-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Journal of Health Science
p-ISSN: 2166-5966 e-ISSN: 2166-5990
2014; 4(2): 34-40
doi:10.5923/j.health.20140402.02
Assessment of Pattern of Sport Injuries in Selected Ballgames during a Season of the Kenyan National Leagues
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLN. K. Bailasha1, L. K. Kibera2, E. G. Rintaugu3, Mwisukha A.3
1Department of Physical Education and Sport, University of Nairobi, Nairobi, Kenya
2Department of Educational Foundations, School of Education, University of Nairobi, Kenya
3Department of Recreation Management and Exercise Science, Kenyatta University, Nairobi
Correspondence to: E. G. Rintaugu, Department of Recreation Management and Exercise Science, Kenyatta University, Nairobi.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
The purpose of this study was to investigate the pattern and specific anatomical location of injuries on male and female players in one season of the Kenyan national division one leagues of basketball, handball and volleyball. It was prospective cohort design with 768 participants (478 male and 290 females) who comprised of 138 male and 133 female, 191 male and 95 female and 149 male and 62 females in basketball, handball and volleyball, respectively. Data was collected during training and competitions and recorded on a sport injury observation schedule. An injury was recorded if it caused a player to stop playing in that or subsequent games during training or competition. Chi-square set at 0.05 level of significance was used to test hypotheses of the study. Findings showed that 2098 injuries occurred during the season with 1362(64.9%) and 736(39.1%) affecting male and females, respectively. Cumulatively, the number of injuries per player was slightly higher in proportion to males (2.8) than females (2.5). Significant differences were found between and within sport and gender on the pattern and also the site of injury. However, within gender, a significance difference in the pattern of injuries was only found in females of basketball, male players of handball and both genders of volleyball. On the specific location of the injury, results showed significant difference was found in all except females of handball. It was concluded that pattern and anatomical location of injuries is influenced by gender, nature and characteristics of a sport.
Keywords: Ballgames, Injuries, Kenya, League
Cite this paper: N. K. Bailasha, L. K. Kibera, E. G. Rintaugu, Mwisukha A., Assessment of Pattern of Sport Injuries in Selected Ballgames during a Season of the Kenyan National Leagues, Journal of Health Science, Vol. 4 No. 2, 2014, pp. 34-40. doi: 10.5923/j.health.20140402.02.
Article Outline
1. Introduction
- The concept of preventing sports injury was first muted in 1905, when the then president of United States(U.S), Robert Theodore Roosevelt challenged the American colleges to “adjust the rules in the American football to eliminate risks” [1]. Many years later, not so much was achieved towards this area with much attention being focused on the process of treating and rehabilitating injured athletes [2]. In the recent past, there has been growing enthusiasm for a paradigm shift from curative to preventive management of sport injuries. These developments have had resultant effects on the rules, facilities/equipment and standards of officiating in different sports [3]. Anecdote evidence indicate that sport injuries are alarmingly increasing, possibly due to the rigors of training, entry of many participants in sport for health benefits or the fact that sport is currently a major source of employment. The process of preventing sport injuries requires knowledge of their patterns in order to unearth information that to guide formulation of strategies for their prevention [4].The model of causation of sport injuries and their risk during sport participation contend that sport injuries should be delineated from different sources- intrinsic, extrinsic or the inciting events(actual playing actions) [5]. They should also be approached from a mechanical, social, and psychological and tissue adaptations point of view [6, 7]. Furthermore, it is recommended that methodology of studying sport injuries need to engage proactive approach to produce current and real time empirical data [8, 9]. Studies on the pattern of sport injuries indicate that nature of the sport whether contact, non-contact, individual or team sport and characteristics of its skill influence pattern and location of the injury [10-13]. There is however a dearth of literature about cohort prospective studies of injuries in different sports collectively; with most of the studies being retrospective and focusing on a specific sport during a day or two days tournament [14, 15].With the current influx of many people into sport for both competitive and recreational needs, documentary evidence of the pattern and anatomical site of the injury is necessary to give insight on the risk of participating in a particular sport. This would facilitate development of strategies for injury prevention as well as determine approaches of training [16-18]. A study of the pattern and anatomical site of injuries in different sports would also form a framework for comparative purpose and guide and encourage synergism in harnessing capacities for developing collaborative programs of injury prevention among federations. Injury studies need to be conducted to determine injury profile of players in order to answer questions on whether there are differences in the spread of injuries and anatomical location between males and females in different sports. Therefore, a study of the pattern and site of injuries represents unparalleled opportunity of reducing morbidity and mortality of athletes [19].
