-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Food and Public Health
p-ISSN: 2162-9412 e-ISSN: 2162-8440
2019; 9(3): 79-83
doi:10.5923/j.fph.20190903.01

Green Tea Consumption Does Not Adversely Affect Kidney Function and Haematological Parameters
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKenneth Essex1, Amged Mehdi2, Sapha Shibeeb1, 3
1School of Medical Science, Griffith University, Gold Cost Campus, Queensland, Australia
2Faculty of Physical Education and Sport Science, Karbala University, Iraq
3Endeavour College of Natural Health, Melbourne Campus, Victoria, Australia
Correspondence to: Sapha Shibeeb, School of Medical Science, Griffith University, Gold Cost Campus, Queensland, Australia.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

It is well established that green tea consumption is associated with many health benefits. These benefits include anti-thrombotic, anti-oxidant, anti-atherogenic and anti-obesity effects. However, there are limited studies have investigated the direct effect of green tea consumption on renal function and haematological parameters. Therefore, the aim of this study was to assess the effect of green tea consumption on kidney function, red cell count, haemoglobin, white cell and platelet counts in healthy human subject. Ten healthy human volunteers (5 females and 5 males) consumed three cups/day (200 mls per cup) of green tea for a period of four weeks. Kidney function and haematological parameters were analysed at the end of weeks 1, 2 and 4. Our data indicated that green tea consumption does not adversely alter renal function as assessed by serum creatinine concentration, serum urea concentration and glomerular filtration rate. Furthermore, full blood count parameters remained within the normal reference interval and numbers remained unaffected. This study demonstrated that green tea consumption is not associated with adverse effects on kidney function and haematological parameters.
Keywords: Green tea, Kidney, eGFR, Creatinine, Urea
Cite this paper: Kenneth Essex, Amged Mehdi, Sapha Shibeeb, Green Tea Consumption Does Not Adversely Affect Kidney Function and Haematological Parameters, Food and Public Health, Vol. 9 No. 3, 2019, pp. 79-83. doi: 10.5923/j.fph.20190903.01.
Article Outline
1. Introduction
- Tea is one of most commonly consumed beverages worldwide [1]. Tea is extracted from the leaves of the Camellia sinensis plant and is processed to give a variety of different flavours and qualities [2]. Green tea is a raw, dried and unprocessed (non-oxidised) leaf that retains all of the natural chemical polyphenols, which otherwise would be oxidised and reduced during the processing of the leaves into oolong (partially oxidised) or black tea (oxidised) [1,3]. Green tea is composed mostly of the low molecular weight polyphenol flavonoids, specifically catechins. The catechins found within green tea are epicatechin (EC), epicatechin-3-gallate (ECG), epigallocatechin (EGC), and epigallocatechin-3-gallate (EGCG) being the major catechin, accounting for 48-55% [4].Several in vitro, clinical trials and animal studies have demonstrated strong evidence that green tea and its polyphenols may play an important role in reducing the risk of developing several chronic diseases, particularly cardiovascular disease, obesity and cancer [5]. Indeed, green tea has been shown to exert many biological activities that include anti-oxidative, anti-inflammatory and anti-thrombotic effects [6,7]. We have demonstrated that EGCG inhibited platelet aggregation in a concentration dependant manner [8].In a study by Mohamadin et al. (2005) investigating the renoprotective effect of green tea extract following Cyclosporine A (CsA) induced nephrotoxicity, it was found that administration of green tea extract was associated with renoprotective effects [9]. Other studies have shown beneficial effects on kidney function including reduction in diabetes-induced hypertrophy and nephropathy of kidneys [10,11] and protection against nephrotoxicity [12]. While, some studies have reported high-dose green tea extract were associated with increased creatinine levels, disrupted kidney function and hepatotoxicity [13,14]. However, the majority of reported effects were observed in animal studies and little or no evidence demonstrating the effect of green tea consumption of human kidney function.Although green tea consumption has been shown to exert beneficial effects and is generally safe and well tolerated, there are few case reports that suggested some green tea constituents particularly EGCG may produce hepatotoxic effects in humans [15]. However, these adverse hepatotoxic effects have been attributed to predisposing conditions that subjects may have [15,16]. Furthermore, these adverse effects have not been demonstrated in controlled studies [16].The general safety of green tea and its catechins have been demonstrated by both human and animal studies [17]. However, there is little evidence to demonstrate the effect of green tea on human kidney function and blood cell counts. Therefore, the aim of the study is to investigate the effect of green tea consumption on kidney function and blood cell generation in healthy humans.
