-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Food and Public Health
p-ISSN: 2162-9412 e-ISSN: 2162-8440
2019; 9(3): 84-93
doi:10.5923/j.fph.20190903.02

Prevalence of Stunting, Overweight and Obesity among Egyptian Primary School Children in Behera Governorate
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNesrin K. Abd El-Fatah1, Mira M. Abu-Elenin2
1Assistant professor of Nutrition, Dept. of Nutrition, High Institute of Public Health, Alexandria University, Egypt
2Lecturer of Community Medicine, Dept. of Community Medicine, Faculty of Medicine, Tanta University, Egypt
Correspondence to: Mira M. Abu-Elenin, Lecturer of Community Medicine, Dept. of Community Medicine, Faculty of Medicine, Tanta University, Egypt.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Nutritional status is a primary determinant of a child’s health and well-being; Malnutrition negatively influences physical and mental development. This study aimed to assess the prevalence of stunting, overweight and obesity among primary school children in Behera Governorate, Egypt. A cross-sectional study was carried out on 2027 students. Anthropometric profile was assessed by calculating height for age, weight for age and BMI for age and gender Z scores. The prevalence of stunting and severely stunting growth were (11.3% and 1.15%). It was significantly associated with rural location, poorly educated mothers and birth order≥ 4. Thinness, overweight and obesity were (4.5%, 11% and 8.2%).
Keywords: School Children, Obesity, Stunting, Overweight, BMI for Age, Egypt
Cite this paper: Nesrin K. Abd El-Fatah, Mira M. Abu-Elenin, Prevalence of Stunting, Overweight and Obesity among Egyptian Primary School Children in Behera Governorate, Food and Public Health, Vol. 9 No. 3, 2019, pp. 84-93. doi: 10.5923/j.fph.20190903.02.
Article Outline
1. Introduction
- Children constitute a sizeable proportion of the population; their health and nutrition are of public health concern [1]. Nutritional status is a primary determinant of a child’s health and well-being, responsible for their physical and mental growth and development. Malnutrition manifests itself in the form of Stunting, Wasting, Underweight, Micronutrient deficiency or Overweight and Obesity (“double burden” of malnutrition) [2]. Stunting is a cumulative process of reduced growth that predominantly occurs before three years of age and persists into school age [3]. About 1% loss in adult height as a result of childhood stunting is associated with a 1.4% loss in productivity [4]. Stunting is associated with impaired mental development and poor school and academic performance, consequently become a public health burden. This association is because of complex environmental, social, and economic factors, besides nutrition unawareness [1]. According to the latest Egypt’s Demographic and Health Survey, 2014; stunting remains a significant public health concern in Egypt, affecting 1 in 5 children under 5 years of age, wasting and underweight for under five children stand at 8 and 6 percent, respectively. Wasting has increased significantly since 2000 [5]. According to the International Obesity Task Force, at least 155 million of the world’s children aged 5–17 are overweight of which; 35 - 40 million were obese. In the Eastern Mediterranean Region, data shows that 80% children aged between 13 and 15 years old are overweight or obese. Unhealthy dietary habits such as skipping breakfast, low milk, fruits and vegetables intake, high intake of soft drinks and sweets are the main causes coupled decrease physical activity. About 60% of obese children or adolescents are more likely to become overweight adults [6] with increasing the risk of development of metabolic syndrome, diabetes mellitus, cardiovascular and even fatty liver in later life [7]. In Egypt, 24.5 percent of children (5-14 years of age) classified as overweight by the (EDHS 2014) [5], while obesity among school age children constitutes an emerging concern (9.8%); the Egyptian Medical Association for the Study of Obesity in early 2010 estimates that 15 percent of Egyptian (school-age) children are obese, in comparison with its 1990’s estimate of only six percent. Different studies had been conducted in different Egyptian cities. In 2017 two studies were conducted in Assiut and Sohag cities [8,9], overweight and obesity prevalence was 11.24%, 16.5% and 12.28, 14.6% respectively. Overweight and obesity among children from 6-12 years; was 23.7% and 19.5% respectively in Menoufia governorate during 2015 [10]. In 2014, A large study was conducted on 3500 Alexandria primary school children, 9% of them were overweight compared to 16.8% were obese. [11]. Finally, in 2011 a study carried out in Port Said city, 17.7% were overweight and 13.5% were obese respectively [12]. Since no studies have been conducted in Behera governorate, the aim of the present study is to evaluate the prevalence of stunting, overweight and obesity among primary school children in Behera Governorate, Egypt.