2. Methods and Materials
2.1. Research Design
- Cohort prospective design was used for this study. Cohort prospective designs have become popular in the recent past as it helps generate real time knowledge about aspects of development at different stages of life compared with retrospective design which is affected by recall errors. Prospective designs offer a reasonable alternative of identifying real time information for this study, without unethically interfering with the privacy of respondents unlike other designs like randomized experimental research design [10]. This design was applicable because real time information of sport injuries was observed and recorded from cohorts in basketball, handball and volleyball during practice and competitions.
2.2. Population
- The population for this study was drawn from 62 teams that were registered for the 2010 Kenya national leagues of basketball, handball and volleyball. According to gender, there were 24 teams in basketball with 12 male and 12 female, 21 teams in handball with 14 male and 7 female and 17 teams in volleyball with 12 male and 5 female teams. Bio data of players was extracted from registers of the respective sports and a code value was attached to each player. The code was serialized using membership registration number. In each sport, the following numbers of players were registered; 288 in basketball comprised 144 male and 144 females, 294 in handball comprised 196 male and 98 females and 221 in volleyball comprised 156 male and 65 females. In total 803 players were registered in the three sports for that season and comprised of 496 male and 307 females.An exclusion criterion was developed for the purpose of identifying specific players for the study. Since the aim of the study was to assess new sport injuries within the season, beside other conditions, the exclusion criteria was based on the presence or absence of a sport injury to a player prior to the beginning of the study. Therefore, only a player who was duly registered for the respective sport and was to be regularly fielded and had not suffered a sport related injury during the last four months prior to commencement of this study was selected for the observation. Consequently, 768 players met the conditions of the inclusion criteria with a dropout rate of 4.35%. They comprised of 138 males and 133 females in basketball, 191 males and 95 females in handball and 149 males and 62 females in volleyball hence there was no need for further sampling of the subjects.
2.3. Instrument for Data Collection
- A sport injury observation schedule was developed based on the conceptual model for the causation and management of sport injuries [6, 7]. It was designed to allow recording of multiple injuries during training and competition in real time. A focus group discussion consisting of researchers in the field of human performance and sport appraised the items of the tool. The tool was piloted with basketball, handball and volleyball teams of the national league during the last quarter of the 2009 season. Research assistants were drawn from the team analysts of the respective sports. A team analyst is a certified trainer and therefore has basic knowledge of sport medicine and is supposed to accompany their teams during training and competitions. Research assistants were initially guided by the researcher on the process of observation and recording of injuries in the observation schedule. They were allowed to practice the process by informally record characteristics of injuries in their teams independently. Their results were randomly compared for conformity and consistency and disparities were clarified or corrected. Finally, a group of 12 research assistants and 21 coaches/physicians were selected for the piloting of the tool with selected teams. The teams for the pilot were drawn from the National Division Two Leagues of basketball, handball and volleyball in the last quarter of 2009 season and included two male and two female basketball teams, two male volleyball teams, one male handball team.The response return rate for the pilot study was 12 (100%) from research assistant and 15(71.4%) by the coaches/ physicians. The lack of 100 percent return rate from the coaches could be attributed to their absence during training sessions or some injuries could have been too minor to warrant their documentation. An inter-ratter reliability test for consistency in the interpretation of the items in the tool was performed on the responses between research assistants and coach/physicians yielding a reliability of 0.79. A split-half method was used to correlate responses of the items in the observation schedule and yielded a correlation-coefficient of 0.79 which was considered adequate for the study. Data for the study was collected by researcher and research assistants assisted by team coach/physician. Returns and summaries were made on weekly basis by the researcher.
2.4. Data Analysis
- Data was coded and cleaned through statistical package for social sciences (SPSS). Data generated was nominal and was therefore expressed in frequencies and percentages and presented in tables. Chi-square test of independence at p value ≤ 0.05 probability of error was used to analyse the data since it is the appropriate non-parametric statistical tool for the analysis of nominal data [20].