2. Materials and Methods
2.1. Human Participants
- The green tea (Lipton®) used in this study was chosen specifically due to its accessibility and availability to the public. Flavonoid concentration was reported to be between 100 and 200 mg of flavonoids per tea bag as per the manufacturer’s estimation.
2.2. Green Tea
- The green tea (Lipton®) used in this study was chosen specifically due to its accessibility and availability to the public. Flavonoid concentration was reported to be between 100 and 200 mg of flavonoids per tea bag as per the manufacturer’s estimation.
2.3. Green Tea Consumption
- Each volunteer consumed three cups/day (200 mls per cup) of green tea for a period of four weeks. One week prior to the initial blood collection, participants were advised to minimise foods containing antioxidants. This was to minimise the inference of other antioxidants from other food sources.
2.4. Sample Collection and Preparation
- At the beginning of week 1 participants’ blood was collected to establish a baseline level. At the end of week 1, week 2 and week 4, blood samples were collected. Venous blood drawn was collected into serum separating tube (SST) and Ethylenediaminetetraacetic acid (EDTA) tube using butterfly needles (BD vacutainers®). SSTs were allowed appropriate time to clot and were immediately centrifuged at room temperature for 10 minutes at 2000 x g. Serum was then aliquoted into Eppendorf tubes and stored at -80°C and later analysed. EDTA tubes were analysed immediately post collection for haematological parameters.
2.5. Kidney Function Tests
- Serum urea and creatinine were analysed on a fully-automated ARCHITECT ci8200 (Abbott Diagnostic, Lake Forest, IL, USA), using spectrophotometry, following the ARCHITECT ci8200 operator’s manual. The estimated Glomerular Filtration Rate (eGFR) was calculated using the subject’s age, sex and serum creatinine result according to the CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) formula [18]. Estimated GFR is considered one of the useful methods to assess kidney function [19].
2.6. Full Blood Counts
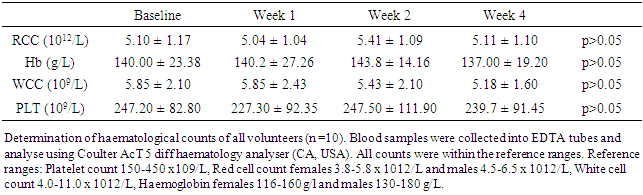
- Full blood counts consisting of red blood cells (RBC), white blood cells (WBC), platelet (PLT) count and haemoglobin (Hb) were analysed using whole blood from collected EDTA containing blood collection tubes by a Coulter Act 5 Diff Haematology Analyser (Beckman Coulter Inc, Brea, California, USA).
2.7. Statistical Analysis
- Results are presented as mean and standard deviation (±SD) and analysed using GraphPad Prism software version 6.01. Statistical analysis was analysed using one-way ANOVA while utilising Dunnett’s as a post hoc test. A p<0.05 was considered statistically significant.
3. Results
- Ten healthy subjects completed the 4 week trial. Mean age ± standard deviation (SD) for the sample was 28.50 ± 7.25 years Full blood count was measured at baseline and at weeks 1, 2 and 4 of the trial to assess the effect of green tea consumption of haematological parameters. There was no significant change in the values of red blood cells (RBC), haemoglobin (Hb), white blood cells (WBC) and platelets (PLT), table 1.
|
3.1. Kidney Function Tests
- Serum creatinine and urea were directly measured to assess the renal function in response to green tea consumption. Serum creatinine and urea concentrations did not significantly change from baseline over the 4 week period (p> 0.05 vs baseline, Figures 1 & 2, respectively). Baseline (week 0) serum creatinine was 74.66 ± 6.77 mmol/L, and week 4 concentration was 73.87 ± 6.13 mmol/L, p>0.05. Similarly, baseline serum urea concentration was 4.70± 0.68 µmol/L, while, week 4 concentration was 4.80 ± 1.06 µmol/L, p>0.05.
