-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Journal of Health Sciences
2012; 2(4): 23-28
doi: 10.5923/j.health.20120204.01
Overweight and Obesity Prevalence and Physical Activity among Moscow Schoolchildren
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-Text HTML
Full-Text HTMLGurevich K. G. , Burdukova E. V. , Pustovalov D. A. , Oranskaya A. N.
UNESCO chair, Moscow State University of Medicine, Dentistry, Moscow, 127473, Russian Federation
Correspondence to: Gurevich K. G. , UNESCO chair, Moscow State University of Medicine, Dentistry, Moscow, 127473, Russian Federation.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
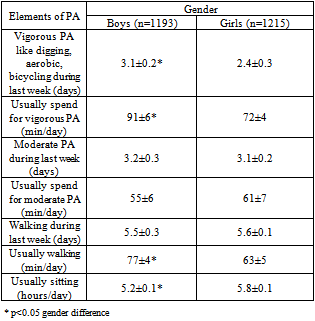
15067 Moscow school-age children and adolescents (6-17 years old, 7760 boys, and 7307 girls) were examined. From age of 10- 13 years old numbers of girls with underweight growth up to twice. In boys group number of schoolchildren with underweight was just the same. Instead of girls, number of boys with underweight was stable. Number of girls with overweight (without obesity) was higher 20% of population except age 16-17 years old. Peak number of girls with obesity registered in age 8-14 years old. In age 11, 13-14 years old number of girls with overweight was higher than 25%. Number of boys with overweight (without obesity) was some lower then number of girls; it also was near 20% of populations. The highest levels of overweight were registered in age 12-13 years old. Boys’ physical development demonstrated to be ahead such of girls. The flexibility of the boys was reduced in comparison with girls. At the same time the boys had the best indicators of physical development and coordination of movements. With age significantly increased physical performance of school children: it was increasing in flexibility, in improving speed of visual-motor reaction.
Keywords: Schoolchildren, Obesity, Physical Activity
Article Outline
1. Introduction
- Control and management of functional reserves and psychophysical human health will always be relevant and highly complex scientific and practical problems. After generation of the population follows each other in a relatively short time scales even in the life of one man. In this sense, one lost to improve the recovery of children and adolescents five years or a maximum of ten years already wrapped almost hopelessly lost in the valeological sense generation. Thus, it is important to maintain the health of children for schooling, because after it ended they still need to either further study or work activity[1], [2], [3].Long-term trend of deteriorating health of children and youth entails a subsequent decrease in health in all age groups, and further affects the quality of manpower, the reproduction of generations. Since the early 1990's trend towards worsening indicators of health, in particular, an increase of psychosomatic disease of adolescents and youth, especially in graduation classes of major cities and industrial cities. In 2008 number of children with chronic diseases increases on 4.7% compared with 1998. The mass screening of students found that among healthy children can be attributed only 34% of the studied, with high risk of developing chronic disease and severe functional violationscan be attributed most (52%) examined children[3].During the school time the number of children with myopia increases 5 times, disorders of the locomotor apparatus increases in 1,5 times, diseases of the nervous system increases in 2 times. 33% of youths who were released from service in the Armed Forces have mental disorders. 77% of students are at high level of influence of pollutants and 68% have high levels of CO2. In these children there is the heavy breathing, shortness of breath, dry cough, and rhinitis are more likely than other students. Children affected by high levels of CO2 are more vulnerable nasopharynx than their peers, they were 3.5 times higher at risk of nocturnal dry cough and a 2-fold higher risks the development of rhinitis[1], [3].During puberty there are changes at all levels, especially in the biological, as well as psychologically and socially, changing the intensity of physiological processes, hormones, function of organs. Skeletal growth is faster than the development of muscle tissue, hence the awkwardness, disproportionately, the angularity of the figures. In girls there was increasing fat mass by 10-20%, which is subjectively experienced by them very difficult. Heart volume is increased puberty twice, while there are significant variations in blood pressure, often upwards, frequent headaches. Doctors often put adolescents diagnosed: vasoneurosis[1].The propose of this work was to study physical activity and overweight among Moscow schoolchildren.