2. Subjects and Methods
2.1. Study Design and Sampling
- A cross-sectional study was conducted during the period from January to April 2017 in Behera governorate primary schools, Egypt. Behera governorate have 19 Educational Administrations with 734592 primary schools’ students. Sample size was calculated using EPI-INFO 2002 software, and due to the unavailability of data regarding nutritional status of school children in Behera governorate, we assume that 50% of children were overweight and obese with a precision of 3%, confidence level of 99% and an error of 0.01; a minimum sample of 1840 students was required. The sample size was increased to 2027 for proper representation of different age groups.A multistage stratified random sampling technique was used; stratification was based on Behera Educational Administrations, grade level and sex. In the first stage, two Educational Administrations were chosen randomly from Behera Governorate (Bandar Kafr El Dawar (51 mixed primary schools) and Hosh Issa (67 mixed primary schools). From each administration two mixed primary schools were randomly selected after exclusion of the one-gender schools. The predetermined sample was proportionally allocated on the selected schools. In the subsequent stages, the allocated sample for each school was equally allocated on all grades (students selected by simple random sample from two classes /each grade from first to fifth grades). The study was approved by The Ethics Research Committee of High Institute of Public Health at Alexandria University. All students and their parents were informed about the purpose of the study and a consent to participate in the study was obtained. Privacy and confidentiality were assured.
2.2. Data Collection
2.2.1. Demographic and Socioeconomic Data
- Sampled students or their parents filled out a self-reported pre-designed questionnaire to collect demographic and socioeconomic data including age, gender, and grade level of students. Also, residence, educational level and occupation of parents, family size, number of house rooms, and income/month data were collected to calculate the socio-economic score.
2.2.2. Anthropometric Measurements
- Body weight (in kilograms) and height (in meters) of each student were measured according to criteria described by Gibson (2005) [13]. Height for age (HA), weight for age (WA) and BMI for age (BMA) and gender Z scores were calculated by anthroplus software and were compared to an international reference population, the WHO Growth Reference for School-Aged Children and Adolescents [14]. HA measures are below minus two standard deviations (-2 SD) from the median of the reference population are considered stunted. Children who are below -3 SD are considered severely stunted. Children whose WA measures are below -2 SD are underweight for their age, while those whose measures are below -3 SD are severely underweight. Finally, Children whose BMI > +2 SD above the WHO growth standard median are considered obese. Overweight BMI > +1 SD and thinness: BMI < -2 SD. Sever thinness: BMI <-3 standard deviations below the WHO growth standard median.
2.2.3. Eating Habits
- The frequency of following habits were assessed; number of main meals per day, breakfast consumption, intake of snacks, fast food consumption, and eating food at schools.
2.3. Statistical Analysis
- Data analysis was performed using the Statistical Package for Social Sciences (SPSS, version 16; SPSS Inc., Chicago, USA). Descriptive statistics in the form of number and percentage were used to represent qualitative data. Chi square test was used to detect significant difference between groups. When Chi square test was not appropriate, Monte Carlo Excat Test (MCET) was used instead. For all statistical analyses, p-values ≤ 0.05 were considered significant.
