-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Food and Public Health
p-ISSN: 2162-9412 e-ISSN: 2162-8440
2016; 6(5): 123-129
doi:10.5923/j.fph.20160605.03

Household and Food Sensitive Critical Correlates as Predictors of Child Nutritional Status
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLDavid Omondi Okeyo1, Peter Kirabira2
1School of Public Health, Department of Nutrition and Health, Maseno University, Maseno Township, Kenya
2Institute of Public Health and Management, International Health Sciences University, Kampala, Uganda
Correspondence to: David Omondi Okeyo, School of Public Health, Department of Nutrition and Health, Maseno University, Maseno Township, Kenya.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Malnutrition has both short and long term effects and may lead to increased mortality among children under five years. It may also lead to impaired development, poor educational achievement and poor economic productivity if not addressed at an early stage of child growth and development. Rapid growth of urban informal settlement is being experienced in Kisumu city in Kenya and this slum is characterized by overcrowding, filth, inadequate water supply, poor drainage and poverty. These characteristics have negative impact on general health and may compromise nutritional status of children within this setting in addition to staggering economic development. This menace could be attributed to household factors such as food security measures, food consumption frequency and diet pattern, parasitic infection, family size and family diversity. The study attempted to explore the competitiveness of household factor correlates as key predictors of nutritional status. The study targeted a sample of 400 households made up of caregivers with children aged between 6-59 months as sampling units. The study employed use of structured questionnaire with key variables under focus explicitly covered and anthropometric assessments techniques. Statistical analysis explored use of risk estimated odds ratios in multivariate logistic regression. The results revealed that parasitic infections, family size and diet diversity score had significant influence on both Height-for-Age z-score (HAZ) and Weight-for-height z-score (WHZ) (p<0.05) based on odds ratio estimations. Weight-for-age z-score (WAZ) did not show linkage with household factors except for parasitic infection which was inversely associated with underweight in a similar pattern as wasting (p<0.05). In conclusion, it appears that when all the three blocks of factors are put together and considered interactively HAZ is hierarchically predicted by food security, intestinal parasitic infection, family size, diet diversity score and health seeking behavior in that order.
Keywords: Household factors, Correlates, Child nutritional status, Slum
Cite this paper: David Omondi Okeyo, Peter Kirabira, Household and Food Sensitive Critical Correlates as Predictors of Child Nutritional Status, Food and Public Health, Vol. 6 No. 5, 2016, pp. 123-129. doi: 10.5923/j.fph.20160605.03.
Article Outline
1. Introduction
- Malnutrition within urban informal settlements continues to rise higher that the rural setting rates. In order to target reduction of malnutrition within urban informal settlement household factors are core in the epicenter of intervention models. Key measures of households in this context included food security measures, food consumption frequency and diet pattern, parasitic infection, family size and family diversity. Food insecurity may have greater influence on nutritional status. Some authors have attempted to establish the linkage between food insecurity and nutritional status of children at household level. A study conducted in Nepal revealed a strong linkage between food security and malnutrition