-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Food and Public Health
p-ISSN: 2162-9412 e-ISSN: 2162-8440
2019; 9(4): 111-118
doi:10.5923/j.fph.20190904.02

A Pilot School-based Intervention to Increase Fruit Intake in Adolescents in Urban Benin
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLEunice Nago, Sherifath Mama Chabi
School of Nutrition and Food Science and Technology, Faculty of Agricultural Sciences, University of Abomey-Calavi, Abomey-Calavi, Benin
Correspondence to: Eunice Nago, School of Nutrition and Food Science and Technology, Faculty of Agricultural Sciences, University of Abomey-Calavi, Abomey-Calavi, Benin.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Low- and middle-income countries are encountering notable dietary and lifestyle changes referred to as the nutrition transition, as it happened in high income countries many decades ago. These changes are especially noticeable in urban areas and characterized by poorer quality diet, among others. The present study aimed at testing the ability of a school-based fruit intervention to increase the daily fruit intake of adolescents in Cotonou, a city of Benin, a low-income country. The study also examined whether the intervention affected overall daily diet, particularly intakes of vegetables and sweet foods. The intervention was designed based on findings of a previous study. It lasted 2 months and consisted in operating a fruit stall under strict hygiene conditions, in a school selected by convenience. The study used a pre-post design without controls. Baseline and follow-up anthropometric and 24-hour dietary recall data were analysed in 229 participants. Mean fruit consumption at school was 175g higher at follow-up in consumers, identified as students who ate fruits from the stall. Consumers’ daily fruit intake increased by 166g, significantly more than in non-consumers. The contribution of fruit consumption at school to consumers’ daily fruit intake rose from 3% at baseline to 78%. On average, their daily fiber intake increased significantly and fat energy contribution in their daily diet declined from 33 to 28%, a level in the normal range. Hence, the intervention is promising and could be an efficient and sustainable means to promote fruit consumption and healthy diet in adolescents in urban Benin.
Keywords: Adolescents, Healthy diet, Out-of-home eating, Nutrition transition, Low-income country
Cite this paper: Eunice Nago, Sherifath Mama Chabi, A Pilot School-based Intervention to Increase Fruit Intake in Adolescents in Urban Benin, Food and Public Health, Vol. 9 No. 4, 2019, pp. 111-118. doi: 10.5923/j.fph.20190904.02.
Article Outline
1. Introduction
- The World Health Organization (WHO) recommends to consume at least five servings (400g) of fruits and vegetables per person per day [1,2]. This intake level is sufficient for a healthy and balanced diet, and contributes to prevent obesity and many chronic diseases, such as several types of cancer [3-6]. However, high rates of low fruit and vegetable consumption, over 70%, are observed in sub-Saharan Africa [7,8], and more specifically in West Africa [9]. In Benin, a low-income country in this region, it is estimated that 93% of urban dwellers aged 25 to 64 years consume less than 5 portions of fruits and vegetables per day [10,11]. There is a need for fruit and vegetable interventions, especially in adolescents who represent 23% of the Beninese population [12,13]. In a previous study in Cotonou, the most populated city of Benin [14], a low mean daily fruit and vegetable intake of 97g was observed in adolescents in school settings while their daily intake of sugary foods was 304g on average [15]. Schools are appropriate settings for nutrition interventions in adolescents as most of them attend these places [16]. Moreover, several fruit and vegetable interventions implemented in high income countries (HIC) induced substantial increases in the fruit and vegetable intake of school adolescents [17,18]. Multi-component school-based fruit and vegetable programs, combining classroom education, behavioral change curricula, parental home assignment and food service modification, among others, are the most effective. However, they demand more financial and human inputs as well as more time and process monitoring effort. Interventions with a single environmental change component, such as increased fruit and vegetable availability, are more cost-effective [17-23]. Availability and accessibility are major mediators of adolescents’ fruit and vegetable intake in HIC [24,25]. In the study conducted among school adolescents in Cotonou, Benin, this held true, as well as food safety [26]. In this study, adolescents were more favorable to a school program on fruits only than on vegetables only or both fruits and vegetables. Consequently, a single-component school-based fruit intervention was developed and involved selling fruits in the school setting under high hygienic conditions. The main objective of the present study was to test the ability of a school-based fruit intervention, which consisted in operating a fruit stall with a high hygiene standard, to increase adolescents’ daily fruit intake. The study also examined whether the intervention would affect the adolescents’ overall daily diet, particularly intakes of vegetables and sweet foods. There are very few experiences of healthy diet promotion in adolescents in Africa. This study was expected to shed light on the potential effect of a school-based fruit intervention.
