following variables were included: demographics (age and gender), healthcare seeking behavior (HSB) (user of outpatient services, frequency of consultation, admission user, and frequency of admission), and the consumption of medical care resources (amount of each claim, total amount of claims, and length of stay). These variables were defined according to the NHIA.
2.4. Demographic Variables
- Due to the limitations of the database, the only two demographic variables analyzed were age and gender, which have been reported to be the basic factors influencing the assessment of health needs and utilization services [13]. Age was stratified into following groups: 55-59, 60-64, 65-69, 70-74, 75-79, 80-84, and 85+ years of age for analysis.
2.5. Healthcare Seeking Behavior (HSB)
- Users of outpatient services/admissions referred to the total number of persons using outpatient services/ admissions within one year. Frequency of consultation/ admission referred to the total number of outpatient visit/admissions within one year.
2.6. Consumption of Medical Care Resources
- The amount of each claim was the expense (not including co-payment) that the NHI-contracted medical care institutions submitted to the NHIA for each patient per episode of illness. The total amount of claims was the total expense for each patient within one year. Length of stay was calculated by subtracting the day of admission from the day of discharge.
2.7. Statistical Analysis
- Descriptive statistics, such as percentage and frequency were used to determine the distribution of study participants’ characteristics and the trends in seeking healthcare as outpatients and inpatients by gender and age. Two-way analysis of variance was used to analyze differences and trends in frequency of healthcare seeking behavior and consumption of outpatient and inpatient medical care resources by gender and age. SPSS 19.0 was used for all analyses.
3. Results
3.1. Study Participant Characteristics
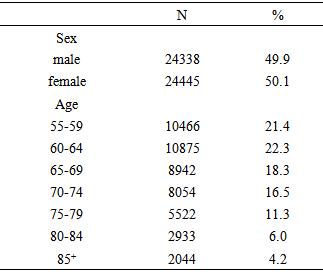
- Among the study participants, 49.9% were male and 50.1% were female; the gender of 53 persons was unknown. The 60-64 agegroup accounted for 22.3%, 55-59 and 65-69 age groups accounted for 21.4% and 18.3% respectively, and those aged≧85 accounted for 4.2% (Table 1).
|
3.2. Trends in Seeking Outpatient Healthcare