among children with a focus given to WAZ and HAZ (Singh et al., 2014). A similar linkage was also found in rural Ethiopia (Hadley et al., 2012) and Malaysia (Ali et al., 2014). However, the two studies had more focus on the strong relationship between food insecurity and WAZ. Critical analysis of these studies reveals an outcome that is inclined towards WAZ. This implies that much of the relationships that exist between food insecurity and nutritional status show limited influence on WHZ and HAZ, but more frequent on WAZ. This therefore shows that further research was needed in different settings to explain this relationship further.Diet diversity is a measure of quality of diet and a proxy outcome of food security at household level. Diet diversity which is depicted by varied food groups may have a strong linkage with nutritional status of children at household level. Some studies which have been conducted among rural households have revealed strong relationships between diet diversity and nutritional status. Diet diversity had a strong association with HAZ across eleven (11) demographic and health surveys (Arimond and Ruel, 2004). Other studies with similar outcome revealed strong linkage with both HAZ and WAZ within urban setting with slightly lower risk in rural setting (Hatløyet al., 2000) suggesting that diet diversity and variety could be a major issue in urban setting and hence within informal settlements than in rural setting. High diet diversity was associated with reduced odds of HAZ (Rah et al., 2010), Implying a possible influence. Most household infections target parasitic helminthes infections. These infections are common within informal settlements in Sub-Saharan Africa due to poor sanitary conditions and lack of personal hygiene among households. Many studies have revealed strong linkage between helminthes infection and stunted growth among children (Shang et al., 2010; Moock and Leslie, 1986) and some of these high prevalence of HAZ associated with helminthes were common in urban schools (Amuta and Houmsou, 2009) depicting high risk within urban informal settlement. A study conducted by Luanga et al., (2012) showed that increased incidence of HAZ and WAZ could be attributed to the potential effect on intestinal infections, common at household level with poor hygiene measures put in place. Strong evidence attempts to relate gastrointestinal parasitic infections such as ascaris lumbricoides, hookworm and trichuris trichiara with low household income, poor handling of personal and environmental sanitation, overcrowding and limited access to clean water (Mengistu et al., 2007). These conditions are typical characteristics of urban informal settlement and could be real for Obunga slum in Kisumu. Poor nutritional status was associated with parasitic infections (Nam et al., 2012) in Ethiopia and this kind of relationship would warrant further investigations in other unique settings and more specific in urban informal settlement that has become a public health concern. Family size refers to the number of people living in a household to constitute a family. Larger family size may interfere with food distribution especially among poor households where resources are limited. Large family sizes have been found to be associated with protein-energy malnutrition [PEM] (Ehtishman et al., 2011). This background confirmed that many of the studies seemed to dwell on general rural population with few urban oriented investigations. This indicates limited focus on unique settings of Public Health concern like urban informal settlements. The general research effort ignores competition of these factors as predictors of nutritional status with an integrated predictor model block. These are major gaps that this study intends to close.
2. Materials and Methods