2. Methods
2.1. Design and Sampling
- The study was a pilot intervention using a pre-post design without controls. A private school was chosen in Cotonou by convenience to host the intervention. Private schools are ten times more numerous than public schools and therefore are more representative of secondary schools in the city [15]. Authorization was obtained from school authorities. All students in the selected school, from the first to the last grade (7th grade) were free to buy fruits from the stall. However, only a subsample was surveyed. Inclusion criteria were: 1) to be a 5th, 6th or 7th grader and 2) to be younger than 19 years. Reasons were that it was observed in a previous study [15] that students in grades 5, 6 and 7 were old enough (≥ 13 years) to answer survey questions properly, and that adolescence ends at 19 years according to the WHO. Fifth, 6th and 7th graders were 288 in total and 261 were younger than 19 years, thus were eligible for the surveys. Written informed consent was requested from their parents. Among the 261 eligible students, 249 effectively participated in the baseline survey. This number was sufficient for the surveys considering sample size estimation made using PASS 11 software (NCSS, Kaysville, UT). Thus, with an estimated 48g (SD 105g) mean daily fruit intake of the adolescents [15], and considering an average serving size of 100g, a 80% power and 5% precision, the minimum sampling size required to detect a pre-post difference of 0.2 serving size (worst case scenario) [18] was 217 subjects.
2.2. The Intervention
- Students were told the study was about their whole diet and were not informed an intervention with particular focus on their fruit intake was ongoing. A woman was recruited to sell a variety of good quality (ripe but not spoiled) and nicely presented fruits in the school compound. She was identified on the basis that she was looking clean and willing to continue operating the fruit stall after the intervention. The intervention was implemented as much as possible in real-world conditions, so that the stall could keep on functioning afterwards. School vending in Benin consists in offering food to students during breaks, without further advertising. Therefore, to obtain realistic effects, we did not do an aggressive promotion of the stall, nor placed great emphasis on nutrition education. Only a single leaflet about the general health benefits of fruits and vegetables was distributed to the students and teachers and sent home for the parents. The fruit vendor complied with the school regulation (including a preliminary medical check-up) to obtain accreditation as a regular vendor. She operated the stall from the morning break to the afternoon break (9:45 to 17:05) like the other vendors. Six types of fruits, selected among the ones reported as preferred by school adolescents in Benin [26] were sold: apples, bananas (not plantain), oranges, grapes, pineapples and papayas. Apples, bananas, oranges and pineapples were sold per piece. Pineapples were peeled when purchased by the students, cut in small pieces and served on clean plates. Grapes and papayas (peeled and cut in pieces) were presented in small bags, varying in size (~60-100g) according to their market price. Other products sold in the school were sweet foods (biscuits, candies, industrial and locally-made sweet beverages), cakes, prepared meals (sandwiches with egg, meat, ham, sausage, mayonnaise and/or butter, maize-based porridges with sugar and milk, rice with beans, tomato sauce and fish, egg or meat). Hygiene rules followed by the fruit vendor were defined for the purpose of the intervention based on the Beninese Code of public hygiene (like wearing clean clothes, apron and headscarf, washing hands, plates and other utensils with soap and potable water, keeping the rubbish away). A supervisor kept a daily record of fruit sales (numbers) on a monitoring form and ensured the fruit vendor complied with the hygiene rules. The intervention lasted two months and the language used was French.
