-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Food and Public Health
p-ISSN: 2162-9412 e-ISSN: 2162-8440
2016; 6(3): 65-74
doi:10.5923/j.fph.20160603.02

Food Hygiene Awareness, Processing and Practice among Street Food Vendors in Ghana
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLElvis J. Dun-Dery 1, 2, Henry O. Addo 1, 2
1Department of Population, Family and Reproductive Health, School of Public Health, College of Health Sciences, University of Ghana, Accra, Ghana
2Faculty of Public Health and Allied Sciences, Catholic University College of Ghana, Brong-Ahafo Region, Sunyani, Ghana
Correspondence to: Elvis J. Dun-Dery , Department of Population, Family and Reproductive Health, School of Public Health, College of Health Sciences, University of Ghana, Accra, Ghana.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Food poisoning and other food borne diseases could occur through poor hygiene practices, especially in areas where food and drinks are served. In most cities around the world, selling of whole meals on the streets is an important means to generating income. Unfortunately, the emergence of informal food businesses can cause health problems if the foods are not prepared and handled under hygienic conditions. Therefore, there is a need to look into the operations of food vendors to ascertain whether they are adhering to proper hygiene practices. The study was descriptive cross-sectional in design with a Multi-stage sampling technique applied in selecting 266 food vendors. Study specific structured questionnaires were used in the data collection. Data were entered into statistical product and service solutions version 20 for analysis. Absolute and relative frequencies were displayed using tabulations. Chi-square test was done to ascertain the associations between the practice of food hygiene and various explanatory variables. Multiple logistic regressions were used to test the strength of associations between various variables and the outcome variable. There was almost a universal awareness of food and personal hygiene among vendors (90%). As a result, a greater percentage of the vendors adhered to basic hygiene practices (87%). The study found that storage of food for resale (Chi-square=256.329, p-value<0.001) and the use of hand in serving food, (Chi-Square=17.035, P<0.001) were the main predictors of food hygiene practice among vendors. After controlling for confounders through adjusted odds ratios, only awareness that the source of water can contribute to food hygiene, was a determinant of food hygiene practice (OR 0.548, CI 0.316-0.948). In assessing the frequency of hand washing, majority (44%) washed hands every 20-30 minutes, and 42% at each serving. Those who washed every 1hour were 14%. Considering that a percentage of vendors are yet to adopt basic hygiene practices, it will be prudent to ensure continuous education and enforcement of policy regulations within the food industry.
Keywords: Food and personal hygiene, Food vendors, Food-Borne illness, Food poisoning
Cite this paper: Elvis J. Dun-Dery , Henry O. Addo , Food Hygiene Awareness, Processing and Practice among Street Food Vendors in Ghana, Food and Public Health, Vol. 6 No. 3, 2016, pp. 65-74. doi: 10.5923/j.fph.20160603.02.
Article Outline
1. Introduction
- Globalization of food trade has focused its attention on strengthening measures taken to ensure quality and safety, especially on finished foods, and different countries have developed specific regulations to ensure food safety and hygiene [1]. Food and personal hygiene are known to prevent several food-borne diseases when practiced. It is broadly acclaimed that deliberate or accidental contamination of food due to improper handling of food might endanger the lives of consumers [2]. Several hygiene practices such as poor personal and environmental hygiene, inadequate storage of food and drinks, improper preparation and cooking are known to compromise the safety of food [3]. In the last decade, street food vending has expanded rapidly to provide a wide range of inexpensive foods for public consumption. This industrial expansion is however not without problems. The increasing relevance of food consumed away-from home brings new challenges for public health policies [4]. Food safety is now a major public health concern and cases of outbreaks have recently been recorded, both in Ghana and Africa at large [5]. Diarrheal diseases due to contaminated and unhygienic food are among the leading causes of illness and deaths in low-income countries, and several outbreaks of disease have been attributed to consumption of street food [6]. In Ghana, diarrhea has been recognized as one of the major causes of hospitalization, resulting in 16% deaths among African children younger than five years [7]. Food-borne Illness or food Poisoning is any illness associated with eating food contaminated by disease-causing bacteria, viruses, or parasites; natural toxins in plants or animals [7]. Food is said to be hygienic when it contains no hazardous substance that could be harmful to human or animal health [8]. Though this is the case, microbiological hazards in ready to eat food and