2.1. Study Setting Description
- This study concentrated in Kisumu East where under five mortality rate (220/1000) has consistently exceeded the national rates between 2008 and 2014 (52/1000) with minimal decline experienced at the moment (Central Beureu of Statistics et al. 2014). Malnutrition remains one of the leading causes of child mortality in poor resource settings. A few studies that have explored the causes of malnutrition in urban setting in Kenya concentrated more on the capital city influence where Nairobi has been on focus, ignoring fast growing cities like Kisumu. Kisumu is currently experiencing high rate of expansion of urban informal settlement including Nyalenda, Bandani, Manayatta, Nyawita and Obunga.
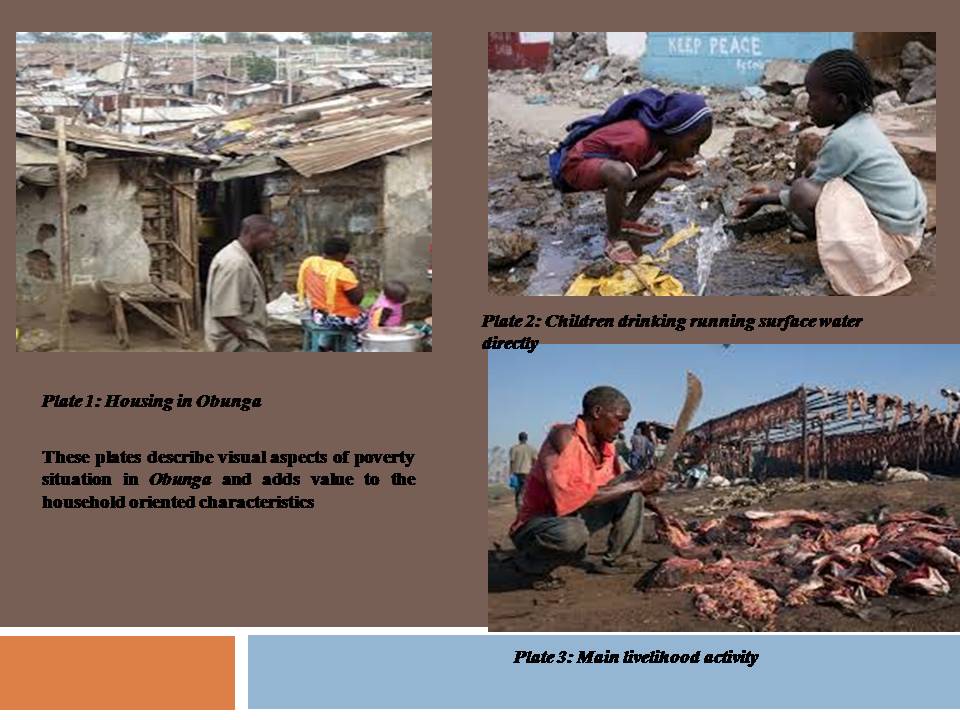 | Figure 1. Visual setting description |
2.2. Research Process and Methods
- The study targeted a population of 4000 eligible households from which a scientifically determined representative sample size was determined to arrive at 400 eligible households. An eligible household had a child between 6-69 months whose mothers consented to participate. Fishers et al formula (Mugenda and Mugenda, 2009; Omondi 2016) was used to determine the sample size. Selection of individual participants was based on systematic randomly sampling techniques. The study employed use of structured questionnaire which had household variables and additional anthropometric form for weight, height and age records. The latter were conducted using standards calibrated instruments and acceptable clinical procedure. Household factors included measures such as food insecurity, diet diversity, intestinal infections and family size. The final tool was pre-tested for reliability and validity. Reliability test applied participating pretest methods where the respondents were informed that the pretest is a practice run. They were asked to explain reactions to question form, wording and order. This kind of pretest was useful to determine whether the questionnaire was understandable. The second pretest method was an undeclared pretest, where the respondents were not informed that the exercise was a pretest. The survey was given just the same way as it would happen for the real survey. This type of pretest was useful in checking choice of analysis and the standardization of the survey. Validity focused on content approach from expert review mechanisms. Data was analyzed using both descriptive and inferential statistics. Descriptive statistics made use of means and standard deviation, histograms and proportions. Inferential statistics used mainly z-test for single proportion and odds ration as a test for associated risk estimates. The study put into consideration critical ethical issues of research involving human subjects mainly informed consent, confidentiality and ethical approvals.
3. Results
3.1. Descriptive Summary of Household Factors
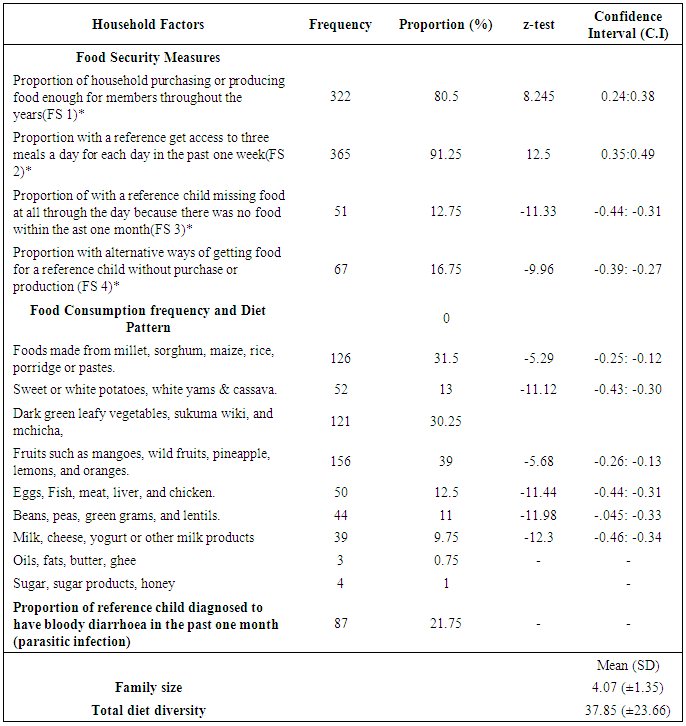
- The finding in Table 1 shows distribution of selected household factors among eligible households. Food security factor which had four indicators revealed that food access and food production were the most dominant food security measures among households at 91.25% and 80.5% respectively. These proportions were significantly higher than expected frequency.
|
3.2. Family Size Distribution
- The findings of this study revealed that each household had at least four members depicted by a mean of 4.07 (±1.35). The range of family size was 1-11 children with normal distribution (skewness=1.162). This distribution is shown in figure 2. This information implies that a household in Obunga slum will have at least 4 members any time one makes a visit assuming that other factors like fertility rate or death remain the same. Six members were randomly left out in the calculation of mean.
