-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Food and Public Health
p-ISSN: 2162-9412 e-ISSN: 2162-8440
2015; 5(5): 174-183
doi:10.5923/j.fph.20150505.04
Immediate Risk Factor Associated with Child Malnutrition in Ghana; A Critical Analysis of the Ashiedu Keteke Sub-metro Area in Accra
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbena K. Sarpong 1, Smart A. Sarpong 2, Christian Obirikorang 3, N. N. N. Nsowah-Nuamah 4
1Biomedical Scientist, Department of Medical Laboratory Technology, Kumasi Polytechnic, Ghana
2Research Fellow, School of Graduate Studies, Research and Innovations, Kumasi Polytechnic, Ghana
3School of Medical Sciences, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana
4Rector, Kumasi Polytechnic, Ghana
Correspondence to: Smart A. Sarpong , Research Fellow, School of Graduate Studies, Research and Innovations, Kumasi Polytechnic, Ghana.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
This study investigates malnutrition and its associated risk factors among children under six years within the Ashiedu Keteke sub metro area of Accra. It seeks to determine immediate factors contributing to malnutrition in and around the study area. Specific immediate factors studied include breastfeeding practices and some selected disease. We found more males were malnourished than females. We found 54.0% of children that did not complete their immunization program still sufficiently nourished. With Pearson’s chi-square values of p < 0.001, p < 0.000 and p <0.001 for Wasting, Stunting and Underweight respectively, and with 74.7% of children who completed their immunization found to be well nourished, we conclude that immunization practices significantly reduces the incidence of child malnutrition moderately (Phi = 0.277). Sickle, Pneumonia, Sepsis, diarrhoea, fever and meningitis were all found not to be significant contributors to child malnutrition. We again conclude that over 53.9% of children with birth weight below 2.5kg were actually malnourished. We therefore recommend that, interventions directed to parents or caregivers, should include; nutrition counselling on feeding and care practices, the use of locally available food, improved access to quality foods through grants, the distribution of micronutrients and macronutrient supplementation.
Keywords: Malnutrition, Micronutrients, Pneumonia, Immunization, Caregiver
Cite this paper: Abena K. Sarpong , Smart A. Sarpong , Christian Obirikorang , N. N. N. Nsowah-Nuamah , Immediate Risk Factor Associated with Child Malnutrition in Ghana; A Critical Analysis of the Ashiedu Keteke Sub-metro Area in Accra, Food and Public Health, Vol. 5 No. 5, 2015, pp. 174-183. doi: 10.5923/j.fph.20150505.04.
Article Outline
1. Introduction
- All over the world, malnutrition is a risk factor for illness and death. Millions of pregnant women and young children are affected due to infections, poor and inadequate diet. According to Müller and Krawinkel, malnutrition has the ability to increase the risk and worsens the severity of infections (Müller and Krawinkel, 2005). Torún and Chew also asserts that infants and young children are most affected by malnutrition as they have increased nutritional needs to support growth (Torún and Chew, 1994; Torún, 2006). Undernourished children, as well as children with severe malnutrition, have a higher risk of dying than children with an optimal nutritional status (Caulfield et al., 2004).Literature on child malnutrition suggests that except for sub-Saharan Africa, the nutritional status of children is improving globally. From the account of Duggan and Golden, the expected progress is hindered by poverty, infection and ineffective governance (Duggan and Golden, 2005). Even though global data shows a decrease in under nutrition, the malnutrition statistics for Eastern Africa are increasing (Cartmell et al., 2005). Prevalence of undernourishment in Ghana was last measured at 5% in 2010, according to the World health organization (WHO, 2010). Population below minimum level of dietary energy consumption (also referred to as prevalence of undernourishment) shows the percentage of the population whose food intake is insufficient to meet dietary energy requirements continuously. There is not enough information available on the prevalence of severe or oedematous malnutrition in communities. The data available from hospitals only shows the severe cases, hence, malnutrition in general is not always recorded because in most cases it is the secondary diagnosis (Duggan and Golden, 2005). Cartmell et al. (2005) found that in the Central Hospital of Maputo the occurrence of malnutrition in the presence of infections, excluding measles, was greater in 2001 than in 1983. More children had marasmus than kwashiorkor in 2001. Possible explanations for this occurrence was attributed to the increase in HIV infection; with marasmic malnutrition occurring more commonly in HIV infected children in South Africa, Maputo and Malawi (Cartmell etal., 2005).Literature on child malnutrition abounds. However, despite the work done in malnutrition and the reduced prevalence of stunting and underweight in some regions, the number of cases hasn’t changed over the last 10 years (Zere and McIntyre, 2003; Müller and Krawinkel, 2005) with about 30 percent of all children in low- and middle-income countries being underweight (Mother and child nutrition, 2007). Malnutrition therefore is and will continue to be a health threat to developing countries.This study investigates malnutrition and its associated risk factors among children under six years within the Ashiedu Keteke sub metro area of Accra. It seeks to determine immediate factors contributing to malnutrition in and around the study area. Specific immediate factors studied include breastfeeding practices, weaning, dietary intake and disease.