3. Results
- This study involved 2027 primary school children, from grade 1 (19.9%), grade 2(18.1%), grade 3 (21.5%), grade 4 (21%) and grade 5 (19.5%). Their mean age was 8.6± 1.5 years ranged between 5.8 to 14.4 years. Boys were (50.5%) and girls were (49.5%). Children recruited from rural schools represent 22.1% and 77.9% were from urban ones. Regarding the socioeconomic status, the majority were considered to be of low level (80.8%, 17.8%) were at moderate level and only (1.4%) of high level. We found that (8.2%) of the students were obese, (11.1%) were overweight and (3.94% & 0.59%) were thin & severely thin respectively.The prevalence rate of obesity and overweight were least at 7-8 years (grade 2) (9.3%, 4.4% respectively) and significantly increased with age to be the highest at the age of 9-10 years (grade 4) (P=0.003). Higher rates were found between girls (12.5%, 8.8% respectively) than boys (9.8%, 7.5% respectively) and the children of urban back ground (12.5%, 9.5%) than rural ones (5.4%, 3.4%) (p <0.0001). Rate of overweight and obesity was significantly observed between children whose mothers had low to middle level of education, and of high to moderate socioeconomic level, while thinness rates was higher among children from low educated mothers and low socioeconomic level, as shown in Figure 1 & Table 1.
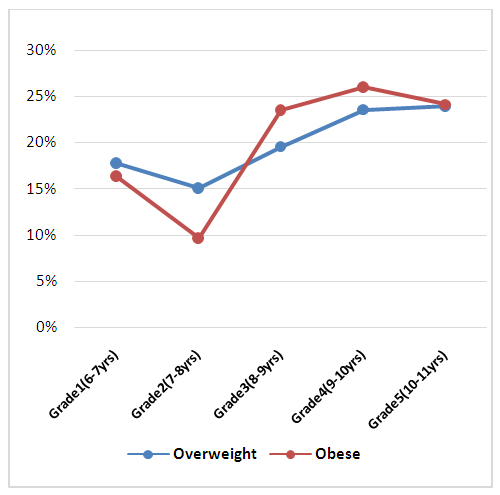 | Figure 1. Frequency distribution of overweight and obesity among different primary school children grades |
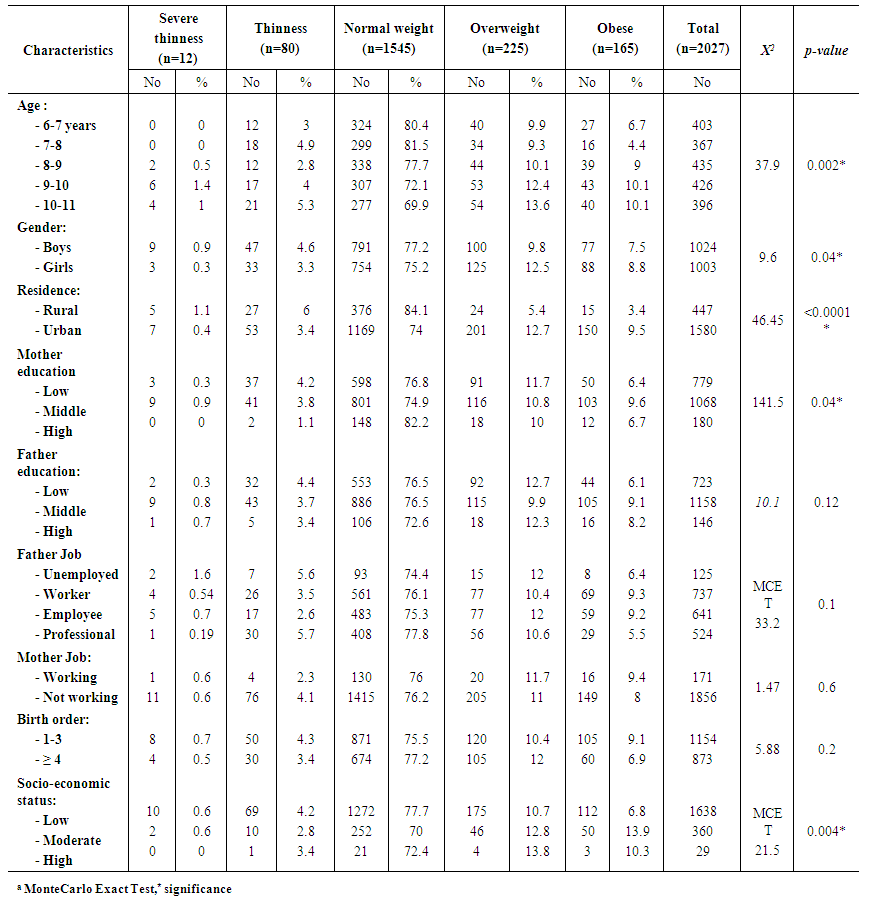 | Table 1. BMI for Age Z-Score of the Studied Primary School Children in Relation to Sociodemographic Characteristics |