chemical hazards, mostly pesticides from agricultural products including fresh vegetables and fruits have been highlighted [9]. Recent reports also highlighted the danger of high levels of heavy metals including lead, cadmium, arsenic, mercury and copper from utensils, raw materials or transport methods used [9]. Other studies have taken a look at consumer behavior for possible answers to questions such as: why, what, when, where and how vendors purchase raw materials for processing [4]. Ensuring food hygiene and safety practice among vendors is one challenge that has existed for decades, and therefore the need for vendors to adhere to high standard food safety regulations and hygiene practices cannot be overemphasized [10]. However, a preventive strategy based on thorough analysis of prevailing conditions to ensure the achievement of quality assurance programme objectives is also recommended [1]. There has been an inadequate supervision and monitoring by food safety officers, and the enforcement of food hygiene regulation has been weak [11].Although Ghana has implemented several policy mechanisms to control food contamination, several sources of contamination still exist that are difficult to control. Poor sanitary conditions like open gutters, flies, improper waste disposal, and overcrowding are still persistent dangers to food hygiene [12]. An estimated hospitalization in Ghana due to food related diseases stands at 420,000 per year, with an annual death rate of 65,000 people [8]. Even vendors who exhibit knowledge about food hygiene still find it difficult associating dirty hands with the transmission of diarrheal pathogens in Ghana [6]. Just to say the least, the sources of food contamination are but few of the roots and sources of contamination that are known in the limelight. Very little is usually known and explored about how street food vendors themselves perceive food safety and how to practice it. The objective of this study is to explore the practices and perceptions of vendors on food and personal hygiene and the challenges encountered by environmental health officers in implementing hygiene standards and policies in Ghana.
2. Materials and Methods
2.1. Study Design, Area and Population
- The study was a descriptive cross-sectional in design and employed only quantitative and qualitative data collection methods, using structured questionnaires to gather data from the six Sub-districts across the Wa Municipality of the Upper West Region. The Wa Municipal is one of the nine districts in the Upper West Region of Ghana and its capital is also the regional capital. The population of the region in 2014 based on the year 2010 Population and Housing Census’ projected growth rate of 1.9% is 702,110.The target group used for this research was the estimated 862 food vendors operating in the Wa municipality, from which the sample size was picked. All food vendors in the Municipality formed part of the study population. The researchers also included the environmental officers to assess their level of intervention in ensuring food hygiene, resulting in a sample size of 266 vendors.
2.2. Sampling Technique
- Food vendors from the various Sub-municipalities were selected using a multi-stage sampling technique. First of all, using stratified sampling technique, the six Sub-municipals numbered with alphabets A-to-F were divided into 12 main zones, with each Sub-municipality having two sub-zones. The vendors in the lower and second cycle institutions formed the first zone in each Sub-municipality and all the non-school based food vendors were also grouped into the second zone. The zones within all six sub-municipalities were numbered beginning with those in Wa central, Kambali sub, Bamahu sub, Charia sub, Charingu sub, and Busa sub respectively, resulting into 12 zones. Data on the number of communities in each Sub-municipality were taken and the communities in which food vendors operated were identified using convenience sampling technique. Wa central had 53 communities with vendors in only 42 communities. Thus, (42/53) * 100 = 79.25%; therefore, 79% of 42 = 33 communities for Sub-Municipality A (Wa Central) – 33 communities were sampled in Wa Central. The same method was used for the number of sampled communities in the other Sub-municipalities, with respect to the number of communities in it and the number in which vendors operated. Every vendor in schools which constituted the first zone in each Sub-municipality was sampled by convenience sampling technique. A systematic sampling technique was however used to sample every first and third vendor in communities which also constituted the second zone in every Sub-Municipality.
2.3. Data Collection
- The researchers interacted with vendors using interviewer administered questionnaire. The researchers sought the consent of the vendors prior to administering the questionnaire. Recruited research assistants were also given orientation to help administer questionnaire. They were given guidance on the purpose and focus of the research, the administration of complete questionnaires without any form of coercion, and handling of unresponsive interviewees during the process.
