-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Food and Public Health
p-ISSN: 2162-9412 e-ISSN: 2162-8440
2016; 6(3): 59-64
doi:10.5923/j.fph.20160603.01

Assessment of Food Safety Practices in a Rural Community in Southwest Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLA. A. Fasoro1, C. O. Faeji2, O. I. Oni2, T. Oluwadare1
1Department of Community Medicine, College of Medicine and Health Sciences, Afe Babalola University, Ado-Ekiti, Nigeria
2Department of Medical Microbiology and Parasitology, College of Medicine and Health Sciences, Afe Babalola University, Ado-Ekiti, Nigeria
Correspondence to: A. A. Fasoro, Department of Community Medicine, College of Medicine and Health Sciences, Afe Babalola University, Ado-Ekiti, Nigeria.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Food safety has been a major health challenge in both developed and developing countries. Ensuring food safety is key to preventing food borne illnesses which are contracted through consumption of unsafe foods. The aim of this study was to identify the food safety practices of residents of a rural community in Southwest, Nigeria. The study design was cross-sectional. Five clusters were selected by simple random sampling from the sampling frame. All households in the clusters were sampled to achieve a sample size of 216 households. Data were collected using a semi-structured questionnaire. The results show that majority of the respondents were female (62.2%), Christians (78.1%), married (53.1%), and belong to the Yoruba ethnic group (88.3%). Residents of the community showed good food safety practices with 80.6% reported to always washing their hands before cooking, 90.3% always clean their cooking utensils before and after use, 83.7% always clean their cooking environment, and nearly all (96.9%) reported washing their hands after using the toilet. A statistical association was found between educational level and washing of hands after the use of toilet (p = 0.037). Though the results show a satisfactory level of food safety practice, however, more improvements can still be made. The method of waste disposal and source of drinking water pose a future threat to the health of the community residents. Hence, a call for government’s intervention in providing potable water and modernised waste disposal facilities.
Keywords: Food safety, Community, Practices, Household
Cite this paper: A. A. Fasoro, C. O. Faeji, O. I. Oni, T. Oluwadare, Assessment of Food Safety Practices in a Rural Community in Southwest Nigeria, Food and Public Health, Vol. 6 No. 3, 2016, pp. 59-64. doi: 10.5923/j.fph.20160603.01.
1. Introduction
- A food is a substance taken into the body to maintain life [1] and this food is said to be contaminated when it contains any unacceptable matter which can be in the form of microorganisms, poisons, or physical contaminants such as pieces of glass or metal [2]. Food safety is a science of describing handling, preparation and storage of food in ways that prevent food borne illness. These include a number of routine practices that should be done to avoid potential health hazards. The need for avoidance of foods that are contaminated with harmful bacteria, viruses, parasites, toxins, chemical and physical contaminants are vital for healthy eating. Contamination can occur at any point through its preparation, handling, storage and consumption [2]. Ensuring food safety is key to preventing food borne illnesses which are contracted from consumption of unsafe foods. Food borne diseases are an important cause of morbidity and mortality world-wide but the full extent and cost of unsafe food, and especially the burden arising from chemical and parasitic contaminants in food is still unknown [3]. The signs and symptoms of food borne illness ranges from gastrointestinal symptoms, such as stomach upset, diarrhoea, fever, vomiting, abdominal cramps, and dehydration, to more severe systemic illness, such as paralysis and meningitis, hence emphasizing the importance of food safety and hygiene in the prevention of food borne illnesses [4]. For over 20 years, food safety has been a major health challenge in developed and developing countries. In 2001, over 600 food borne disease outbreaks in American institutions were recorded [5]. In developing countries, up to an estimated 70% of cases of diarrheal disease are associated with consumption of unwholesome food [6, 7] and poor food safety practices may result in foodborne illnesses and multiple hospitalisations [8]. It is also estimated that every year about 76 million people in the United States become ill from pathogens in food; about 5,000 death cases recorded [5]. This is alarming given that food borne illnesses are mostly under-reported, mainly because its symptoms such as diarrhoea and abdominal cramps mirror those of common intestinal infections [9, 10]. A recent study by the WHO investigated 31 global hazards which caused 