2.3. Measures
- 2.3.1. Anthropometry. At baseline, weight and height of the sample was measured with portable Seca 225 stadiometres (Seca, Hamburg, Germany, precision 0.1 cm) and Seca 880 scales (Seca, Hamburg, Germany, precision 100g), according to standard procedures [27]. Participants’ age was determined from their reported date of birth. Their nutritional status was described based on the body mass index (kg/m2) and sex- and age-specific cut-offs of the International Obesity Task Force [28,29].2.3.2. Outcome measures. At baseline and follow-up, trained interviewers evaluated the daily diet of the participants during face-to-face 24-hour recalls. Food intakes reported on two non-consecutive survey days, in a single school week, from Tuesday to Friday, were averaged to estimate food intake on a daily basis. The place of preparation and the place of consumption of each food were recorded. The dietary assessment method used was described previously [15]. Food group intakes (in grams) were derived from the dietary recalls. The West African Food Composition Table [30] was used to categorize thirteen food groups: (1) Cereals and their products; (2) Starchy roots, tubers and their products; (3) Legumes and their products; (4) Nuts, seeds and their products; (5) Vegetables and their products; (6) Fruits and their products; (7) Meat, poultry and their products; (8) Fish and their products; (9) Eggs, milk and milk products; (10) Fat and oils; (11) Sweet foods (sweet beverages, candies, chocolate and lollipops); (12) Other (unsweetened) beverages (including water) and (13) Miscellaneous (like condiments). The original groups “Eggs and their products” and “milk and their products” were combined in a single group as their intakes were previously estimated low in school adolescents in Cotonou [15]. Plantain bananas and potatoes were included among “starchy roots, tubers and their products” because they are more starchy and more energy-dense than fruits and vegetables.
2.4. Data Analysis
- Food intake data were processed using a format designed in Microsoft Access (Microsoft Corporation, Redmond, WA, USA). Statistical analyses were performed with the Stata software package (version 10.0, Intercooled Stata; Stata Corp LP, College Station, TX, USA). Under-reporters and over-reporters were not excluded from data analysis since accuracy of basal metabolic rate (BMR) predictive equations in adolescents is uncertain [31,32]. Consumers were isolated as students with a positive difference in their fruit intake at school between follow-up and baseline. A paired samples t-test was used to compare consumers’ mean intakes of “fruits and their products”, “vegetables and their products” and sweet foods, as well as other dietary variables, between baseline and follow-up. In case of non-normality, the non-parametric Wilcoxon signed rank sum test was performed. To compare baseline values of anthropometric and food intake variables and change in dietary parameters between consumers and non-consumers, an independent samples t-test was used. For non-normally distributed data, the non-parametric Wilcoxon-Mann-Whitney test was performed. Pearson’s chi-square test was used to assess differences in proportions. All tests were two-sided and the significance level was set at 5%.