2.4. Data Analysis
- The data entry and analysis was performed using the Statistical Product and service solutions (SPSS version 20) processing software. Administered questionnaires were collated at the end of each day. All necessary differences and errors were usually rectified before the processing. The data was usually processed afterwards into statistical bar graphs, pie charts, and frequency tables. Uni-variate analysis was used to generate both absolute and relative frequencies. Bi-variate analysis (chi-square test) was also used to test association between outcome variable and independent variables. The p-value was adjusted from 0.05 to 0.25 to enable the establishment of as much statistical relationship as possible [13]. The analysis further included the calculation of odds ratios to test the strength of association between independent variables and the practice of food hygiene.
2.5. Ethical Considerations
- Ethical clearance was sought from the Ethics Committee of the Wa Municipal Health Directorate, the Municipal Assembly and from the various representatives of the Sub-district health centers in all the Municipalities. The participants were also duly informed that their participation in the study was purely voluntary and as such they could choose to partake or not. Confidentiality of their responses however was of high priority and was not compromised in any way.
3. Results
3.1. Background Characteristics of Respondents
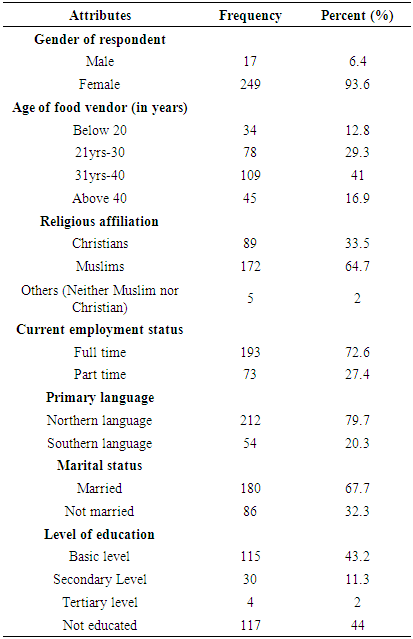
- The study respondents comprised 266 food merchants operating within the municipality. Overall, 94% of the vendors were females with most of them (41%) being between ages 31 years and 40 years. A greater proportion were Muslims (65%) and 73% operated as full time vendors. Majority of the vendors (80%) were of the northern tribe, 68% were married and 44% of the vendors had not experienced any level of formal education (see Table 1).
|
3.2. Awareness on Food Hygiene
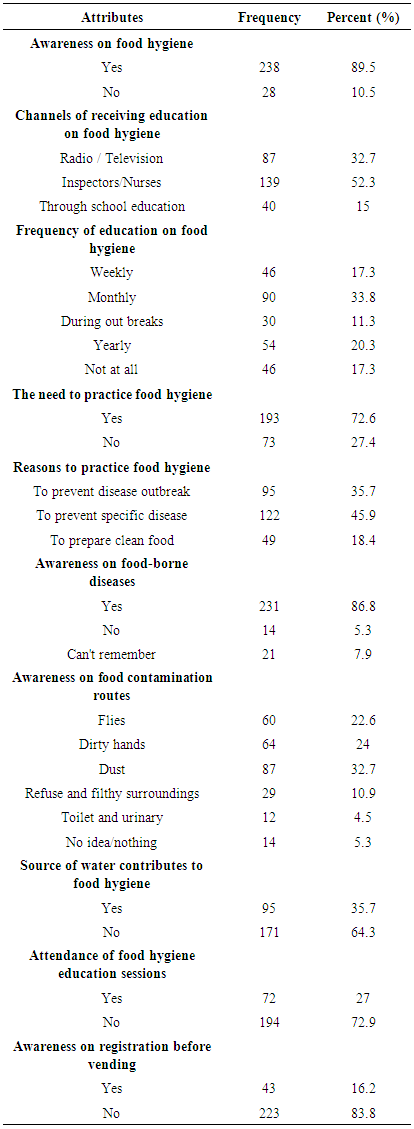
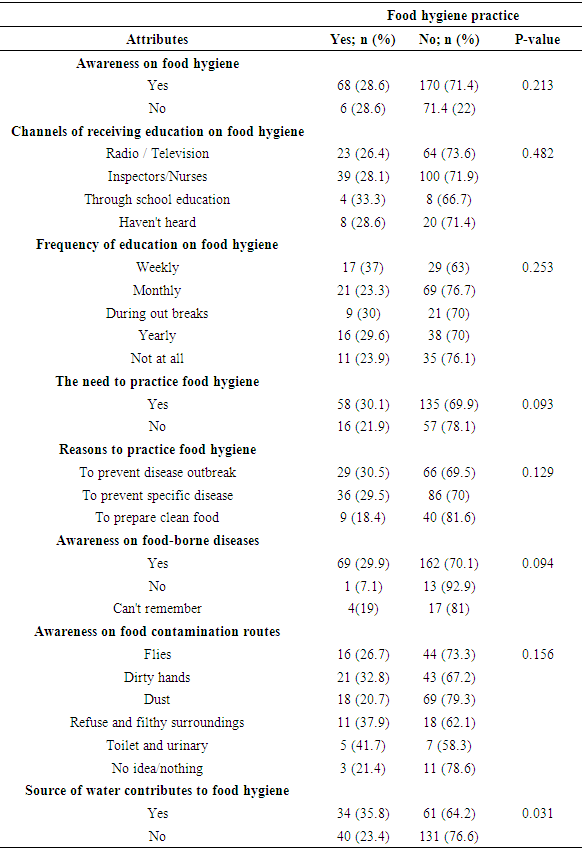
- Awareness on food hygiene was almost universal (89.5%) with majority of the respondents (52%) receiving food hygiene education and information from hygiene inspectors and nurses (52%). Radio and television were other sources of information (33%) and the least group was through formal school education. This results in an 87% food hygiene practice rate. The findings further revealed 