600 million foodborne illnesses, 420,000 deaths and 33 million Disability Adjusted Life Years (DALYs) in 2010 [3]. The most frequent causes of foodborne illness were diarrhoeal disease agents, particularly norovirus and Campylobacter spp. In the same year, foodborne diarrhoeal disease agents caused 230,000 deaths, particularly non-typhoidal Salmonella enterica and 18 million DALYs were attributed to foodborne diarrhoeal disease agents. Other major causes of foodborne deaths reported were Salmonella typhi, Taenia solium, hepatitis A virus, and aflatoxin [3]. The highest burden of foodborne disease per population was observed in Africa [3]. The burden is borne by individuals of all ages, most especially children under five years of age, and by persons living in low-income countries. About 40% of the global foodborne disease burden was among children under five years of age, [3] which shows the considerable public health impact of contaminated food. In Nigeria, many rural and sub urban regions lack essential amenities and adequate enlightenment or sensitization on importance of food safety [11]. Practices identified as contributing to foodborne outbreaks include improper refrigeration, prolonged handling and inadequate reheating of cooked food and contamination of food by commercial or household food handlers who worked while ill or had poor personal hygiene [8, 12]. Sanitary measures, principles and procedures need to be put in place to ensure that food is free from agents of contamination in order to promote a healthy living practice. Sanitation issues in food production comprises of four components which include quality of the raw food, personal hygiene of the personnel handling the food, the sanitation of the environment where the food is being stored, prepared and served, as well as of the equipment being used [13]. Noncompliance or compromise in the hygiene and sanitation standards of any of these components can result in food contamination and subsequently food poisoning. Epidemiological data on food borne disease outbreaks in this community is not available but poor storage practices coupled with poor personal hygiene and lack of knowledge in food safety practices, which is peculiar with food handlers in rural communities [11], are causes of concern. It is important that consumers can take simple measures to reduce their risk of foodborne illnesses, especially in the home, hence this survey and its enlightenment campaign. This study was aimed at assessing the food safety practices and hygiene of household members of a rural community in Southwest, Nigeria and also giving proper orientation and sensitization according to the WHO standard to promote food safety practices.
2. Material and Methods
- Study designThe study design employed in this study was a cross-sectional design carried out among residents of Are-Ekiti community. The sample size was calculated using the formula for estimation of sample size for a descriptive study. The level of significance was set at 5%. Adjustment was made for non-respondents that may be encountered during the data collection. The sample size estimated was 216 household respondents. The sampling frame used consisted of the names of the streets in the rural community. Five clusters (streets) were needed to achieve the required sample size and they were randomly selected, they were Ilawemo, Idemorun, Ileko, Odo-ode and Olaofe. All the households in the five clusters were sampled. The youngest adult in each household was interviewed.Study populationAre-Ekiti is a rural community located in the Irepodun/ Ifelodun Local Government Area of Ekiti State, Nigeria. Its geographical coordinates are 7° 43’0” North, 5° 18’0” East [14]. The town has an average population of about 10,000 individuals, comprising of both indigenes and non- indigenes. The last census conducted showed that the total population of Irepodun/ Ifelodun local government was 131,330 [15]. There are 14 towns and 27 villages and farmstead in the local government.Data collection/study instrumentThe data was collected between 22nd July, 2015 and 31st July, 2015. The instrument of the study was a standardized and validated semi-structured questionnaire. The questionnaire was formatted using the WHO’s five Keys to Safer Food as a guide [16]. EthicsApprovals to conduct this study were obtained from the Oba of the community, the Alare of Are-Ekiti and the Chief Nursing Officer of the Primary Health Care Clinic in the community. Verbal informed consents were also obtained from each respondent before and/or during data collection. Confidentiality of each respondent’s answers was guaranteed.Data analysisThe data was analysed using Statistical Package for Social Sciences (SPSS) version 20. Descriptive statistics were presented in frequencies and percentages. Categorical variables were tested for associations by using the Pearson’s chi-square and Fisher’s exact tests.