- The percentage of users of outpatient services among the study participants accounted for 86.91%, 75.24%, and 64.04 % in 2001, 2006, and 2011, respectively. If calculated separately by gender, the outpatient percentage for females was greater than that of males’ (87.41%>86.41%, 77.32%>73.14%, 67.79%>60.27% for those years), and there was a declining trend over the years. The percentage of outpatients in each age group decreased as well, especially for those over 70. (Table 2)
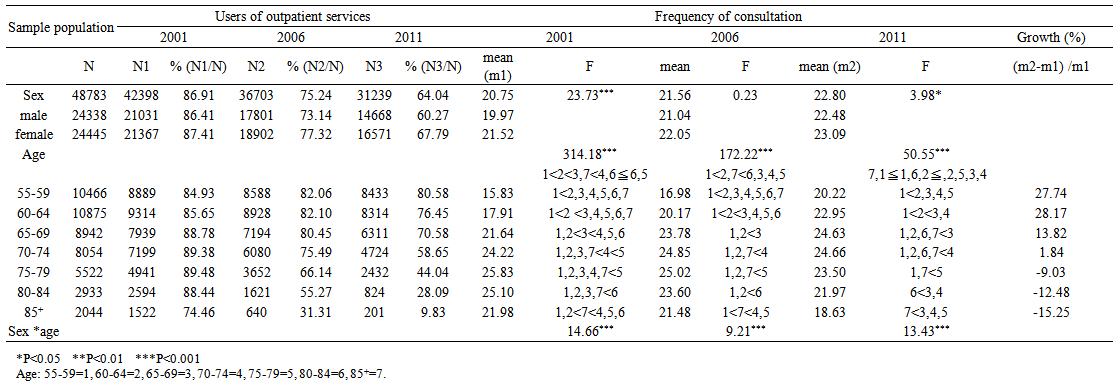 | Table 2. Trends in seeking outpatient healthcare |
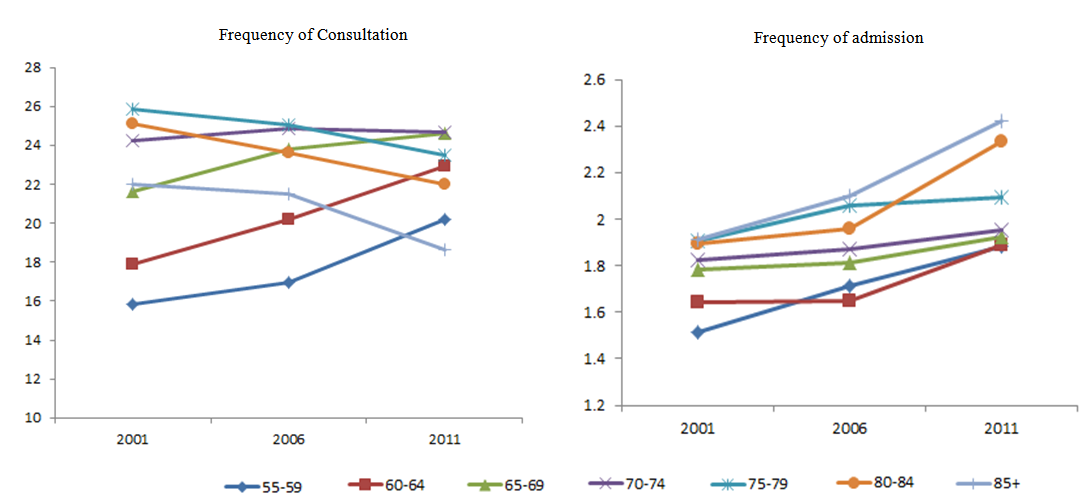 | Figure 1. Trend map of seeking outpatient/inpatient healthcare on each age group amount of each claim (outpatient) |
3.3. Trends in Seeking Healthcare Admission
- The percentage of admission users among study participants accounted for 15.84%, 14.65%, and 14.27 % of services in 2001, 2006, and 2011, respectively. If calculated separately by gender, the percentage of males users was greater than that of females users for those years (17.46%>14.22%, 15.80%>13.51%, 14.85%>13.68% for those years), and there were more users of inpatient services in the older groups. There were no obvious gaps between age groups. The frequency of admissions by gender showed significant differences, and there was a rising trend over the years. The older age group had a higher frequency of admission. The gaps were larger between 60-64 and 65-69in particular, and the frequency of admissions for each age cohort showed a rising trend over the 10 year period, particularly for those over 75. (Table 3, Figure 1)
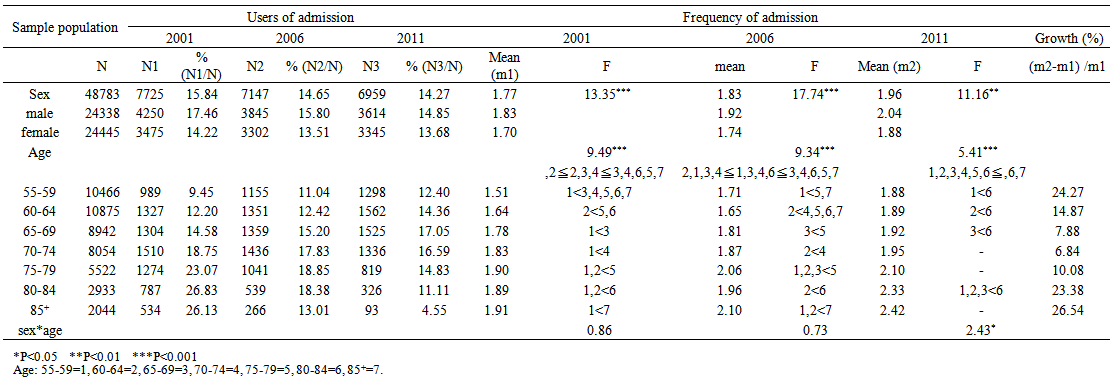 | Table 3. Trends in seeking healthcare admission |
3.4. Analysis of the Consumption of Outpatient and Inpatient Medical Care Resources
- Table 4 showed the gender differences in amount of each claim and the total amount of claims for outpatient services. Both claims made by males was greater than those did by females, and there was a rising trend over the years. The both amount of claims were highest for 70-84 year olds and there was a rising trend by year for each age cohort. The amount for 85+ year olds declined sharply in 2006, and the percentage of growth was largest for 55-69 year olds. (Figure 2)