87% being knowledgeable on food borne diseases. Most respondents (34%) confirmed being educated monthly and yearly (20%), however, 17% of the vendors never received any form of education on food hygiene. Overall, seven in every ten of the respondents (73%) agreed there was a need to practice food hygiene. About half of the respondents (50%) were aware that preventing specific diseases was the reason to practice food hygiene, 36% were also aware that preventing disease outbreak, and preparing clean (18%) were reasons vendors should practice food hygiene. Of note is also the fact that more than half of the respondents (64%) were unaware that the source of water can contribute to food hygiene, but 24% mentioned dirty hands and flies (23%), as sources of food contamination. In addition to that, 73% did not attend any organized hygiene education sessions and 84% were unaware they needed to be certified before operating as vendors. Other details are given on Table 2.
|
3.3. Food Storage, Processing and Routes of Contamination
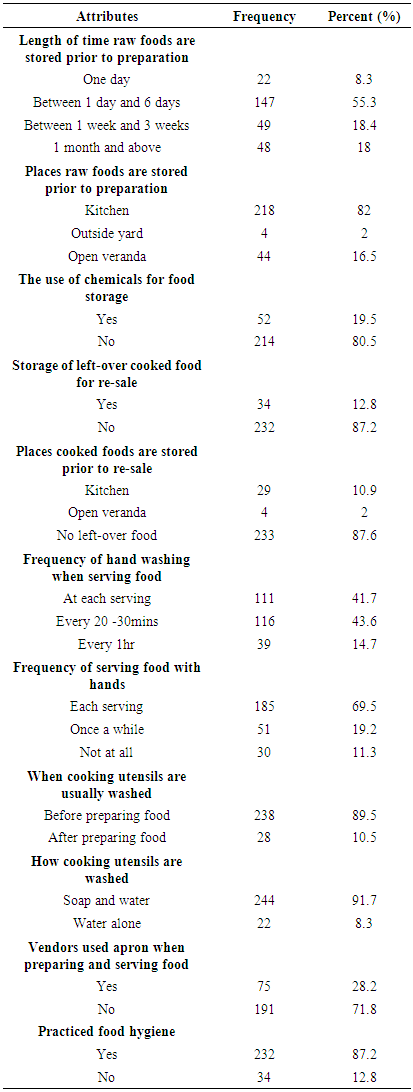
- The study revealed that, above half of the respondents (55%) stored raw food for one day to 6 days while 18% stored raw food between one week to 3 weeks and one month respectively. Only a small proportion of the respondents stored food a day prior to preparation. Among those who stored food prior to preparation, about eight in every ten (81%) of the vendors do not use chemicals in food storage. Majority (82%) of the respondents used the kitchen as a storage facility, while others (17%) stored raw food in open verandas. The rest stored food outside their yards. Two-thirds of the respondents never stored left-over cooked food for re-sale and even those who stored left-over cooked food (13%), only 11% used the kitchen as a storage facility. It is worth noting that, a greater proportion of the vendors (70%) still used their hands in serving each meal, only 11% never served meals with hands while 19% used hands just once awhile. Upon this, only 42% washed their hands before serving each meal. Those who washed their hands every 20 to 30 minutes were 43%, the rest practiced hand washing only on hourly bases. Close to all respondents (90%) washed cooking utensils before preparing food and 92% use soap and water in washing utensils. However, three-quarters of all vendors were not using aprons during food preparation and serving stages (See Table 3).