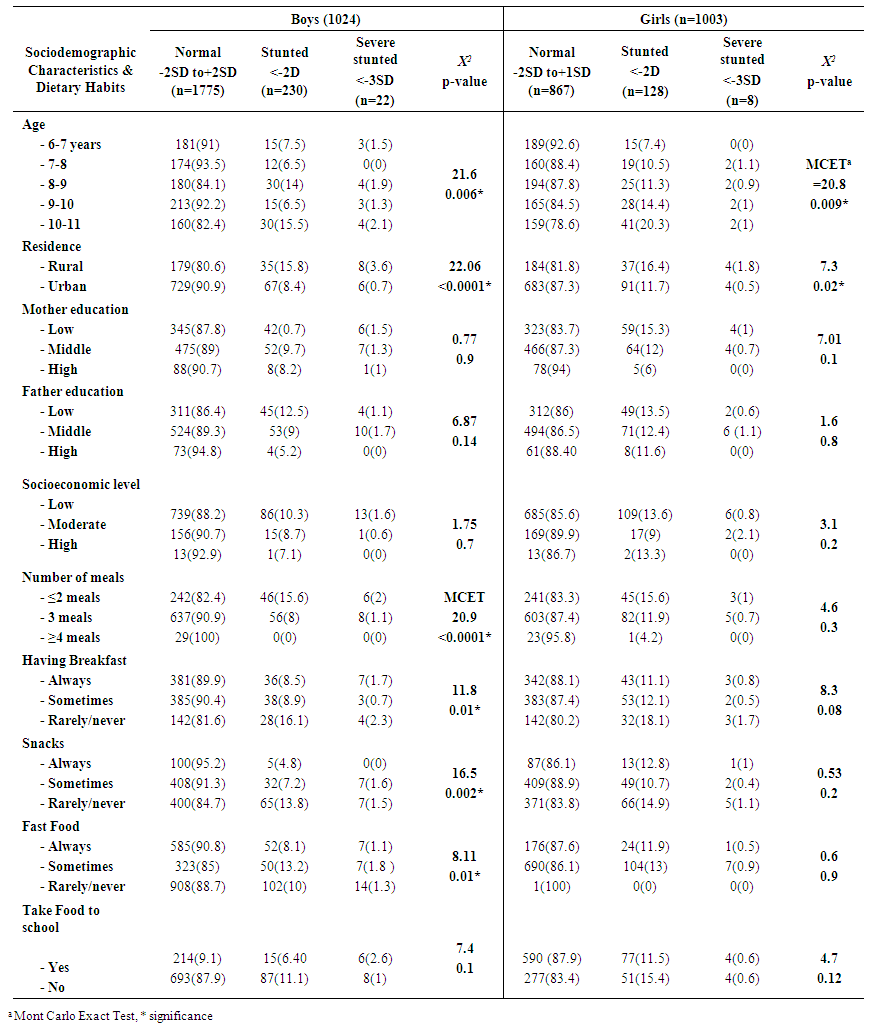
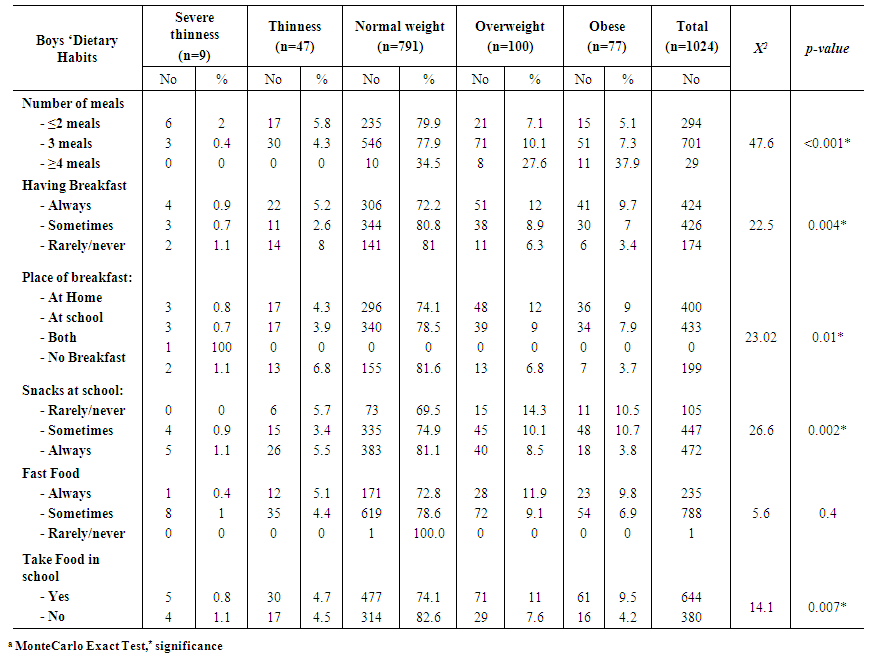 | Table 2a. Dietary Habits Associated with BMI for Age Z-Score among the Studied Primary School Boys |
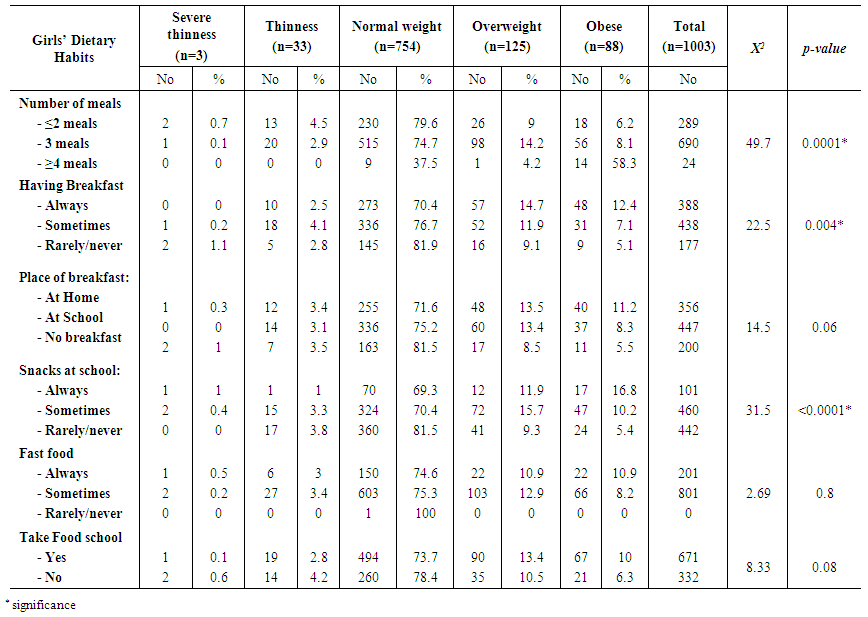 | Table 2b. Dietary Habits Associated with BMI for Age Z-Score among the Studied Primary School Girls |
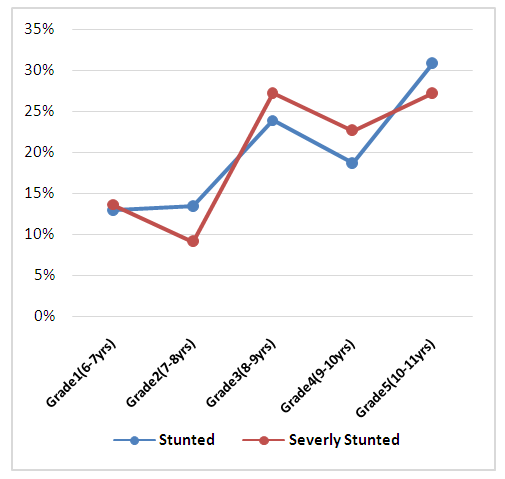 | Figure 2. Frequency distribution of stunting and severe stunting among different primary school children grades |
4. Discussion
- Childhood has emerged as a critical period for malnutrition, stunting as an indicator of chronic malnutrition or excessive weight gain in early years of life may lead to poor physical and mental development, obesity and chronic disease in later years [15]. Stunting of a child’s growth may be the result of a failure to receive adequate nutrition over a long period of time or of the effects of recurrent or chronic illness. Chronic undernutrition, as evidenced by the proportion of stunted children, was of mild prevalence in this school-aged study, the prevalence of stunting and severely stunting growth was 11.3%, 1.15% respectively. The overall prevalence of stunting in our study was high compared to other countries such as Russia (3.3%) [16] or in Brazil (9.1%) [17]. Some other studies reported higher rates of stunting, 18.7% in Iraq [18], 40.3% in Nigeria [3] and 37.9% in Ethiopia [19], since these countries experience constraints on economic, environmental and social development that affect the physical growth of children