-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Food and Public Health
p-ISSN: 2162-9412 e-ISSN: 2162-8440
2020; 10(1): 7-18
doi:10.5923/j.fph.20201001.02

Factors Associated with Utilization of Postpartum Care Services in Luanshya District
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMwangala Simataa 1, Alfred Makani 2
1Public Health, Mufulira Nursing School, Mufulira, Zambia
2Health Policy and Economics Levy Mwanawasa Medical University, Lusaka, Zambia
Correspondence to: Mwangala Simataa , Public Health, Mufulira Nursing School, Mufulira, Zambia.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Utilization of postpartum services is a major concern worldwide due to the great impact it has on infant and maternal mortality. Postpartum is defined as the first six weeks (42 days) following delivery of an infant. Care during this time is for the health and survival of the mother and the new born. Current estimation of Luanshya postpartum coverage of first postpartum care is 15% which is far below the recommended 80% by WHO. This study was therefore aimed at determining the factors associated with utilization of postpartum care services in Luanshya District. An analytical cross-sectional study was conducted on 187 mothers taking the children to the clinic aged between seven weeks to three months. Data was collected using questionnaires having both closed and open-ended questions. Stata 11 was used for statistical analysis of quantitative data. Qualitative data was explored for emerging themes and the frequency of themes were quantified. Chi-square was used to determine association of the variables. Logistic Regression analysis was used to ascertain which variables significantly affected the dependent variable. The findings from this study revealed that postpartum attendance was very low and stood at 27.8%. The major factors associated with low utilization of postpartum services were: postponement of sixth day postpartum care for Bacillus Calmette Guerin (BCG) (46%), feeling ill after delivery 29.4% and tradition 62.8%. This study demonstrated that there are gaps in the utilization of postpartum care services. Capacity and accessibility of health systems as well as cultural and religious practices are areas that affect postpartum care and hence should be worked on especially at community level. Such programs should include male involvement, influential family members such as grandmothers as well as traditional and religious leaders. Newborn babies should be vaccinated with BCG vaccine at birth so that the postpartum care appointments should be specifically for postpartum care.
Keywords: Post-natal care, Post-natal services, Post-natal utilization
Cite this paper: Mwangala Simataa , Alfred Makani , Factors Associated with Utilization of Postpartum Care Services in Luanshya District, Food and Public Health, Vol. 10 No. 1, 2020, pp. 7-18. doi: 10.5923/j.fph.20201001.02.
Article Outline
1. Introduction
- Utilization of postpartum services is a major concern worldwide due to the great impact it has on infant and maternal mortality. The literature reviewed has shown that the majority of perinatal deaths occur during the postpartum period. as stated by WHO and UNICEF [1], and defined postpartum as the first six weeks following delivery of an infant. It is also known as postnatal period or puerperium. According to Juma [2] postpartum services are those services offered to the mother and her baby during the first six weeks following delivery. It is a critical time for the mother and the baby. Complications may arise in this period and can lead to ill-health of the two [3] Postpartum services are an important component of obstetrics and neonatal care aimed at preventing and managing any complications that may endanger the survival of the mother and the baby [4] During this period, not only is the mother vulnerable to physical complications but also psychological disturbances which may be aggravated by adverse social circumstances such as lack of understanding of their own situation and lack of emotional support from the partner and their family [4].World Health Organization (2011) stated that up to 3.1 million new born deaths that occurred in 2010 could have been prevented if mothers and newborns received efficient postpartum services. The world estimation of postpartum coverage was at 35% compared to nearly 70% who received ante partum care in 2008. [5] Underutilization of postpartum services is a worldwide problem especially in Sub-Saharan countries [6] According to Eyler [7] 3 in every 10 mothers received postpartum care. Zambia is among the countries in the Sub-Saharan region which has a low postpartum coverage - 49% compared to high percentage of ante partum care (94%) as reported by the Zambian Central Statistics Office [3].World Health Organization at the Alma Ata International Primary Health Care Conference (Geneva) in 1978 recognized that infant and maternal mortality was a major public health problem that needed priority action [8] However, there are efforts by member countries to reduce maternal and infant mortality ratios by three quarters between 1990 and 2015 as stipulated in the millennium development goals to which Zambia is a signatory [3]. Despite the efforts made to improve the postpartum coverage in Zambia, the coverage is still below the national target which is 80%. Postpartum care comprises examination and treatment provided to women after delivery [9] It is not only for normal deliveries and those who delivered at the health institutions but also for those who had still births, premature deliveries, and miscarriages or home deliveries [3]. In Zambia, Maternal and Child Health services have been included in the essential health care package since maternal and child mortality is recognized as having a large impact on the well-being of the country [3] Postpartum Care is carried out at the sixth hour, sixth day and at the sixth week during postpartum period. [10] This approach is aimed at reducing infant and maternal mortality.