|
3.4. Associations between Background Attributes of Respondents and Food Hygiene
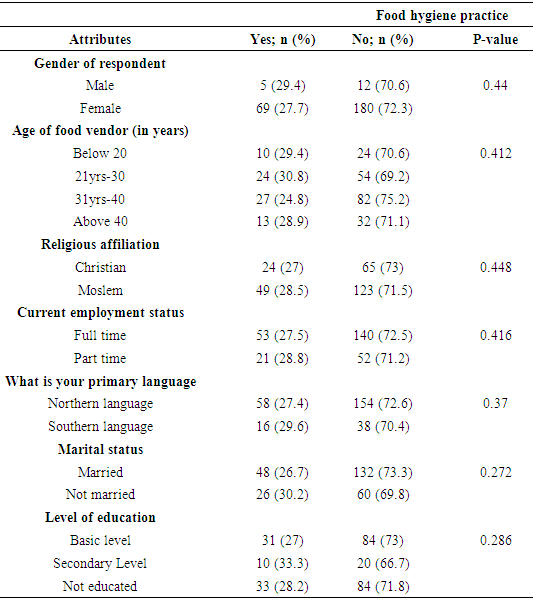
- An established relationship between the background characteristics of respondents and food hygiene was performed using bivariate analysis and a significant p-value of 0.25. The p-value was adjusted from 0.05 to 0.25, considering the Hosmer DW goodness of fit statistic [13], to enable the study reveal as much relationship as possible. The results however indicated no established statistical relationship between background characteristics and food hygiene practice (refer to Table 4).
|
3.5. Associations between Hygiene Awareness and Food Hygiene Practice
- Respondent’s awareness on food hygiene was also explored to ascertain its possible relationship with food hygiene practice during food processing. The results suggested a statistical relationship between vendor’s awareness and their practice of food hygiene (p<0.21). Frequency of hygiene education (p<0.25), knowledge on the need to practice food hygiene (p<0.09) and awareness on the reasons to practice food hygiene (p<0.12) were all statistically related to the practice of food hygiene. Similarly, awareness about food borne diseases (p<0.09) and food contamination routes (p<0.15) were also associated with food hygiene practice. In addition, considering that vendors were unaware that the source of water used for cooking contributes to food hygiene, also influenced their practice of food hygiene (p<0.03). All other variables were not associated with the practice (see Table 5).
|
3.6. Associations between Some Selected Characteristics and Food Hygiene Practice
- The study also examined the relationship between some selected variables and their likely influence on the practice of food hygiene. Type of facilities or storage places used for the storage of raw foods (p<0.20), the length of time food is stored (p<0.25), as well as the use of chemicals in the storage of food (p<0.11), were all significantly related to the practice of food hygiene. Secondly, the type of facilities where left-over cooked foods are stored (p<0.22) and how cooking utensils were washed (p<0.15), were also associated with vendor’s practice of food hygiene. On the other hand, whether cooked foods were stored for re-sale or not, did not have any significant relationship with the practice of food hygiene (see Table 6).