before puberty. It is believed that stunting is mainly a problem of young children, recent studies suggest that children will not catch up growth during middle childhood if they remain in the deprived environment that caused them to become stunted in the first place. Thus, children who have become stunted are likely to remain stunted into adolescence [20].It was noted that the prevalence of stunting increased significantly with age in a (for boys χ2 = 21.6, P 0.006 ; and for girls MCET = 20.8, P=0.009). The peak rate for stunting and severe stunting for both genders was at the age of 10-11 years [ (15.5%, 1% for boys), (20.3%, 1% for girls)]. This age pattern was also reported in studies demonstrating an increasing prevalence of stunting with age [18,21]. It could be explained that older children may be more stunted than younger ones because they were more malnourished as young children, not because they are growing poorly as schoolchildren.Regardless that there was no gender difference statistically, in this study girls were more likely to be stunted than boys, indicating that growth in girls may be more sensitive to socioeconomic factors and to age specific differences in catch-up growth. This may be supported by gender inequity in food intake. Similar findings are reported in other studies [18,21,22]. Factors associated with stunting among school-age children in our study were respondents’ age, rural location, poorly educated mothers and unemployed fathers, these findings mirror what is documented in literature and emphasizes the importance of educational status on stunting, in line with other related studies [3,23,24]. Higher prevalence of intestinal parasitic infestations in rural areas was reported in a previous study [25]. Our study buttresses existing literature which indicates a positive association between birth order over 4 and child malnutrition [3,24]. Less frequent meals per day and skipping breakfast were significant determinants for stunting, these observations in line with several studies among conducted among school children irrespective to gender stratification [3,17,19].In the present study, the overall prevalence of overweight and obesity among children aging from 6 to12 years (11%, 8.2%) were lesser than the reported results of a national Egyptian Demographic Health Survey [5]. However, rate of thinness was (4.53%) higher than the national level 2.5% [5]. Other regional studies in Dubai, Kuwait and Jordan showed higher figures for overweight and obesity [26-28], while lower rates were reported in UK, those variations related to cultural and dietary habits differences [29]. In Assiut, Sohag and Port Said cities [8,9,12], overweight prevalence was in agreement with our results. But higher rates of overweight and obesity was detected among 6-12 years children in Menoufia governorate during 2015 (23.7% and 19.5% respectively) It could be attributed to the reduced activity level observed by the researchers [10]. Among 3500 Alexandria primary school children, lower (9%) prevalence of overweight but higher obesity rates were recorded compared to our findings as this study sampled students from private schools too [11].