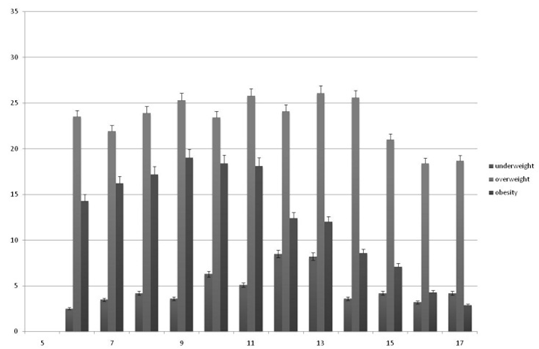 | Figure 1. Percent of girls with underweight, overweight and obesity due to age |
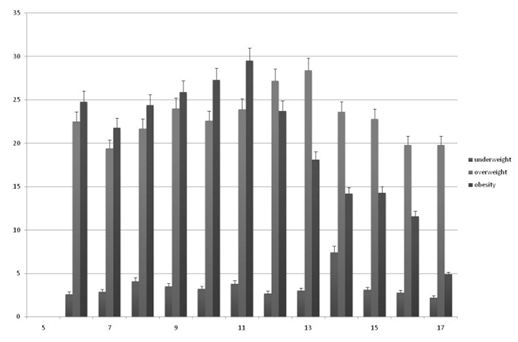 | Figure 2. Percent of boys with underweight, overweight and obesity due to age |
2. Material and Methods
- School-age children and adolescents were examined (2010-2011). Beforehand, written informed consent was signed by parents confirming participation of their children in that investigation. The work was approved by local ethical committee of Moscow State University of Medicine and Dentistry.Totally we include in investigation 15067 Moscow schoolchildren from all Moscow regions, 7760 were boys and 7307 were girls. Height and weight data were obtained from participants (6-17 years old). BMI (body mass index) was calculated for each of data pair. Derived data was analysed according to the World Health Organization growth charts, for gender and age (at the children last birthday)[4]. Participants were considered to be obese if their BMI was ≥ 95 percentile. Overweight was defined if the person had a BMI < 95 and ≥ 75 percentile. Those with a BMI ≥ 25 and < 75 percentile were considered to be the normal weight group. And those with BMI < 25 percentile considered to be the group with underweight. We applied a median index for the overall age groups’ assessment.Further examination including waist circumference and hip circumference, and skinfold thickness measurement were done. Skinfolds were measured in three standard points: triceps (TSF), subscapular (SSF), abdominal (ASF). TSF was assessed in the upper third of the upper arm’s back (posterior) surface. SSF was assessed at the end of the lower (inferior) angle of the shoulder-blade (scapula). ASF was done on umbilicus level along the midclavicular line. Those anthropometric data proved classification of schoolchildren in groups with underweight, normal weight, overweight or obesity due to individual proportions of body due to international recommendations [4], [5]. We measured blood pressure (BP) and heart rate (HR) before and after physical activity. With the help of spirometer we measured lung capacity (LC). We performed the following functional tests: motor coordination (determined in the test by throwing at the wall and catching the batted ball from a distance of 3 meters), the timed inspiratory capacity (breath holding at inspiration in the sitting position), flexibility (in cm below the floor level). Evaluated the physical performance as pushups and press (number of times within 30 seconds). Using a computerized program calculates the index of physical health (IPH)[2].Usual daily physical activity was detected using Russian version of IPAQ questionary as it early described[6].Statistics included the Student’s T-test, Wilcoxon-Mann- Whitney U test and F-Test. Pearson chi-square analysis and standard adjusted residuals calculated to determine sample characteristics. Also we used correlation and regression analysis [7]
3. Results
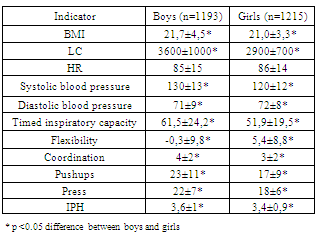
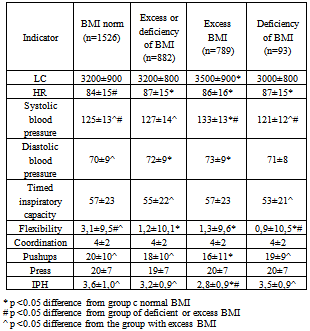
- Number of girls with underweight was about 5% in population (Fig 1). From age of 10- 13 years old numbers of girls with underweight growth up to twice. In boys group number of schoolchildren with underweight was just the same. In stead of girls, number of boys with underweight was stable (Fig 2). Only in age 14 years old we saw increasing number of boys with underweight.Number of girls with overweight (without obesity) was higher 20% of population except age 16-17 years old. Peak number of girls with obesity registered in age 8-14 years old. In age 11, 13-14 years old number of girls with overweight was higher then 25%. Number of boys with overweight (without obesity) was some lower then number of girls; it also was near 20% of populations. The highest levels of overweight were registered in age 12-13 years old.Number of girls with obesity is growing up from age 6 to 9 years old. In age 9-11 years old girls’ population we demonstrated the highest levels of obesity prevalence (about 18%). Number of girls with obesity decreases from 11 to 17 years old. In 16-17 years old number of girls with obesity is lower than 5% of population. Number of boys with obesity is growing up from 6 till 11 years old. In age of 11 years old number of boys with obesity is higher (28%) then those in girls. In age 11-17 years old number of boys with obesity decreases.Boys 14-17 years old had significantly higher BMI than girls of the same age (Table 1). This led to an increase in systolic and diastolic blood pressure reduction alone, which may indicate the existence of boys’ imbalance regulation of the cardiovascular system. The flexibility of the boys was reduced in comparison with girls. At the same time the boys had the best indicators of physical development and coordination of movements. Therefore, the index of physical health in boys was higher than in girls.