1.1. Problem Statement
- Many mothers especially in sub-Saharan region do not receive postpartum care after delivery and the ultimate result is increased infant and maternal mortality rate [11], the quality of care given during postpartum period can determine the outcome of the mother’s health after delivery. The complications that occur in puerperium such as postpartum hemorrhage, infection, chronic pain, impaired mobility, and damage to reproductive system organs contribute 73% to maternal mortality estimates in Zambia [12].In Zambia, infant mortality ratio stands at 76/1000 live births and maternal mortality ratio is estimated to be 483/100,000 live births [13] Despite the reduction from 591/100,000 in 2007, it is still unacceptably high. Hence the intensified efforts in maternal health services to reverse the high trend of mortality. According to Kozier [11] about 51% of postpartum women do not receive postpartum care. Suffice to say that the national target is 80% and anything below 70% needs serious interventions. Luanshya district is no exception to this trend. Which estimated its postpartum attendance at 40%. Out of the expected 40%, only 15% received care on their appointment dates. However, ante partum attendance was at 92% [13]. This clearly shows a remarkable gap between the mothers who attend antenatal clinics and those who go back for postnatal services after delivery.It is therefore critical to investigate the factors that deter mothers from utilizing postpartum services, as this would aid in devising strategies to improve the coverage, hence the need to conduct a study in order to critically establish the factors associated with the gap. The main factors that influenced the problem could be the following: Level of knowledge, accessibility of postpartum care services, attitude of postpartum mothers, Quality of postnatal care services, cultural and religious beliefs. The relationship among the variables is shown in the conceptual frame work (figure 1.1).
1.2. Justification of the Study
- Maternal and infant morbidity and mortality has taken a toll in Zambia today especially in the first week after delivery. Therefore, the first six weeks after delivery is critical in determining the healthy survival of women and their newborn babies [14]. According to the district Health Management Information System (HMIS) 2011, out of the expected 40% postpartum coverage, only 15% received care on their appointment dates. This estimate is far much lower than the national target (80%). Therefore, there was need to explore the factors associated with utilization of postpartum services by mothers during the postpartum period in Luanshya district. This study was aimed at adding more information about postpartum care services to the body of knowledge. This would also help Ministry of Health to plan for effective strategies to improve the postpartum coverage. The information on this study would provide impetus or act as catalyst to the Ministry and other partners in the health delivery system to plan for a holistic approach regarding utilization of postpartum services and eventually reduce on infant and maternal mortality rates. At the time of preparation for this study there was no record of a study done on utilization of postpartum services in Luanshya district hence this study.
1.3. Research Question
- What are the factors that may be associated with utilization of postpartum services in Luanshya District?
1.4. General Objective
- To determine factors associated with utilization of postpartum care services at Luanshya Health Centers.
1.4.1. Specific Objectives
- a) To establish the level of utilization of postpartum service and its accessibility to postpartum mothers.b) To assess the knowledge of postpartum services among postpartum mothersc) To determine attitudes towards postpartum services among the postpartum mothers and the health providersd) To identify cultural and religious beliefs related to utilization of postpartum care.