3. Results
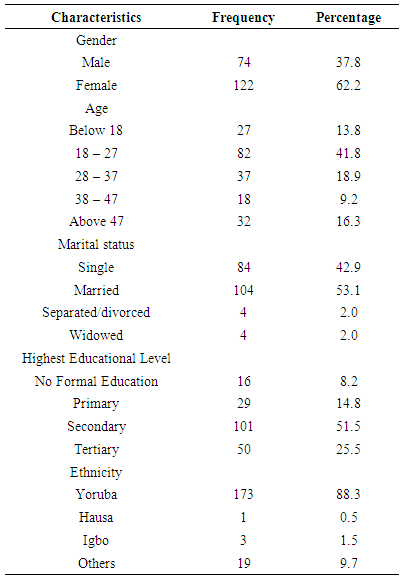
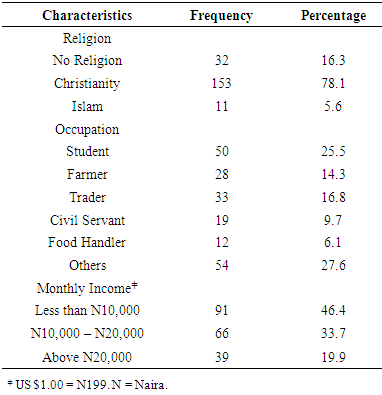
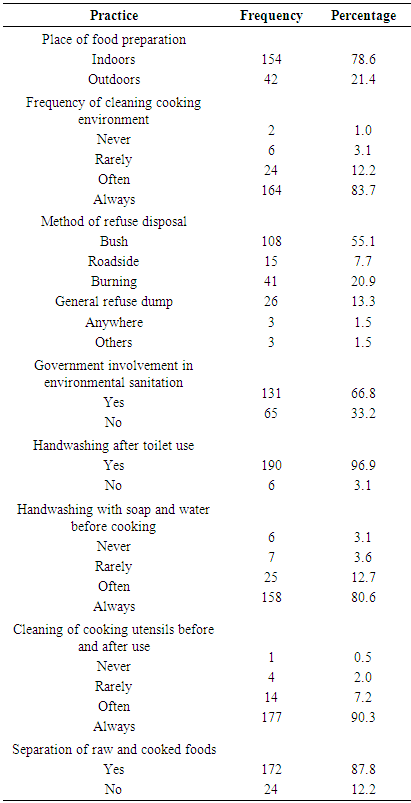
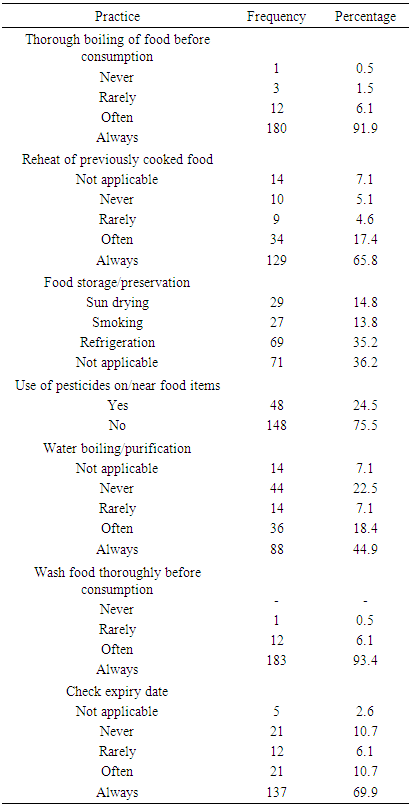
- A total of 216 households were sampled. Valid responses were obtained from 196 respondents giving the study a 90.7% response rate. Sociodemographic characteristics of respondentsThe result of this study showed that 62.2% of the respondents were female. Majority of the respondents (48.1%) were in the 18 - 27 years age group, 53.1% were married, 51.5% had secondary education as their highest educational level and 78.1% were Christians. Nearly all the respondents (88.3%) were of the Yoruba ethnicity. Almost half (46.4%) earns less than N10, 000 as their monthly income.Five keys to safer fooda. Keep clean: To ensure food safety, the individual, utensils and environment have to be clean. Most of the households (78.6%) cook their food in the indoor environment. Nearly all (96.9%) reported washing their hands after using the toilet, 80.6% always wash hands with soap and water before cooking and 90.3% always wash cooking utensils thoroughly before and after use.b. Separate raw and cooked: Only 24 (12.2%) respondents reported storing raw and cooked foods together in a place without anything separating them.c. Cook thoroughly: Bringing the temperature of foods to 70°C while cooking has been shown to make foods safer for consumption. The result showed that 91.8% always cook their food thoroughly before eating, 65.8% always heat previously cooked food before eating while 7.1% do not eat leftovers the following day.d. Keep food at safe temperatures: Storage practices vary across different geographical areas. The least of the preservative method used was smoking (13.8%). Respondents that reported that the question was not applicable to them buy food in small quantities thereby not requiring any storage method for food preservation and this category has the highest percentage (36.2%).e. Use safe water and raw materials: The use of pesticides on food items was also assessed since almost 40% reported pest attacks on their food. Nearly one-quarter (24.5%) of the respondents reported the use of pesticides on/near food items. Only 44.9% always boil/purify their water before drinking while 7.1% buy sachet/bottled water. About 93% always wash their foods/fruits before consumption and 69.9% always check the expiry date of food products before purchase.