|

3.7. Associations between Some Selected Characteristics and Food Hygiene Practice (Multiple Logistic Regressions)
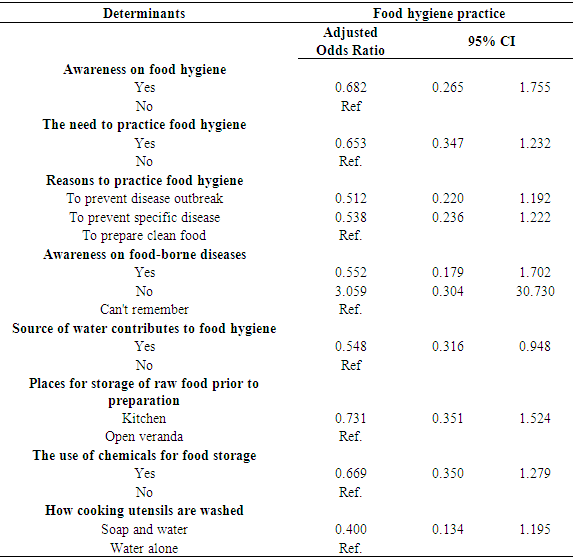
- Adjusted odds ratios were also calculated to determine the strength of association between independent variables and the practice of food hygiene. The results indicates only awareness that the source of water can contribute to food hygiene was a determinant of food hygiene practice (OR 0.548, CI 0.316-0.948). Contrary, all other variables in the model did not predict the practice of food hygiene (see Table 7).
|
4. Discussion
- From the findings of this study, majority of the vendors were females while other studies reported equal percentages for both genders [2]. Similarly, Apanga [5] and colleagues reported majority of females being food vendors in the Northern region of Ghana, a study area with similar characteristics to that of the current study. Other studies have revealed that men are reported to be high risk takers in food handling and preparation issues [14]. If this is the case, it is anticipated that the practice of food hygiene will be high among the female population, which is associated with the current study. In both developed and developing countries, a wide variation in the age of street food vendors has been observed [3], similarly, the current study has reported variations in the age of vendors. Ages ranged between less than 20 years to above 40 years. Both this study and that of Annor & Baiden [2], found age not to be a determinant of vendors’ knowledge and practice of food hygiene. With regards to education, while this study reported majority of vendors not attaining any form of education, [3], again reported findings contrary to this study. Conversely, while education did not determine vendors’ level of knowledge on food hygiene in the current study, educational level seemed to influence vendors’ level of knowledge of food safety to some extent [6].The study result indicates that awareness on food hygiene was translated into practice among vendors. The findings revealed that awareness on food hygiene was almost universal (89.5%), and as a result, almost all vendors (87%) operating within the Municipality were practicing food hygiene. Contrary to this finding, Ababio [8] and colleagues in evaluating food hygiene awareness and practices of food handlers in Kumasi, a city of Ghana, found that vendors had little understanding and awareness about food hygiene issues. In other studies, a significant number of vendors had knowledge on food-borne diseases, such as typhoid and cholera and their ways of transmission were also mentioned [6].This finding agrees with the findings of this study, where 87% of vendors had knowledge on food-borne diseases and another 94% were knowledgeable about contamination routes. However, contrary findings in a survey of 530 vendors in Ghana, indicated that most consumers did not associate unsafe food with food borne illnesses [15]. The pathways of disease transmission most often mentioned were flies, garbage, gutter and fecal materials [6]. Similar contamination routes were also mentioned by respondents of this study, including hands, flies, dust from roads, untidy surroundings and rubbish. It is widely understood that vendors are in a better position to control contamination and ensure food hygiene if they are knowledgeable on the sources of contamination. For each of the foodborne pathogen under active or passive surveillance, information on food vehicle association should be given to all food vendors as well as consuming public, particularly vulnerable. In other studies conducted in India on the microbiological quality of street foods, about 64% of the stalls were adjacent to roads [16], a finding that agrees with findings of this study. The implication is that, vended foods that are closer to the roads tend to be easily contaminated due to dust and constant human activities.In Ghana, public health regulations have stated specific requirements for vendors, including medical screening and certification before vending. However, this health demand seems unsuccessful. Among the 266 vendors interviewed, majority (84%) were unaware they needed to be certified before selling food. In line with this, other studies have shared similar views, where majority of the food vendors (60%) interviewed had no health certificates but operated as vendors. Even though this did not influence vendors’ practice of food hygiene, vendors who are infected with some form of diseases will go unscreened and may end up infecting consumers. This process may be slow, but the cycle of public health prevention begins with the critical first step of surveillance and medical screening. When considering food hygiene, food vendors are a point of focus. Their hygiene practices affect a larger