3. Results
3.1. Patterns of Injuries
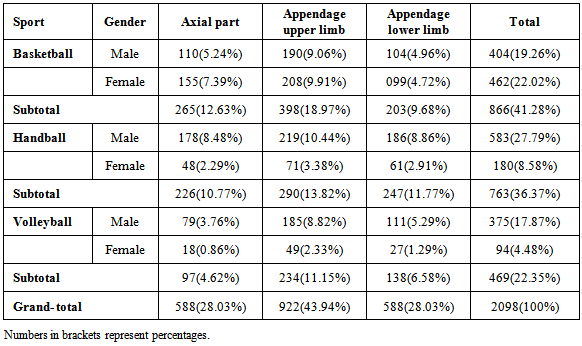
- The patterns of injuries in different sport are presented in Table 1.
|
3.2. Pattern of Sport Injuries Based on the Type of Sport and Gender
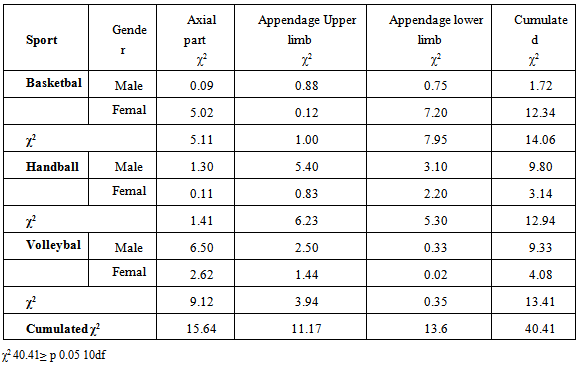
- Table 2 shows the association on the pattern of injuries by sport and gender.
|
3.3. The Anatomical Location of Sport Injuries
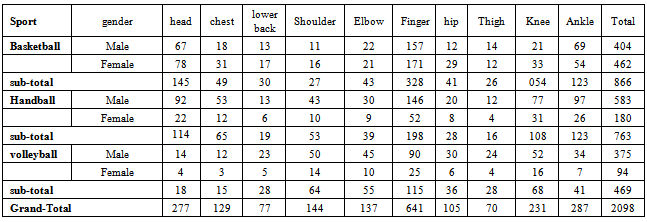
- The anatomical location of the sport injuries are presented in Table 3.
|
3.4. Association between Anatomical Location of the Injuries, Gender and Type of Sport
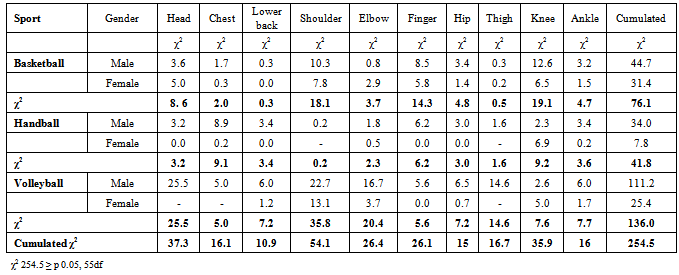
- It was hypothesized that there will be no significant difference in the anatomical location of sport injuries between and within sports and gender. The anatomical location of the injuries and its relationship with type of sport and gender is presented in Table 4.
|
4. Discussion
- The results (table 1) seem to contradict other findings that sport injuries in most sports occur to the ankle and knee than in other parts of the body [12,21-23]. This difference may be attributed to either the method of classifying body parts, the purpose or the sport used between the studies. It was found in this study that in the three sports, appendage upper limb was the most affected with finger as the most commonly injured part. The fact that equipment/facility specifically the ball has been reported to be a main cause of injury in other studies [24,25] indicate that finger on the appendage of the upper limb which is mainly used in these sport is more prone to injuries. It is therefore apparent that nature of the sport and its demands determine the pattern of injuries. Furthermore, injuries on the finger, arm and shoulder are justifiable by the nature of play of these sports. The patterns of injuries in the three sports seem to be similar for both male and female athletes.In regard specific sport, the pattern of injuries showed that playing basketball increases risk of injuries on the appendage upper limb than on either the axial part or appendage lower limb to players. A similar picture is replicated on the handball and volleyball but with a difference on the number of injuries between the axial part and the appendage lower part across these sports. The implication of the results is that most injuries in basketball affect appendage upper limb caused by the ball, the rim and or backboard [26-28]. It is therefore necessary to develop strength training, flexibility and train on the mechanics of handling play equipment. Tapping/strapping of the fingers is also necessary. Coaches should ensure that protective devices are used by players. Furthermore, the skill of dunking in basketball should be discouraged especially among shorter players as it has been reported to be a risk factor in basketball especially on finger or on spinal column.These findings confirms that pattern of injuries within the sports is determined by gender of the participant hence measures of prevention should be based on gender characteristics. Results between sports showed that only axial part and appendage lower limb among basketball females, appendage upper limb among handball males and axial part among volleyball males were significantly different. It attests that pattern of sport injuries is influenced by the sport. The conclusion derived from the above analysis is that pattern of sport injuries is influenced by the nature and characteristics of a particular sport together with gender of the participant. These conclusions are in tandem with other studies. For example, Piry et al., [29] results showed that the incidence of injuries in elite Asian handball players is quite high and prevention should focus on ankle and knee injuries. In soccer, sport injuries mainly affect head and the lower extremity [30]. The upper and the lower extremity were found to be the most sites of sport injuries in volleyball [18] with equipment/facility as the main cause of injury [25,31]. Most injuries in basketball, handball and volleyball affect fingers, head and leg with finger in the upper extremity and ankle in the lower extremity as the main sites [32,2]. According to Dietch et al, [33] and Njororai et al.,[34] pattern of sport injuries is specific to a sport. Indeed