3. Results
3.1. Sample’s Characteristics at Baseline
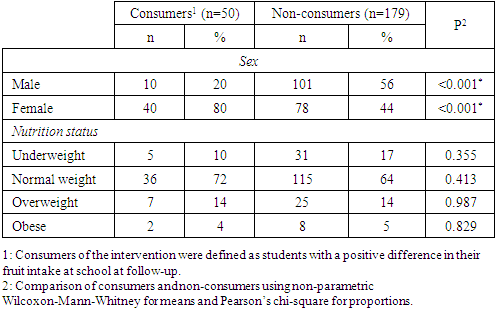
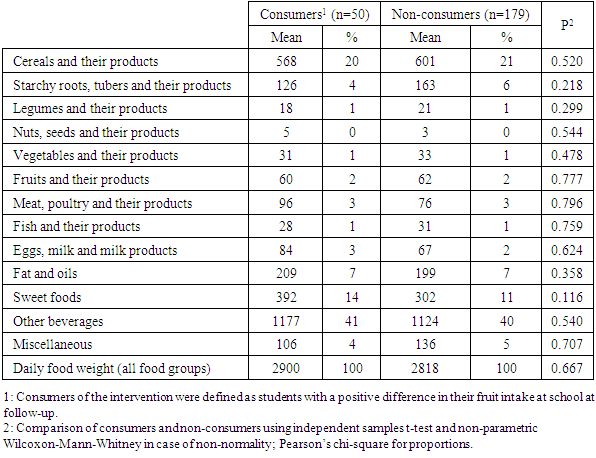
- Among the 249 survey participants, 14 were lost at follow-up and 6 outliers with improbable values for daily intakes of energy, fruits, vegetables or sweet foods were excluded. Among the remaining 229 participants, girls accounted for 51% (n=116). Subjects’ age ranged from 13.0 to 18.9 years with a mean of 17.0±1.3 years. Average BMI was 21.5±4.5 kg/m2. There were 13.9% overweight and 4.2% obese participants. Mean daily energy intake of the participants was 10335±3285 kJ at baseline. From this energy intake, 49% came from out-of-home prepared foods and 20% were consumed at school. Other (unsweetened) beverages (40% of the daily weight of food), cereals and their products (21%), sweet foods (11%) and fat and oils (7%) were more consumed by the participants. “Fruits and their products” and “vegetables and their products” represented respectively 2% and 1% of the daily weight of food consumed. Of the daily fruit intake, 10% were consumed at school. For daily intakes of vegetables and sweet foods, respectively 6% and 44% were consumed at school.Consumers represented 22% (n=50) of the 229 participants. They were older than non-consumers (p=0.028). Mean age of consumers was 17.5±1.0 years and non-consumers were on average 16.9±1.4 years old. Mean BMIs of consumers and non-consumers were the same and respectively 21.8±4.0 kg/m2 and 21.4±4.7 kg/m2 (p=0.382). Girls were more represented among consumers than among non-consumers (p<0.001). The 2 categories have similar nutrition status (Table 1).
|
|
|
3.2. Change in Consumers’ Fruit Intake over Time
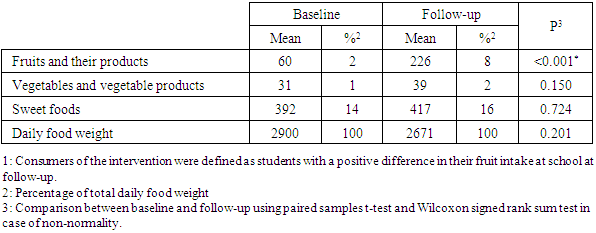
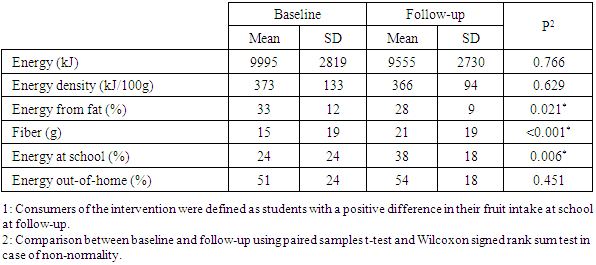
- Mean fruit intake of consumers increased by 166g/day (p<0.001) over the 2-month period (Table 4). This represented an increased from 2 to 8% of the food weight they consumed daily. Mean fruit consumption at school was 177g at follow-up compared to 2g at baseline (p<0.001), which corresponded to an increase from 3 to 78% of the daily fruit intake.
|
3.3. Change in Other Dietary Variables in Consumers
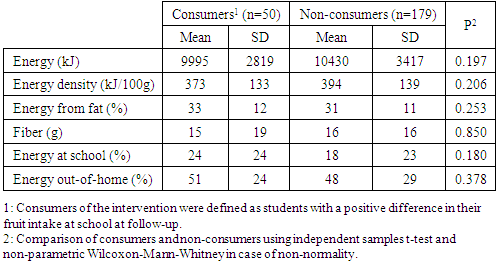
- Mean daily intakes of “vegetables and their products” and sweet foods did not change significantly in consumers over time (Table 4). The average daily energy intake from fat in consumers however, declined by 5% (p=0.021, Table 5). Mean fiber intake rose significantly (p<0.001), as well as mean energy contribution of food consumed at school, which increased from 24 to 38% daily (p=0.006).