1.5. Conceptual Framework
- This study was guided by Andersen’s Health Seeking Behavioral Model developed in 1968 [15] Andersen model is a conceptual model aimed at demonstrating the factors that lead to the utilization of health services; it is determined by the following three categories: Predisposing factors: These characteristics exist prior to a health event. These characteristics are such as formal education, attitude and knowledge towards the health services, age, parity and marital status. According to Andersen, an individual is more likely to use health services based on demographic, positions within the social structure and beliefs of the health service benefits. An individual who believes that health services are useful for treatment is likely to utilize those services.Enabling factors: This category includes resources found within the family and community. Family resources comprise economic status and the location of community resources. These characteristics are such as: access to health facility, Availability of services, availability of health personnel, financial resources, health insurance, social network and support.The Need based factors:The need-based factors generate towards the utilization of health care services. This category includes the perception of needs for health services whether individual, social, or clinically evaluated perceptions of need. These are such as perception of severity or how one views their own general health and evaluated needs represented by professional judgment [15]. The model was meant to discover factors that facilitate or delay utilization of health services and ultimately develop a measure of access to health services. The model provides framework for understanding the potential influence on an individual’s decision to make use of available health services. The Behavioral Model adopted is depicted in the conceptual framework figure below.CONCEPTUAL FRAME WORK
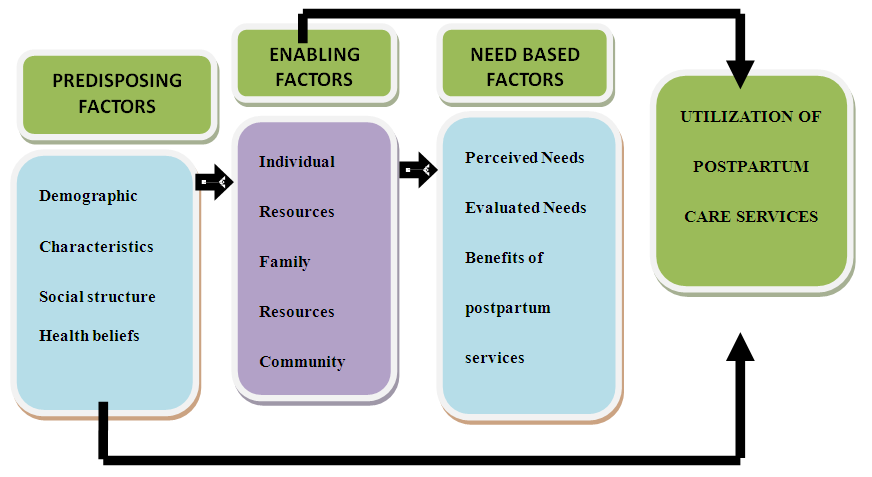 | Figure 1.1. Andersen’s Health Seeking Behavior Model (Source: Kolinsky, 1988) |
2. Research Methods
- The study was carried out in Luanshya district at five main government health centers which are: Mpatamatu Health Centre located 22 km from the health office with the population of 28,104 people, Mikomfwa Health Centre located 6 km from the health office with the population of 29,490 people, Luanshya Main Health Centre 2 kilometers from the health office with population of 19,396, Roan section 9 clinic which is 7km from the health office with the population of 18,802, Mikomfwa Urban Health Centre which is 6km from the health office with a population of 15,438. These health centers are among thirteen government health centers in Luanshya. There are seven private health centers, three hospitals and thirteen government health centers.Luanshya District is situated on the Copper- belt Province of Zambia with the population of 156,059. Luanshya is about 35 km from the provincial capital (Ndola) and 360 km from the capital city of Lusaka. It shares borders with Ndola, in the east, Kitwe in the North West, Masaiti District in the South and the bank of Kafubu River in the southeast. The district covers 935 square km area. The central part of the district is situated on the 1,225 contour levels and the highest point is the Mpata hills in the west at 1,372 meters high.
2.1. Study Population
- The study population comprised of women aged 18-49 who took their children aged 7weeks-Three months for children’s clinic. It was assumed that this group would give accurate information on postpartum activities. The current population of Women in child bearing age was 34,332 and expected live births were 1785.This study was an analytical cross-sectional study.
2.2. Inclusion Criteria
- All women aged 18-49 years of age who were bringing their children to Mikomfwa Urban Health Centre, Mikomfwa Health Centre, Luanshya Main Health Centre, Roan Section 9 Health Centre and Mpatamatu Health Centers for children’s clinics. Postpartum women from Mikomfwa Urban Health Centre, Mikomfwa Health Centre, Luanshya Main health center, Roan Section 9 Health Centre, and Mpatamatu Health Centre.With babies aged seven (7) weeks of age up to three (3) months of age were included in the study.Only mothers from Mikomfwa Urban Health Centre, Mikomfwa Health Centre, Luanshya Main Health Centre, Roan Section 9 Health Centre and Mpatamatu Health Centre who consented to the study were allowed to participate in the study.