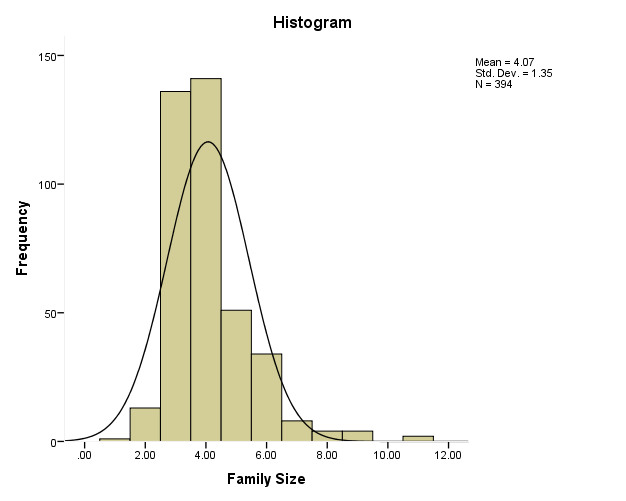 | Figure 2. Distribution of the households by family size |
3.3. Total Diet Diversity Score Distribution
- The mean diet diversity score calculated by total number of food groups consumed from 7 food group categories was 37.85 (±23.66). This shows a wider variation of total diet diversity score among households due to a larger size of standard deviation. However, this distribution pattern still displayed a normal distribution (skewness=-0.031) and a range between 0-96. This shows that the diet diversity score for each household had a true representation of the consumption pattern that is ideal and representative of usual pattern.
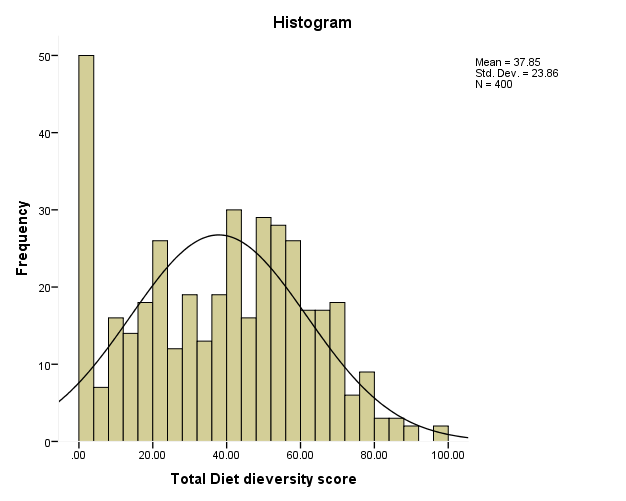 | Figure 3. Distribution of households by total diet diversity |
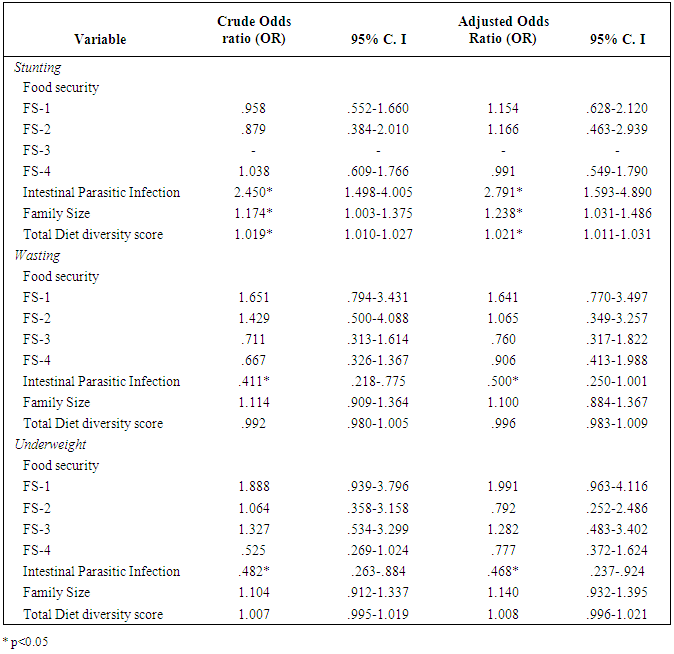
3.4. Influence of Household Factors on Nutritional Status
- Table 2 shows multivariate binary logistic regression of selected household factors in the equation. Based on the previous coding of stunting an Adjusted multivariate analysis was performed to establish the association between household factors and stunting. The results revealed that intestinal parasitic infection was highly associated with stunting (Adjusted odds ratio=2.79, C.I =1.59-4.89, P<0.05. This implies that an increase in 1 unit of intestinal infection was more likely to increase stunting by 2.79 times. Family size was also significantly associated with stunting (Adjusted odds ratio =1.238, C. I=1.031-1.486, p<0.05). This finding implies that for a 1-unit increase in family size increases stunting by 1.238 times. Total diet diversely score gain was highly associated with stunting (Adjusted odds ratio=1.021, C. I=1.011-1.031, p<0.05). This also implies that 1-unit increase in total diet diversely score increases stunting by 1.021 times. All indicators of food security (FS-1, FS2, and FS4) displayed no significant relationship at all with stunting and food security (F3) was invalid in the equation.
|
4. Discussion
- The aim of this study was to determine household factors that influence nutritional status among children 6-59 months within households in Obunga informal settlement in Kisumu city, Kenya. Parasitic infections, family size and diet diversity score revealed significant influence on both HAZ and WHZ. This implies that this category of household factors had considerable effect on both chronic and acute malnutrition of children. These results first, concur with previous studies where there has been strong linkage between helminthes infection and HAZ (Shang et, 2010; Mook and Leslie, 1986). However, parasitic infection somehow decreased wasting and had a significant inverse relationship with wasting. It could be that during infection children who