|
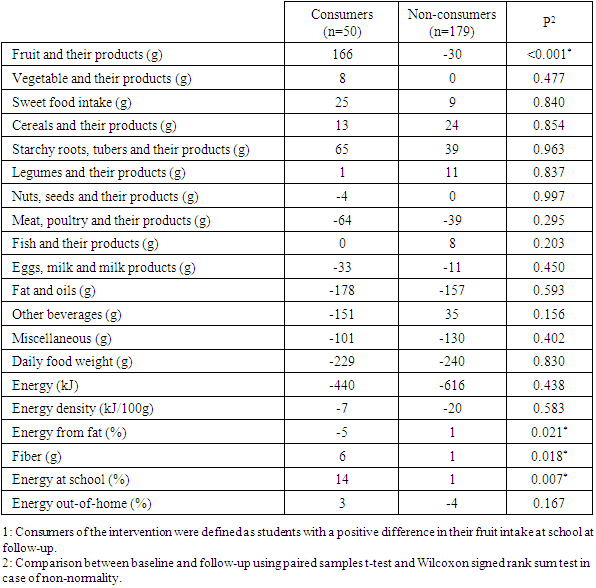
3.4. Change in the Diet of Consumers Compared to Non-consumers
- Except change in fruit intake, consumers and non-consumers were significantly different for change in daily energy contribution from fat, energy contribution of food consumed at school and fiber intake (Table 6). Percentage energy intake from fat decreased by 6% in consumers compared to non-consumers (p=0.021). Fiber intake and energy contribution of school food increased in consumers relatively to non-consumers.
|
4. Discussion
- The purpose of the present study was to test the ability of a single-component school-based fruit intervention, consisting in operating a fruit stall with a high hygiene standard, to increase adolescents’ daily fruit intake in urban Benin. The study also examined whether the intervention would affect the adolescents’ overall diet, particularly the intakes of vegetables and sweet foods. The adolescents’ fruit consumption was positively affected. Consumers, identified as students whose daily fruit intake at school increased, by 175g/day on average, consequently had mean daily fruit intake increase of 166g at the end of the intervention, probably as a result of higher availability and accessibility. The contribution of fruit consumption at school to consumers’ daily fruit intake rose from 3% only at baseline to 78%. Indeed, availability and accessibility were reported as major determinants of fruit consumption in adolescents at home as well as in school settings [24-26]. Several interventions conducted in high-income countries also rose adolescents’ fruit intake [17,18,33]. Specifically, programs targeting increased availability and accessibility of fruits at school were effective [23,34]. Although consumers represented only 22% of the sample, the substantial increase in their daily fruit consumption is an encouraging result, considering the short duration of the intervention and the fact that it was implemented in a period when fruits were expensive and less available. Indeed, the offer of food products on markets is generally low in Benin during the first term each year because it is in the middle of the dry season and this is a period when there is no agricultural production and harvested crops are ending [35]. A longer intervention period and a reduction in the selling prices of fruits in the school, concurrent to cheaper market prices, would probably have induced much greater fruit consumption by more students. It is likely that enhancing the food safety standard of the fruit stall was a good strategy to promote fruits in the target group, as was suggested previously [26].There was no change in consumers’ daily intakes of vegetables at follow-up. This is consistent with findings from other interventions which did not increase vegetable intake, although promoting consumption of both fruits and vegetables [34]. In Ghanaian students, when buying fruits, respondents were much influenced by availability followed by convenience and attractiveness [36] and Beninese adolescents were said to be reluctant to eat vegetables [26]. There was neither a change in consumers’ intake of sweet foods. It was expected that the intervention would induce a substitution of sweet foods with fruits. Likewise, the European School Fruit campaign reduced the consumption of junk food in participants less likely to be exposed to overweight and obesity, but was not effective at all for the more at risk ones [37]. However, other research showed how the promotion of fresh fruit and water reduced by 8 to 38% the proportion of children bringing sweet drinks at school and how this effect was sustained over 2 years after program implementation [38]. In our study, consumers and non-consumers had the same nutrition status at baseline, and this could have hided a potential effect on sweet food consumption.Consumers’ mean fiber intake increased significantly. In parallel, mean fat energy contribution in these participants declined, from 33 to 28%, a level in the normal range, 15-30% [1]. As fruits have a high fiber content and a low fat content [3], the observed changes in consumers’ fat and fiber intakes are probably a result of their greater fruit consumption. There was no change in the daily energy intake and energy density of consumers, despite their higher fruit and fiber intakes and a reduction in their fat intake. Fruits have high water and fiber contents and both components are known to lower dietary energy density and energy intake [3]. In another study promoting fruits and vegetables, subjects consumed more fruits and vegetables and their fat intake also decreased, from 33.6 to 30.6%, but their energy