2.2.1. Exclusion Criteria
- Women from Mikomfwa Urban Health Centre, Mikomfwa Health Centre, Luanshya Main Health Centre, Roan Section 9 Health Centre, and Mpatamatu Health Centres who did not consent to the study were not involved in the study.
2.3. Sampling
- Purposive method was used to select the five health centers: These were the busiest centers and had the largest catchment population so as to capture as many postpartum mothers as possible.The participants from the sampled centers were selected using convenient method: where by all the mothers taking the children to the clinic aged between seven weeks to three months were selected.
2.4. Sample Size Calculation
- The minimum sample size required to determine the prevalence of postpartum attendance in Luanshya district was calculated using open epi version 3.03 at 95% confidence interval level as shown below (http://www.openepi.com/SampleSize/SSPropor.htm). An estimate of 0.15% prevalence was used from a total of 1785 women attending antenatal clinics from the clinic records. The sample size calculated was 177. However; ten more women voluntarily took part in the study giving a total of 187 available for the study.EquationSample size n = [DEFF*Np (1-p)]/ [(d2/Z21-α/2*(N-1) +p*(1-p)]Where:N = Population size (for finite population correction factor or fpc) (N): 1785p = Hypothesized % frequency of outcome factor in the population (p): 15%+/-5d = Confidence limits as % of 100(absolute +/- %)(d): 5%1 = Design effect (for cluster surveys-DEFF): 1Sample size for this study was therefore 187Confidence interval (95%)The sample was divided into 5 selected health centers which gave 37 mothers from each selected health centre.
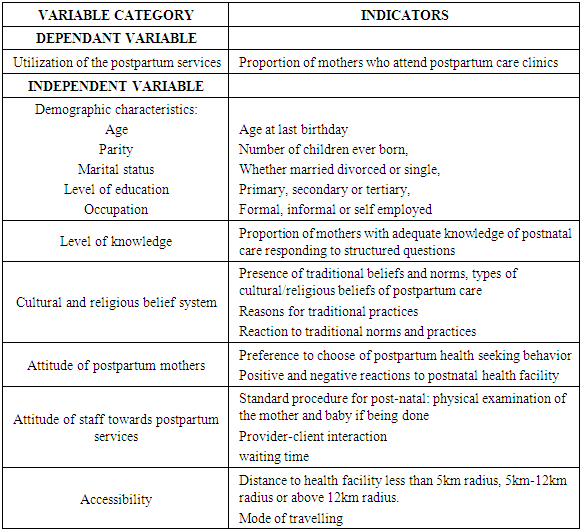
2.5. Variables
- The variables are illustrated in the table below with the indicators.
|
2.6. Data Collection Methods and Tools
- A structured interview schedule was used to get information directly from the respondents. This method was convenient because not all the mothers were literate to read for themselves. Structured interview questionnaire was used comprising closed and open ended, open ended questions were used to obtain the qualitative information. Questionnaires comprised 20 questions generating 31 variables.Interview of participants using a structured interview questionnaire with the help of two trained research assistants was done at the five selected health centers during under five clinic for 22 days spread over a period of three months, where an average of eight questionnaires were administered per day.
2.7. Validity and Reliability
- Two research assistants were trained to minimize intra and inter observer biasness. The instrument was pre- tested in a pilot study to determine if the desired information was going to be achieved. Contents of the questionnaire were reviewed by the principal and co-research supervisors. An extensive editing and review of literature was conducted before compiling the questionnaires.
2.8. Pilot Study
- A pilot study was conducted at section 26 Health centre in Luanshya. The pilot study was conducted on 10% of the total sample (10% of 187= 18.7). This was to test the data collection tools for validity, reliability and to avoid bias. It assisted to obtain clarity and guide the direction of the main study. A pilot study enabled adjustments to be made to the questionnaire before the major study was carried out.