were recovering from symptoms after treatment could have gained weight quickly and during increased level of food intake in view of their condition or parents were becoming more attentive to feed the children. Strong linkage between infections and nutritional status has been a typical outcome in urban schools in slums (Amuta and Housou, 2009) and this concurs and ascertains the outcome for the current study where there are evident relationships. Probably this situation could be explained by a study that identified several environmental related factors such as poor hygiene, overcrowding and culture access to clean water as the theory behind increased menace of common infection-Ascaris lumbricoides, hookworm and trichuris trichiara (Mengistu et al., 2007). Secondly, significant effect brought about by family size on status of HAZ and WHZ also occurs with a study especially for WHZ (Eltishman et al. 2011). Family size has major influence on intra-household food distribution and this also determines food distribution which also determines food access by individual children. Thirdly, diet diversity which is a measure of quality of diet and a proxy outcome of food security as household level significantly influenced HAZ and WHZ. The evidence of this study was a true confirmation of Arimond and Ruel (2004) study as well as Rah et al. (2010) study outcome. These scenarios seemed to be recurrent in urban settings, depriving typical situations in urban slum dwellings.It appears that WAZ did not show linkage with household factors except to parasitic infection which was inversely associated with underweight in a similar pattern as wasting. By proxy explanation, underweight being a short measure for hunger could have been reduced by infection due to possible weight gain during increased level of food intake in view of their condition or parents were becoming more attentive to feed the children Thus outcome was contrary to the findings of Hatloy et al. (2000). However, due to the fact that WAZ is a fluctuating index and a measure of acute hunger, the outcome could be unpredictable in relation to household factors.
5. Conclusions
- In conclusion, based on the findings it appears that when all the three blocks of factors are put together and considered interactively HAZ is hierarchically predicted by food security, intestinal parasitic infection, family size, diet diversity score and health seeking behavior in that order. The study recommends that interventions targeting reducing levels of malnutrition within Obunga informal settlement and other informal settlement with similar characteristics should focus on boosting food security, promoting positive hygiene practices, reducing family size through family planning and emphasize on diet diversity.