|
|
|
|
4. Discussion
- Food safety has remained an important issue in developing and developed world, thus the WHO developed five main keys to safer food, which include keeping clean, separating raw and cooked food, cooking thoroughly, keeping food at safe temperatures, and using safe water and raw materials [16].This study showed the food safety practices among household respondents of Are community. It was observed that 91.8% of the respondents had formal education while just 8.2% had no formal education. This could have influenced the 69.9% of the respondents that do a check on the food expiry date before consumption. Only 16.8% of the respondents rarely or never check for expiry dates of foods. A significant association was found between educational level and washing of hands after toilet use (p = 0.037). All respondents with tertiary education reported washing their hands after use while those with no formal education had the least number of those who wash hands after toilet use. According to WHO, one of the key principles of food safety is the use of safe water and raw materials for food preparation. This study also found that 80.6% of the respondents always wash their hands before cooking. Several studies [17, 18, 19] reported that 87% to 92% of the respondents indicated that food handlers usually washed their hands before handling food, and 62% to 100% usually washed their hands after handling raw meat or poultry. Effective handwashing therefore has been an essential control measure for prevention of pathogens, such as Escherichia coli and Staphylococcus aureus found on the hands of food handlers [20].In addition most of the respondents reported that they cook with clean utensils and always clean their cooking environment. A study in Malaysia found that more than 90% of the respondents in their study had good practice whereby they clean their working areas and wash their hands before working [21]. The residents of this community get their water supply majorly from dug well and rivers. It was observed that 44.9% of the respondents always boil their water before use while 48% respondents do not always boil their water before use. This practice is hazardous and could lead to both food and water borne diseases thereby affecting the health status of the community as a whole. Food safety practices such as the use of pesticides on/near food items showed 24.5% of household respondents engage in such act, as indicated on table 2a, which is also a major cause of food contamination globally. The result obtained from this study also showed the various methods of food storage and preservation practices among the household respondents. Despite increases in the incidence of Lassa fever and increased awareness some respondents (14.8%) still sun dry as a method of preserving their food, 13.8% practice smoking method of preservation, 35.2% respondents are involved in refrigeration while 36.2% respondents said they cook what they can consume at once. Refuse dumps provide a rich source of microorganisms most of which are pathogenic [22]. These refuse dumps thus constitute a habitat for vector and other nuisance organisms capable of transmitting or causing diseases such as typhoid, infantile diarrhoea and cholera in humans and animals [23]. Table 2a showed the refuse disposal method practices with 55.1% and 20.9% respondents practice bush and burning disposal methods respectively. This can cause an increase in food contamination within the environment as related to the results shown on the place of food preparation by the respondents. About 21% of the respondents practice outdoor food preparation while 78.6% prepare their foods indoors. This study employed a cross-sectional study design and as such causal relationships between variables cannot be established. All analyses are based on self-report with the possibility of over and under reporting. The question of food safety and food security remains essential to global health. Thus, strengthening food safety measures will help minimize the burden of foodborne diseases, reduce poverty and contribute to the achievement of the Sustainable Development Goals. Government should help in the management of refuse disposal and provision of potable water for the community. Comprehensive public awareness efforts should be made on the food safety and prevention of foodborne diseases. This study suggests that the residents of this community show a satisfactory level of food safety practice. However, further studies need to be conducted in assessing the burden of foodborne diseases in this community and also the common microorganisms, as well as chemicals involved. Thus, it is important that the people continue to be educated on good hygienic practices and health behaviours with respect to food safety.
ACKNOWLEDGEMENTS
- We will like to express our profound gratitude to the Alare of Are-Ekiti, Oba Jacob Boluade Adebiyi Olofintomilehin III for granting the permission to conduct this study. We also appreciate the effort of Mrs Akejo, the Chief Nursing Officer and the entire community of Are-Ekiti.