|
|
|
|
|
|
4. Discussion
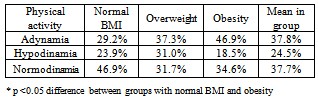
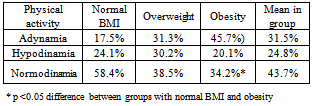
- Obesity in children and adolescents has become one of the most globally challenging medical problems over the past decades[8], [9], [10]. It is acknowledged that several serious consequences of excess weight occur in adults with the most common being cardio-vascular diseases and glucose metabolism disorders[11]. To the present it has also been demonstrated that different deviations from a healthy condition have been observed[9], [12]. Another unfavourable consequence related to childhood obesity is that there is a strong tendency for the continuation of obesity in adulthood [9], [13]. That is why public health specialists today predict a pessimistic morbidity and mortality expectation for future decades of adults[8].Childhood obesity has become an epidemic on a worldwide scale[10] and it continues to increase[11]. Several serious consequences of excess weight occur in adults with the most common being chronic non-communicable diseases [13]. Anthropometric measurements as BMI are important for epidemiological investigations of obesity prevalence. Anthropometric indexes can best predict childhood obesity[8], [9].In spite of a wide range of investigations and reviews that consider the early onset of on excess weight problem from various perspectives, we didn’t find works on detailed analyses of the relationship between obesity and age in children and adolescent populations. It is also evident that there is a lack of data the prevalence of obesity in specific age groups in the Russian Federation in general. The last statistical data that was presented in the works of Peterkova V.A. (data from 1999-2001)[14], Popkin B.M. et al. (2006; data from 1995-2004)[10] and Dedov I.I. et al. (2007; period of data collection did not have a specified)[15]. Our observations of the last years demonstrated high level of obesity and overweight prevalence in schoolchildren, mainly during and after puberties[16]. Boys are more obese than girls. Early we demonstrated prevalence of a central type of adipose tissue allocation related to weight increase is observed in investigated samples of peripuberty children[17]. Considering obvious economic growth in Russia during the last several years and a strong tendency for a western lifestyle the adopter of among the Russian population, especially those dwelling in cities, an increase in obesity rates might be expected.The number of schoolchildren with overweight in RF is comparable with those in USA[18], [19]. The level of obesity in Moscow in children’s’ and adolescent’spopulation is much higher then those in European countries[20], [21], [22], and some developing countries[23], [24].According to data indicated above, the prevalence of obesity is the highest in male adolescents. Among them, the most prominent figures are registered during prepuberty and early puberty ages. In the girls prepuberty age groups have the maximum levels of obesity. The subsequently pronounced lowering of obesity levels could be explained with its relationship to a puberty growth spurt.Also we demonstrated low level of usual physical activity among schoolchildren. Number of schoolchildren with adynamia is twice higher in group with obesity in comparison with those with normal BMI. Low level of physical activity may be an additional risk factor of cardiovascular diseases development in future[25],[26].
5. Conclusions
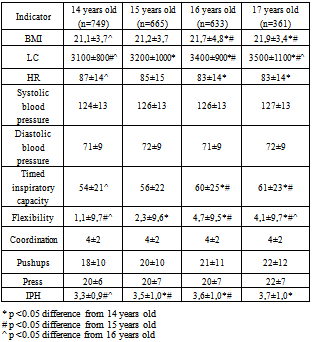
- We demonstrated corresponding between prevalence of overweight and obesity and age. It might be assumed that the highest levels of overweight and obesity are registered in pre-puberties and puberties ages. So, some hormonal mechanisms are playing role in our finding. Our results established high level prevalence of overweight and obesity in Moscow schoolchildren. We can speak about prevalence of overweight in girls’ population and prevalence of obesity in boys’ population. In comparison with the same monitoring of overweight and obesity prevalence in Moscow schoolchildren population we done 3 years ago[17], number of boys with overweight and obesity seems to be the identical. In the same time, number of girls with overweight and obesity increase. In any case we have to speak about critical levels of overweight and obesity in population of Moscow schoolchildren. Such high levels of obesity and overweight in schoolchildren population might influence on serious public health problems in future.We have studied the relation of physical health of schoolchildren with the peculiarities of their development. Shown that the maturation of schoolchildren accompanied by an increase of IPH. At the same time increases the mean value of BMI, which may indicate an increase in the intensity of risk factors for cardiovascular disease.
ACKNOWLEDGEMENTS
- The work supported by grant of President RF MD- 1594.2012.7