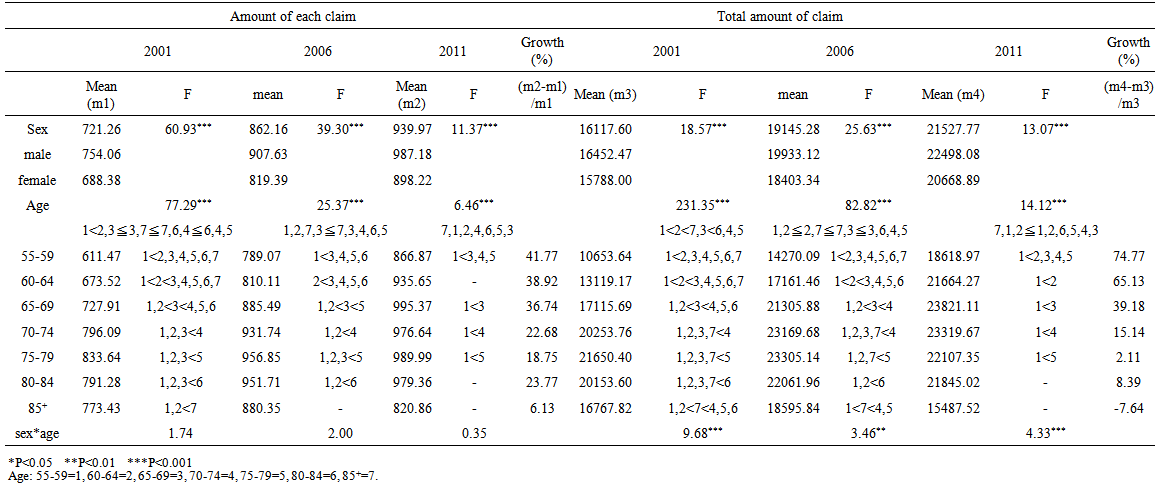 | Table 4. Analysis of the consumption of outpatient medical care resources |
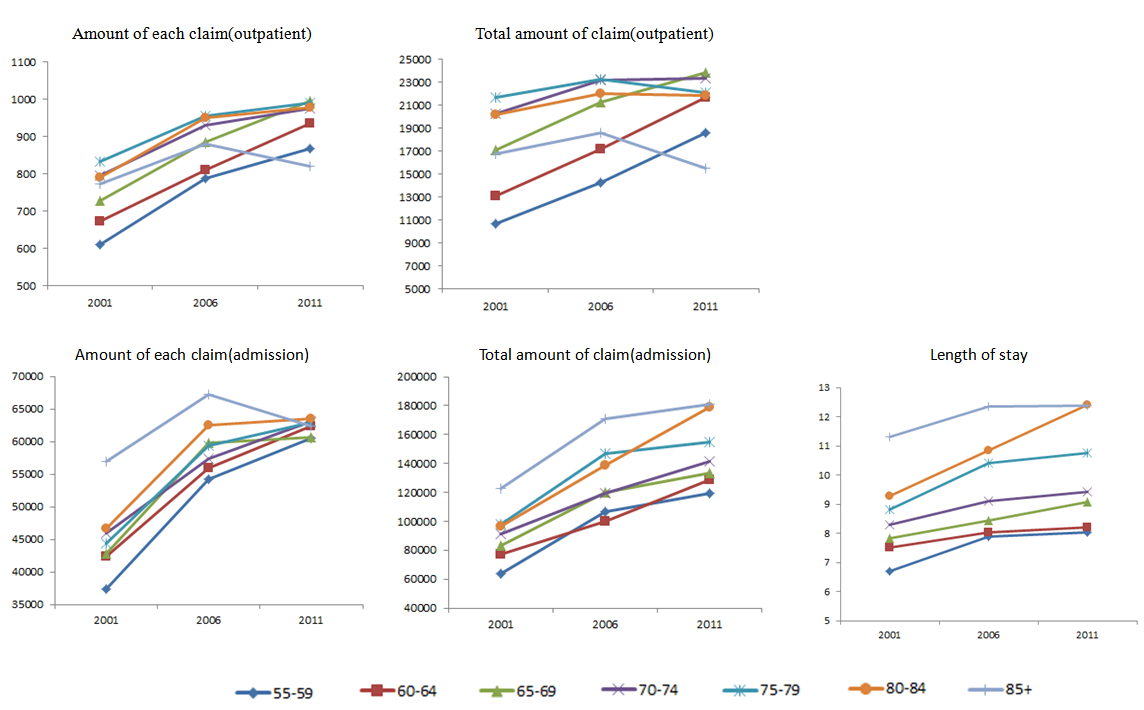 | Figure 2. Trend map of the consumption of outpatient and inpatient medical care resources on each age group |
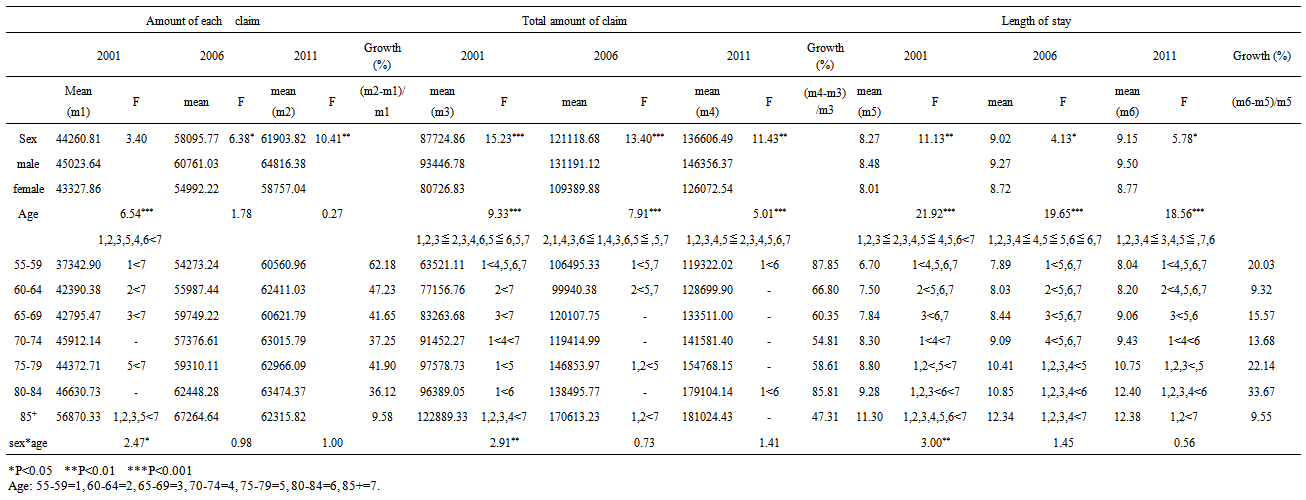 | Table 5. Analysis of the consumption of inpatient medical care resources |
4. Discussion
- This study was different from previous studies, in that it was based on patients’ actual medical records and used a person-based longitudinal approach. It was therefore more responsive to dynamic healthcare seeking behaviors and changes in the consumption of medical care resources. Overall, trends in the percentage of users of outpatient services over the 10 years were from 86.91% to 64.04%. In terms of gender, females ranged from 87.41% to 67.79%, and males from 86.41% to 60.27%.This was consistent with almost 90% of 70+ year olds visiting a physician in the previous year as reported by Vadla et al. [25], and 75% of men and 88% of women visiting a doctor in the previous year as reported by Pleis et al. [26]. In this study, the declining percentage of users of outpatient services by year may possibly have been due to the closure of the study population, due to death or other factors leading to a decrease in the number of persons followed over the 10 years, and more so for those over 70. With regard to the frequency of consultations, this study showed that females had more outpatient visits than males did, and there was an increasing trend over the years. The literature has shown that patterns of outpatient utilization were different; these included visits to family physicians [5, 18], specialist physicians [18, 27], general practitioners [28, 29], or primary care practitioners [4, 30-32]. Although these methods of research were diverse, a common finding remained that women had a higher outpatient utilization rate than men did. In general, women are more sensible than men, are prone to express feelings easily, and show a greater awareness of health problems and symptoms. Therefore, they often have worse perceptions about their own health and suffer from non-fatal condition that can be taken care of in primary healthcare settings [25].Our study found that the users of outpatient services decreased and the frequency of consultation