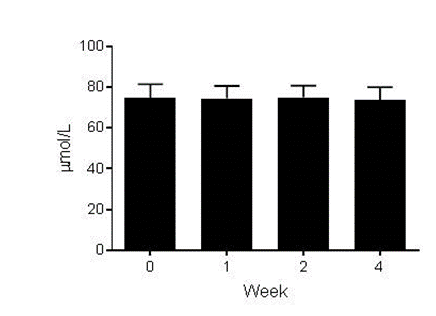 | Figure 1. Effect of green tea consumption on serum creatinine concentration (n=10). Serum creatinine concentration was tested at baseline (week 0) and at the end of weeks 1, 2 and 4. Green tea consumption did not significantly alter creatinine concentration. One-way ANOVA with Dunnett’s post-test. p>0.05 vs.Basline. Mean ± SD |
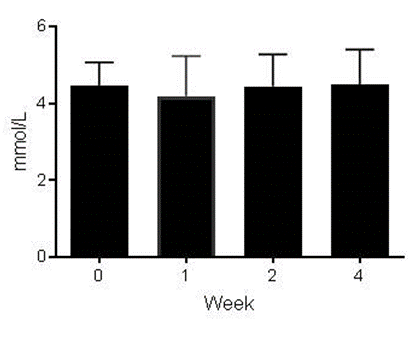 | Figure 2. Effect of green tea consumption on serum urea concentration (n=10). Serum creatinine concentration was tested at baseline (week 0) and at the end of weeks 1, 2 and 4. Green tea consumption did not significantly change urea concentration. One-way ANOVA with Dunnett’s post-test. p>0.05 vs.Basline. Mean ± SD |
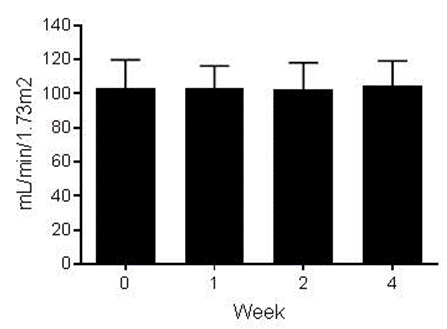 | Figure 3. Green tea consumption for 4 weeks did not significantly alter eGFR (n=10). One-way ANOVA with Dunnett’s post-test. p>0.05 vs.Basline. Mean ± SD |
4. Discussion
- In this study we have demonstrated that continuous 4 week green tea consumption does not adversely alter kidney function in healthy human subjects. To our knowledge this is one of the few studies that have directly investigated the effect of drinking 600 ml/day of green tea on kidney function. Furthermore, our data demonstrate that chronic green tea consumption does not negatively impact full blood count parameters. Green tea and its polyphenolic constituents have been shown to induce multiple beneficial effects [20]. Indeed, a number of studies have investigated the effect of EGCG the major component of green tea on kidney function using animal models of nephrotoxicity [21,22], aging [23] and diabetes induced renal damage [24,25]. Some concerns have been raised regarding reported hepatotoxicity in some subjects. However, several studies have demonstrated that hepatotoxicity is mild and rare and is only associated with high EGCG intake [16]. On the other hand, the direct effect of green tea consumption on healthy human kidney function is not well investigated.The kidneys are an essential organ to human health. The kidneys filter toxic metabolic waste production from circulation [26]. Several tests are available to assess renal function. Measurement of serum creatinine levels provides an indication of renal function. Elevated serum levels suggest impaired renal filtration. Following 4 week green tea consumption the levels of serum creatinine levels did not significantly change, suggesting renal filtration was unaffected. Measurement of serum urea levels is another is another test to assess kidney function [27]. Urea is the main nitrogenous waste product of protein metabolism and is excreted via the kidneys [28]. Drinking green tea for 28 days did not significantly alter serum urea concentration when compared to the baseline.Glomerular filtration rate is widely used in clinical settings as a direct measure of renal function. It is regarded as one of the best methods to assess the overall renal function [19]. When determining eGFR the patient’s age, sex, and body size as well as their serum creatinine levels are taken in account. Decrease in eGFR suggests a decline in overall kidney function [28]. Green tea consumption did not reduce eGFR, suggesting overall kidney function was not affected.Finally, full blood examination was performed to assess the effect of green tea consumption of red cells and red cell parameters, white cells and platelets. There was no significant difference in full blood count parameters post green tea consumption. These data suggest that green tea consumption does not alter blood cells and their capacity to carry out their function. Furthermore, these data also suggest that the bone marrow function is not affected and blood cell production is not altered.
5. Conclusions
- This study demonstrates that drinking 600 ml/day of green tea does not adversely alter kidney function. Kidney function was assessed by serum creatinine, eGFR and serum urea. To our knowledge this one of the few studies that directly investigated the effect of green tea consumption on renal function and parameters of full blood count in healthy humans. However, further studies are warranted to investigate green tea benefits in patients with renal disease.