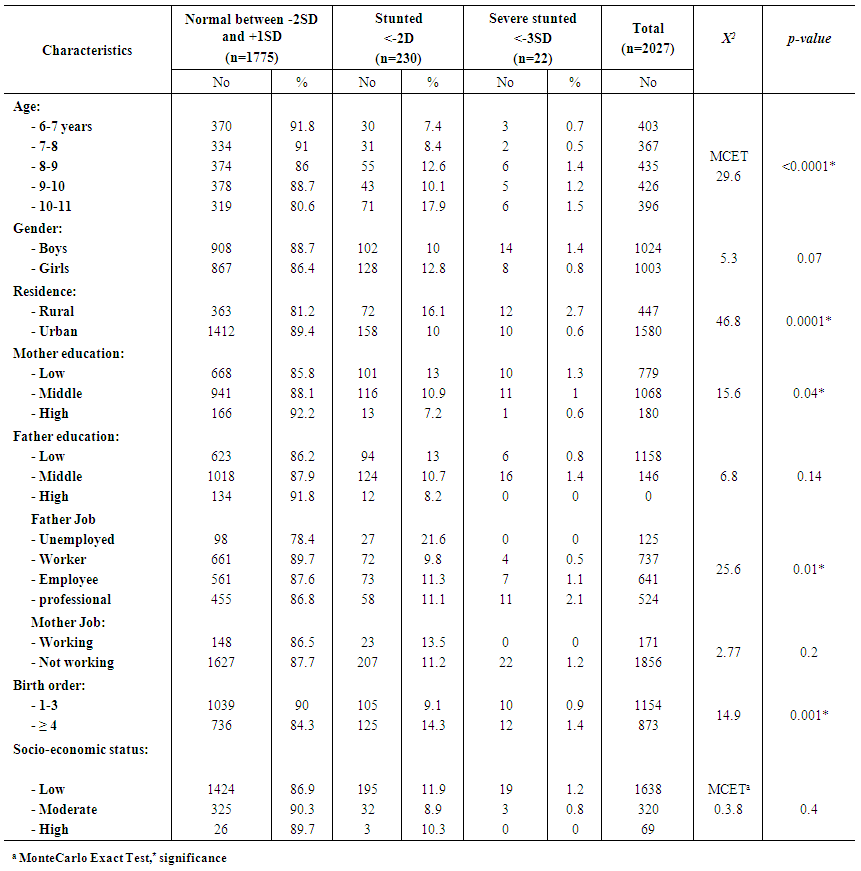 | Table 3. Height for Age Z-Score of The Studied Primary School Children in Relation to Sociodemographic Characteristics |
 | Table 4. Factors Associated with Height for Age Z-Score Percentage among the Studied Primary School Children |
5. Conclusions
- The prevalence of malnutrition disorder among Egyptian primary school children is considerable These conditions are associated with the sociodemographic characteristics of children and parents, as well as the eating habits of children. Parental characteristics and eating habits should be considered when planning feasible and effective nutrition programs for primary school children.
List of Abbreviation
- - Height for age (HA)- Weight for age (WA) - Body mass index for age (BMA)- Body mass index (BMI)- Monte Carlo Exact Test (MCET)
Declaration
- Reviewing the research proposal and approval was conducted before starting by the Ethics Committee of High Institute of Public Health Alexandria University. Administrative approvals were completed from the Ministry of Education and school management as required. The study objectives were explained to students in the class before assessment of their nutritional status and filling the questionnaire. Informed written consent was obtained from caregivers who welcomed to participate in the study and confidentiality was assured.
ACKNOWLEDGEMENTS
- The authors would like to thank the Ministry of Education and selected schools’ managers in Bahera Governorate for their collaboration during conducting this research. Our gratitude also goes to the study subjects for their willingness to participate in the study.