ankle injuries are the most common areas affected in Basketball, Handball and Volleyball [35].McKay et al.,[36] found that ankle injuries occurred at the rate of 3.85 per participation and the three identified risk factors and landing should be considered when preventative strategies for ankle injuries in Basketball are being formulated.The results (Table 2) support previous findings in basketball [19], basketball and volleyball [37], handball [38] and volleyball [15]. It was found that injuries of the head and chest were more common in basketball and handball while injuries of the lower back were mostly common in basketball and volleyball. Injuries to the shoulder were more common in handball and volleyball while those of finger and elbow were more common across the three sports and the genders. Verhagen et al., [9] ankle sprain is the most common injury in Volleyball accounting for 41% of all volleyball related injuries. Previous injury seems to be an important risk factor for ankle sprain. Injury prevention programme should focus on ankle sprains and concentrate on players with previous ankle sprains. Sport injuries on the hip and thigh were more common in basketball and volleyball and those of the knee and ankle were common across the three sports and also genders. The findings agree with the results of [39] that nature of sport influence anatomical location of injuries. Therefore prevention strategies should address characteristics of a sport and take cognizance of the participating gender. The findings show that the site of injuries is sensitive to specific to needs and demands of a particular sport. Gender orientation also influences the anatomical location of a sport injury [19].The analysis of the site of injuries (Table 3) within the sport showed there was a significant difference on injuries to the head, shoulder, finger and the knee for both genders in basketball. In handball, a significant difference was found on injuries to the head, chest, lower back, finger, hip and ankle in males and on the knee in females while in volleyball it was found to injuries on the head, shoulder, elbow and thigh in male and on the shoulder in female players. The findings support previous assertions that the site of a sport injury is specific to the characteristics a sport and gender [31,40]. In handball Dirk, Bouter and Geus, [41] reported that injuries are frequently located at lower extremities (54%) especially the ankle and the majority of injuries involve distortations (35%) and strains (26%). The injuries are located mostly at upper extremities with finger injuries and distortations of ankle joint reported most frequently. Therefore while the authors recommended the expediency of the principle of cross-transfer between these sports, it can only be used on the skills and techniques that cut across the sports if benefits are to be gained. However, common preventive strategies like use of prophylactic equipment and development of muscular strength and joint flexibility are recommended in all the sports.
5. Conclusions
- Based on the findings of this study it was concluded that pattern and site of injuries in these sports are similar with subtle differences that can be attributed to characteristics of each sport and gender. The differences could also be explained by the differences in training and the amount of effort and intensity portrayed by the athletes. However, coaches and players are cautioned that the pattern and sites of sport injuries cannot be generalized since every sport has its own characteristics that form a basis for its training. Consequently, studies are needed to determine the training regimen of athletes in Basketball, Handball and Volleyball as this may shed more light on whether there is a relationship between strength training, frequency of training and competition on the occurrence of injuries. Therefore, it is recommended that studies be delineated on the determinants of the pattern of injury for specific sport and gender .There is need to establish factors that determine injuries on the particular part of the body, the role and position of a player in the team. It is necessary to establish the effects of training on the pattern of sport injuries that are important in developing effective injury prevention programs.