increased over the 10 years; this showed that the frequency of consultation for each person increased each year. Age analysis demonstrated that age 75 became critical for increases or decreases in the frequency of consultations. While it is widely known that health service utilization is usually associated with age [15, 33, 34], Walter-Ginzburg et al. [35] indicated that age was not significantly related to healthcare utilization. Vegda et al. [18] and Nie et al. [5] thought that there was a decrease in utilization at 85+ of each type of frequency of healthcare seeking. Potential explanations for the declining utilization of physicians may be that those people surviving into that age group were healthier or the patient giving up [5], and the gap between different age groups narrowed with increasing proximity to death [36]; we found the same in this study; however, gaps in healthcare utilization were larger in the 60-64 and 65-69 age cohorts.In terms of admission users, the results of this study showed that males has a greater percentage than that of females did, older age groups had a higher percentage than younger age groups, and there were no obvious gaps between groups. Unlike the decline in the percentage of outpatient, the percentage of hospitalization did not show any sign of decline, which may be due to the transfer from outpatient to hospitalization. With regard to the frequency of admissions, the findings of this study showed males were hospitalized more often than females, which was in accord with results of the majority of previous studies [31, 37, 38]. This was probably due to the differences between men and women in health consciousness [39], health problems, healthcare seeking behavior [40, 41], and social factors [42], all of which led to a higher frequency of admissions for men. Men responded later to the severity of symptoms than did women [38], they also tended to delay seeking help, were less likely to have routine checkups and necessary medical care, and dealt with health problems by waiting as long as possible before seeking help [42, 43]. Age analysis showed that the older age group had a higher percentage of hospitalization; this was in agreement with the findings by Woo et al. [36] who found the most frequent admissions in those 85+ years old. The consumption