section of the population who depend on them for their daily meals [8]. It is therefore imperative that vendors adhered to high standards of hygiene when dealing with food. In past studies, seventy percent of the survey respondents reported that they always washed hands with soap before preparing foods, 20% most of the time and 10% some of the time [12]. This study has also stated findings similar to that of Onyeneho and colleagues, indicating that minority of the vendors washed their hands at some point or the other, while the rest practice hand washing between each meal serving and 20 minutes. Since people who purchase and prepare food (food vendors) for larger populations assumes greater responsibilities for outbreaks, hygiene practices like hand washing, cross-contamination of raw foods and cooked foods, and observation of cooling temperatures for cooked food, are critical measures and important means to controlling food-borne illness. On the side of food preservation, while it is discouraging to notice that some vendors in the Upper West Region still keep left-over cooked food in open verandas for resale, vendors in Nigeria seems to be complying with public health standards. Sixty-four percent of the respondents reported that leftover food was cooled and stored in the refrigerator, 8% allowed the food to cool and froze it while 28% discarded any food that was cooked and not eaten [12]. However, other studies in Accra Ghana have also stated similar practice among vendors, where majority of the females (61.9%) chose to leave some foods outside at room temperature to defrost it. As a policy option, surveillance needs to expand to a more representative population size and include education on food preservation as a strategy to controlling food contamination. If this is not done, the danger is that food is likely to be more contaminated than before, since some pathogens tend to be present in the atmosphere. This study however is not without limitations. One major limitation is that, only food vendors were sampled as respondents. Environmental health / food hygiene inspected were not included to sample their input to the practice of food hygiene. It is therefore possible that hygiene inspectors contributed to influencing the practice among vendors through strict policies and regulations. Another limitation is that the study only covered six sub-districts in one municipality and not the whole region. It will therefore be wrong to generalize the study findings as the regional description of the situation. Furthermore, most of the factors under study were not significant, suggesting that the study may be under powered.
5. Conclusions and Recommendations
- Overall, it was observed that respondents had a reasonable level of awareness on food hygiene. However, some of the respondents still had some gaps in their responses to queries on ‘food hygiene knowledge and practices. Though respondents were found to have satisfactory food hygiene attitudes, results of the individual components of hygiene practices, like hand washing with soap, medical screening and certification, etc., proved that, vendors did not follow strict food hygiene practices. It is therefore important that vendors ensure strict food hygiene practices must, to prevent cross-contaminations of foods served to consumers. Temperature control among most food handlers especially for cooked and left-over food was also not done according stated public health standards. Some food handlers used their hands in serving food. Although hand washing was practiced by a higher percentage of food handlers, the frequency varied among vendors, which requires training. Respondents also supported the idea that in Ghana where money and time are required to improve existing environmental standards, the most efficient way to improve on the hygiene activities of vendors will be through education and regular surveillance. Every nation including Ghana has regulations enacted to protect its people against unsafe practices in the food industry, and the existing agencies needs to be equipped to enhance control. In addition to this, public health policies and reforms are the driving force to achieving safety in food hygiene practices. It is recommended that these policies are enforced strictly with educational components for food vendors, both in Ghana and other countries.
ACKNOWLEDGEMENTS
- We appreciate all the food vendors within the municipality for giving us the opportunity to share their experience. We further acknowledge the Wa Municipal Health Directorate of the Ghana Health Service, all lecturers and departmental heads of the Catholic University of Ghana for their administrative support. Similarly, we are thankful to Frederick Dun-Dery, Elijah Mahama and Richard Iddrisu, for their individual technical inputs during the research.