2.9. Ethical Considerations
- The researcher ensured that all ethical and legal implications were addressed. Ethical Approval was requested from the Excellence in Research Ethics and Science (ERES) an institutional review Board (IRB). The Ministry of Health and the District management of Luanshya granted authority to conduct the study at five health centres of Luanshya district through the District Health Office. Rights of Respondents-Written Informed consent form was obtained to allow voluntary participation. The respondents were availed with information regarding their rights whether to accept participating in the study or not for them to make an informed choice. Benefits to Respondents-The purpose and benefits of the study was communicated to respondents in order to clear out any misconceptions they could have about the study before the mothers got involved in the study. All respondents were availed with information regarding direct and indirect benefits. The researchers explained to the respondents about the importance of the research towards improving the quality of health delivery for their wellbeing and their babies. It was explained to participants that the study would benefit the community by coming up with effective strategies for improving postpartum services. Confidentiality-Respondents were reassured that all information provided by the respondents would be treated with utmost confidentiality. The information obtained about the participants remained confidential and was kept in a safe place under key and lock. The questionnaires were kept for five years before being disposed of. Anonymity-Anonymity of participants was maintained by not using names on the questionnaires. This anonymity was guaranteed by virtue of the respondents not disclosing their names and where they came from in terms of their house numbers.Privacy-Privacy was maintained by interviewing participants in isolated rooms and data not Shared with other people. Above all, the interviews were carried out in exclusive places where others could not hear the discussion. Justice-Participants were treated fairly regardless of who they were in the study. They were informed that they could withdraw any time if they so desired. The participants were not exposed to any kind of discomfort or any form of harm: physically, psychologically or exploitatively.
2.9.1. Data Entry and Analysis
- EpiData version 3.1 was employed to create questionnaire databases for double entry and validation. Excel was used for certain elements of graphical documentation. Data was then exported to Stata for analysis. Stata 11.0 was used for all data statistical analysis. Qualitative information from open ended questions were analyzed and interpreted using mixed methods principle of conversion by transforming qualitative into quantitative data. Responses from open ended questions were explored for emerging themes. The information was then converted to quantitative data by quantifying the frequency of identified themes in order to interpret and understand the emerging themes.In investigating whether the independent factors affected the dependent variable (Mothers’ utilization of postpartum care) cross tabulation or bivariate analysis was done to extract factors that were crudely associated with utilization. Utilization in this study is defined as having attended the 6days postpartum care appointments. Chi Square statistic and p values were obtained as indicated in table 3.2.
3. Results and Discussion
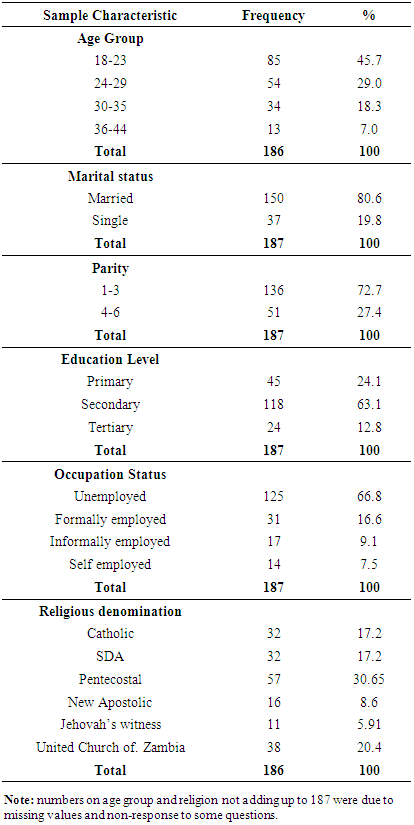
3.1. Demographic Characteristics
- A total of 187 mothers participated in the study. Table 3.1 Shows that the majority of the women were in the age group 18 to 23 (45.9%), married 150 (80.25%) and had 1-3 children (72.7%). High proportions of these women had attained secondary school education 118 (63.1%) and were unemployed 125 (66.8%).