of medical care resources for males was higher than that of females’ as demonstrated in this study, which was consistent with Hsu et al. [44] and Cylus et al. [45] some diseases such as heart disease and heart failure occur more often in men, resulting in higher hospital costs. The difference may be due to the masculine views in men [43, 46], who disregard early signs of disease and the importance of preventive care [12, 29, 30, 42, 43, 47]. Additionally, women traditionally play a greater role in managing family health and the use of health care services [29]. The result of this synergistic effect is that men are less likely than women to seek healthcare as outpatients and more likely to seek healthcare as inpatients, resulting in more hospitalization expenses for men. For acute medical care, medical expenses often increase with age [48, 49], and were higher at 75-84 years of age when studied by Hsu et al. [44]. Heinrich et al. [50] found that 75+ year olds had an approximately11.3day length of stay. This study showed the same result.
5. Conclusions
- Compared to the previous literature that focused on cross-sectional and self-reported past history studies, this study used person-based longitudinal method and actual medical records to investigate the trends in healthcare seeking behavior and consumption of medical resources. The results clearly demonstrated that there were gender and age differences, as men had a lower frequency of consultation but a greater frequency of admissions and consumption of medical care resources than women. Age 75 was a significant age in healthcare utilization. Given that population aging is inevitable and continues to increase rapidly, it is important to establish a new health care system, raise awareness of health risks, strengthen preventive health services, especially for men, and plan health manpower resources to train enough professionals in the care of the elderly.
ACKNOWLEDGMENTS
- This study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by National Health Research Institutes in Taiwan. The interpretation and conclusions contained here indo not represent those of Bureau of National Health Insurance, Department of Health or National Health Research Institutes.
Conflict of Interest
- The authors declare that they have no conflict of interest.