intake did not change [3,39]. It was suggested that replacement of higher-fat foods occurred. Changes in food group consumption between baseline and follow-up showed a 178g decrease in the intake of fat and oils, 21g more reduction than in non-consumers, although this difference was not significant.There is enough evidence that school-based fruit interventions are successful in adolescents [17,40] and their food consumption at school is important in urban Benin [15,41]. Considering the promising result of the present intervention after a short implementation period and although fruits were relatively costly, the promotion of fruits in urban Beninese adolescents via the school environment remains an interesting strategy. School-based fruit interventions with multiple components are suggested as the best option to increase adolescents’ fruit consumption. However, they are much more costly than single-component programs [17,18]. Among single component programs, free distribution of fruits yielded good results with sustained effect over years [19-21]. Free distribution of fruits had a similar positive effect on primary school children’s fruit intake in the Netherlands and showed a better potential for being adopted by teachers than a multicomponent intervention consisting of a classroom curriculum and parental involvement, without free fruits and vegetables [42,43]. However, free distribution of fruits requires having enough funds in the long term. As a LIC, Benin has limited resources to implement such a strategy. Moreover, although free distribution of fruits is an effective strategy [20,21,35,44] but is likely to establish an unintentional habit by exposing the adolescents to a frequently repeated behavior under the same conditions. On the other hand, a fruit stall would induce an intentional habit by making the students decide themselves to buy and consume fruits with full knowledge of the health benefits for them [18]. An intentionally acquired habit is likely to last longer. Moreover, sustainability of a free distribution would necessitate finding funds in the long term while a fruit stall is expected to be financially viable. In a low-income country, where the national budget is already deficient, the latter strategy would more easily find some interest from nutrition and health policy makers.The strategy tested in the present study, which was to sell fruits to students, had promising results and would more easily get approval from national policy makers than a free distribution. As such, this program deserves more attention. Its implementation at a larger scale and for a longer period would provide more elements to improve it. Attention should be given to the best way to embed it in the current national school feeding program although this program only target primary school students for the moment.The present study used an experimental design and was conducted in only one school selected by convenience. The intervention lasted only 2 months. However, the purpose of the study was to pilot-test the intervention at a small scale before further implementation. Moreover, this duration was long enough to detect changes in fruit intakes. Food intake, including fruit consumption, was estimated from 24-hour dietary recalls which are subject to memory bias. But, caution was taken to help subjects recall their food using physical aids (common household utensils of the study area) and prompting. This study is novel in the fact that the intervention tested is feasible, relevant and a context-appropriate way to promote fruit consumption in adolescents in urban Benin, as it was developed from a previous assessment of views and perceptions of the target population. Thus, this pilot intervention maximises conditions for a sustained effect.
5. Conclusions
- Operating a fruit stall following strict hygiene rules was able to increase fruit consumption in a sample of school-going adolescents in urban Benin. This intervention, if improved through a larger-scale implementation during a longer time period, would provide a good means to sustain regular and sufficient fruit consumption in school-going adolescents in urban Benin. In the context of Benin, a low-income country, lacking financial resources to implement national nutrition and health policies, this strategy is preferred over free distribution although the latter is already proven to be efficient and sustainable. A cost-effectiveness study is needed to compare the two strategies and provide additional evidence in favour of the fruit selling strategy.
ACKNOWLEDGEMENTS
- The authors thank all the school communities who participated in this study, especially the students.