|
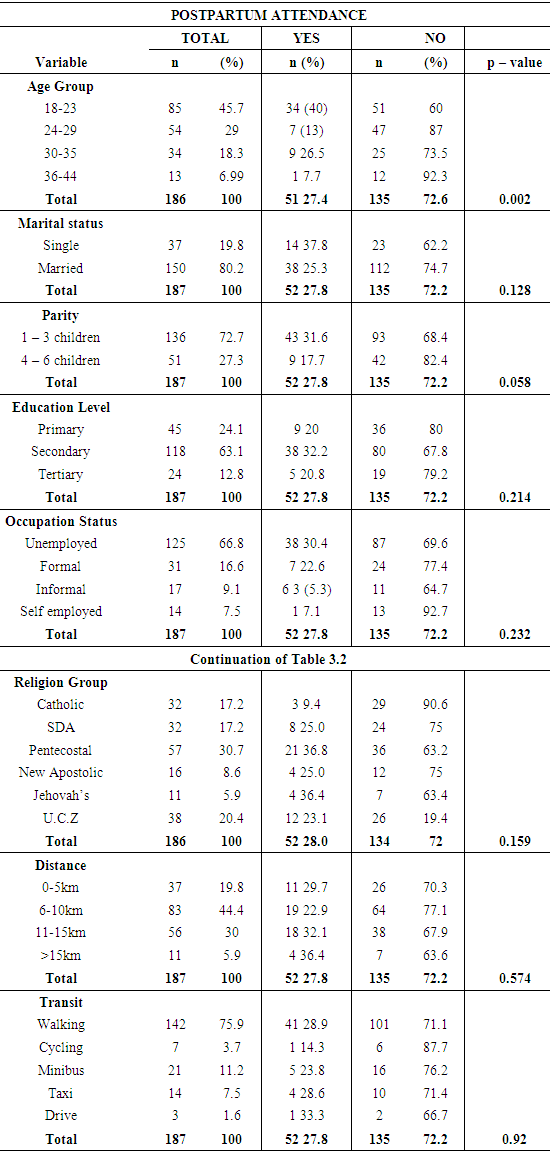
3.2. Access and Utilization of Postpartum services
- The association between postpartum visits and the independent variables is shown in table 3.2 below. The table shows that only age group (p - value = 0.002) and parity (p - value = 0.05) were significantly associated with utilization and were therefore included in the multivariate regression model. The Likelihood ratio test was then performed to assess whether the regression model with age group and parity had a better fit than the models with only either independent variables. The Likelihood ratio test determined that the model with only age group (p - value = 0.006) better described the pattern of attendance of post-partum care in this study.
|
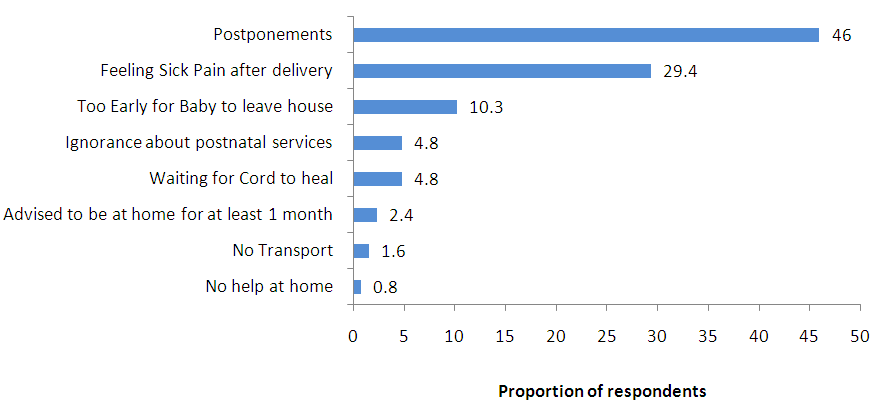 | Figure 3.2. Reasons for not attending postpartum services |
3.3. Knowledge and Attitude towards Postpartum Care
- The women were asked to explain what they understood by the word postpartum care in their own words and they responded as shown in figure 3.3.
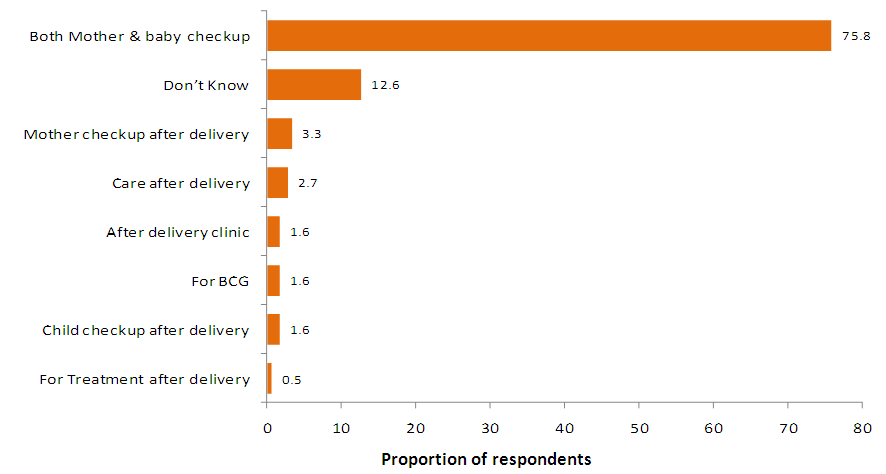 | Figure 3.3. The meaning of postpartum care |
|
3.4. Religious and Cultural Beliefs
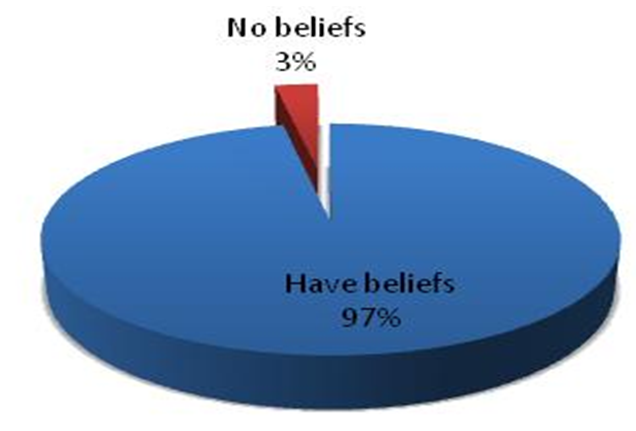
- When asked whether beliefs existed, women responded as shown in Figure 3.4 which shows that most of the women (97.3%) acknowledged the existence of cultural beliefs in their communities while 3% said there were no beliefs.
 | Figure 3.4. The existence of religious and cultural beliefs |
 | Figure 3.5. Religious and cultural beliefs |
3.5. Demographic Characteristics
- This study shows that most of the respondents were young mothers aged 18-23 (45.7%). The majority were married (80.2%) and it can be argued that they might have received some support from their partners and the members of the community without being stigmatized, A study conducted by WHO in Mali revealed that the people close to the mother have great influence on the choices she makes regarding her health and that of her baby. The study demonstrated that grandmothers had more knowledge on maternal health and this reduced infant mortality. The study also concluded that husbands who were more informed on maternal and child health were supportive to their wives [5,16].Many respondents had reached secondary level of education (63.1%) and most of the mothers were not employed (66.8%). Therefore, the fact that these had more time to go to the clinic than the women in employment could be justifiable. In terms of parity, majority of the respondents had 1-3 children (72.7%). Similarly [8] Kogan and Leary (1990) in their study found that 82% of women with 1-3 children went back for postpartum care, although this is slightly higher than what was found in this study. The explanation for this trend could be probably that experience, knowledge and confidence on maternal and child health are gained as one bear more children. These demographic results also tally with the study by (WHO and UNISEF) [1] which found that demographic status of women may influence their visits to the health facilities. This could be due to long distance, domestic pre-occupation, and the culture of seclusion.
3.6. Accessibility and Utilization of Postpartum Services
- Access to health care may be influenced by many factors among them availability of the service, knowledge on the service, economic factors as well as religious and cultural factors. The study revealed that the prevalence of postpartum attendance at 6 weeks for Luanshya district was 27.8% and is very low compared to other studies in the region especially that Luanshya is urban; Similarly, it was also found by CSO, 2007 that very few women (50%) receive postpartum care after delivery. Those who went for sixth week postpartum visit were more (57.2%) than those who attended the sixth day (27.8%) postpartum visit. The proportion at six weeks in the ZDHS survey compares well with what was obtained in the study. This could be that by the sixth week most mothers had recovered from the birth trauma as stated in the study done by Ingalls [17].The study found that age group and parity were significantly associated with postpartum utilization. However, age group had more effect on attendance of post-partum care in this study. The explanation for this could be that the younger age group lacks the necessary experience when it comes to child bearing and hence they easily follow instructions and advice from the health facility. This is in line with other studies that have attributed low postpartum attendance to parity and in a study by Kogan [8], younger women (parity 1-3) utilized postpartum services more compared to the older generation. This can also be explained by the effect of traditions and culture on populations which may have more effect on the older women than the younger ones. The younger mothers have a lot of access to information such as social media due to their exposure to secondary education. The other possibility is the education sector support to the girl child which makes them comfortable to access health services as they can go back to school after delivery.With regards to socio-economic status, this study found that the status of the mother had no effect on the mother’s choice to utilize postpartum services. This is contrary to other studies done on the same topic by other researchers. In their study Kogan [8] also found that low social economic status of the women hindered them from utilizing postpartum services. Andersen Seeking behavioral Model illustrated socioeconomic status as an enabling factor in which one depends on resources available [15].Some barriers reported by the mothers were postponement of days for BCG by the caregivers (46%), followed by feeling sick (29.4%). A bulletin by WHO [5] revealed that immunization is one of the effective interventions that can reduce up to 24% of the infant mortality. However, findings from this study show that the immunization program especially for BCG is usually postponed in the clinics. Postponement or delay in attending to clients can discourage the mothers from going back to the health institution for postpartum care. This may imply that the mother and the child are at risk of increased morbidity and mortality. This suggests that the quality of the health care that mothers are receiving may not be adequate. WHO [5] concluded that if health care is considered inadequate, then it may not be utilized. There is need to pay more attention to the delivery of the BCG vaccines as this is affecting women’s utilization of postpartum services. The reason for feeling sick during the first six days could be that they were still recovering from labour and delivery pains. Similar to these findings, is the study by Perry (2004) who stated that 80% of women are still in pain during the 1st week of delivery.
3.7. Knowledge and Attitudes towards Postpartum Care
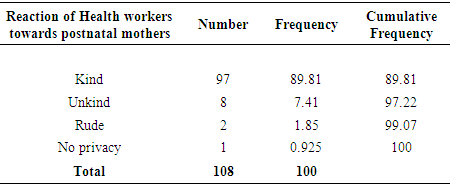
- The women were asked to explain the meaning of postpartum care; the respondents gave the following responses: The majority (75.8%) knew what the meaning of postpartum care was. The proportion of those who did not know what postpartum care was, were 12.6%. The respondents were also asked how they were welcomed at the postpartum clinic and the majority (94.3%) of the women said they were welcomed kindly. These results defeat the WHO statement which assumes that the women may shun postpartum service because of unkind attitude of health workers at health care centres [6]. In our study however, indicated that the attitude of the health workers was kind, unlike the findings from the WHO study.
3.8. Religious and Cultural Beliefs
- The majority (97.3%) acknowledged the existence of traditional and religious beliefs. This is in line with the statement by Postmontier, Kaewsarn and Jafarey [18,19,22] which says that the postpartum period, is generally filled with ‘do’s and don’ts of which 90% of postpartum mothers practice cultural beliefs. Some of these beliefs can interfere with the use of valuable postpartum services. The majority (62.8%) were traditionally advised to stay in the house for one to three months, followed by those who were advised to keep the baby in the house until the cord healed (13.3%). CBOH, (2003) also found that most of the mothers follow the tradition and not medical advice. A similar study by Jafarey which was done in Uganda also revealed that a cultural belief is an important predictor of postpartum service utilization [20] In the study by Juma [21], it found the same influence of cultural beliefs on postpartum utilization. Therefore, were compelled to recommend that efforts should be made in order to incorporate beneficial cultural beliefs into health care delivery where perception such as not doing heavy work until the woman fully recovers. In so doing it might enhance quality care services.
4. Conclusions
- Findings from this study show that accessibility and utilization of postpartum services is quite low compared to the 80% for developing countries. Although most women knew what postpartum care was, this did not translate into them seeking the service hence the low coverage. Postponement of postpartum care dates for BCG Vaccination was a major barrier to utilization of postpartum services in Luanshya district. Religious and cultural beliefs such as seclusion were found to be factors that affected women’s utilization of postpartum services. Contrary to other studies, findings from this study demonstrate that a health care provider attitude towards postpartum mothers was generally acceptable.
5. Recommendations
- Based on the above findings, the following recommendations were made;1. Infants should be vaccinated with BCG at birth to avoid compromising the appointment of 6th day postpartum visit for BCG vaccination. 2. Health services should be taken as close as possible to the hard to reach areas.3. Strategies should be put in place to follow up postpartum mothers on the 6th day postpartum visit and Community education programs should be intensified. This should be done through involvement of the community outreach or mobile programmers.4. There is need for programs that will address the religious and cultural barriers to postpartum care. Such programs should include male involvement. Influential family members such as grandmothers as well as traditional and religious leaders should be targeted.
ACKNOWLEDGEMENTS
- We sincerely thank the two data collectors who made our work possible.