2. Method
2.1. The Study Setting
- Princess Marie Louise hospital is a Ghana health service healthcare institution located in Accra, within the Ashiedu Keteke sub metro of the Greater Accra region that provides medical care services, pursues diseases control and offers reproductive and child health (RCH), family planning (FP) and nutrition services. Ashiedu Keteke Sub-Metropolitan District Council is the smallest among the eleven Sub-Metropolitan Districts of Accra with a population of about 250,000 people (GSS, Census 2010). It was established by Legislative Instrument 1722. It consists of three electoral areas - Kinka, Ngleshie and KorleWokon.Currently, the hospital has a total of 265 staff with 6 permanent doctors and 81 nurses .The medical service of PML consists of 74 beds, an out-patient Department (OPD), Emergency ward, Laboratory unit/blood bank, X-Ray Unit, Dietetics and Environment Health Unit, Mothers’ Hostel, Disease Control Unit, Family Planning and Reproductive and Child Health (RCH) units, among others.
2.2. The Study Design
- The main focus of this study is to determine the immediate factors contributing to malnutrition in the Accra, precisely the Ashiedu keteke sub-metro where the PLM children’s hospital in located. Data was collected with the help of a structured questionnaire. The questionnaire helped us to gather information regarding background information on mother and child to enable us determine the associations between variables under investigation.The sampling methods consisted of a convenience sample of all children 0-60 months, admitted to paediatric wards / infant care of the PLM children’s hospital, between January and February 2015. In all 163 children with their caregivers were sampled and studied. The inclusion criteria used in selecting the sample include:1. All children 0-60 months who visited the paediatric or infant care units, whose mother/ caregiver was present. 2. All children 0-60 months with a mother / caregiver present that agreed to the verbal consent.For the purpose of this study immediate factors contributing to malnutrition include the following: Breastfeeding and other feeding practices where exclusive breastfeeding and partial breastfeeding are classified as follows: Exclusive breastfeeding: where an infant receives only breast milk and no other liquids or solids, not even water, with the exception of drops or syrups consisting of vitamins, mineral supplements or medicines (Bland, 2007). Partial breastfeeding: where an infant receives some breastfeeds and some artificial feeds, either milk or cereal, or any other food (Bland, 2007). Other immediate factors studied include dietary intake and some selected diseases.The following standardized measurements was used as recommended by Gibson (2005): Weight, Height.- Weight: Older children (above 24 months) were measured using a digital electronic scale, accurate to the nearest 0.1kg. All participants were weighed without shoes and with light clothing on and where possible before a meal and with an empty bladder. The scale was placed on a hard level surface; child stands in the middle and kept still until the measurement was taken (Gibson, 2005). - Children below 24 months were weighed with an infant scale. The child was naked or ware minimal clothing during weighing. The child is then placed on the scale so that the weight was distributed evenly. The measurement would then be taken to the nearest 10g.- Height / Length: children were required to remove their shoes, stand with their heels touching the back of the height measure, legs straight, arms alongside the body, shoulders relaxed and looked straight ahead with their chin level with the ground (Gibson, 2005).- Length of children below 24 months would be measured from the crown to the heel using a paediatric measuring board to the nearest 0.1cm. The measurement would be taken only if the head is level with the headboard and the end of the measuring mat or board is against a flexed heal. The measurement would be taken at eyelevel (Gibson, 2005).
3. Results and Discussion
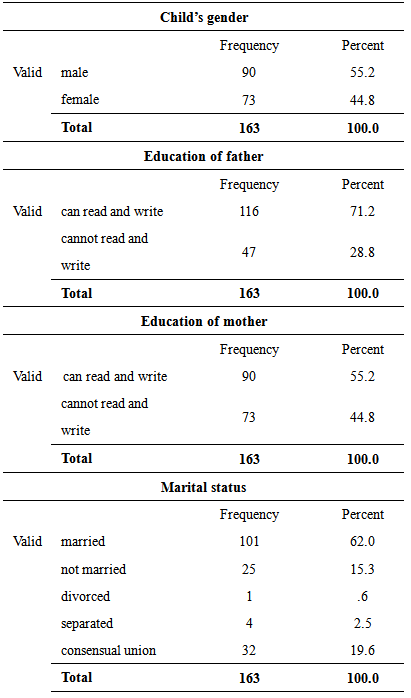
- A total of 163 responses were sought through an in-depth interview with the respondents chosen by a non-probability convenient sampling with specific interest on caregivers with children between six months to five years. In all, 90 out of the total 163 children studied were males representing 55.2% of total respondents while 73 out of the total 163 children studied were females representing 44.8% of the total respondents. Table 3.1 gives a tabular breakdown of the demographic characteristics of Children and caregivers. From the table 3.1, the majority of parents (mothers and fathers) are appreciably educated to the extent that they can read and write. 116 (representing 71.2%) of the father of the surveyed children could read and write whereas 90 of the mothers (representing 55.2%) could also read and write. However, 47 of the fathers (representing 28.8%) and 73 of the mothers (representing 44.8%), could not read and write. Hence, the majority of illiterate caregivers were mothers.
|
|
3.1. Immediate Factors Contributing to Malnutrition
- Immunization practices, diseases and infections like diarrhoea, fever, pneumonia, sepsis, meningitis, and sickle cell were considered to be immediate factors contributing to malnutrition together with breastfeeding practices, exclusive breastfeed and birth weight. The results obtained on them after rigorous analysis is as presented in tables 3.3, 3.4 and 3.5, respectively.
3.1.1. Immunization Practices
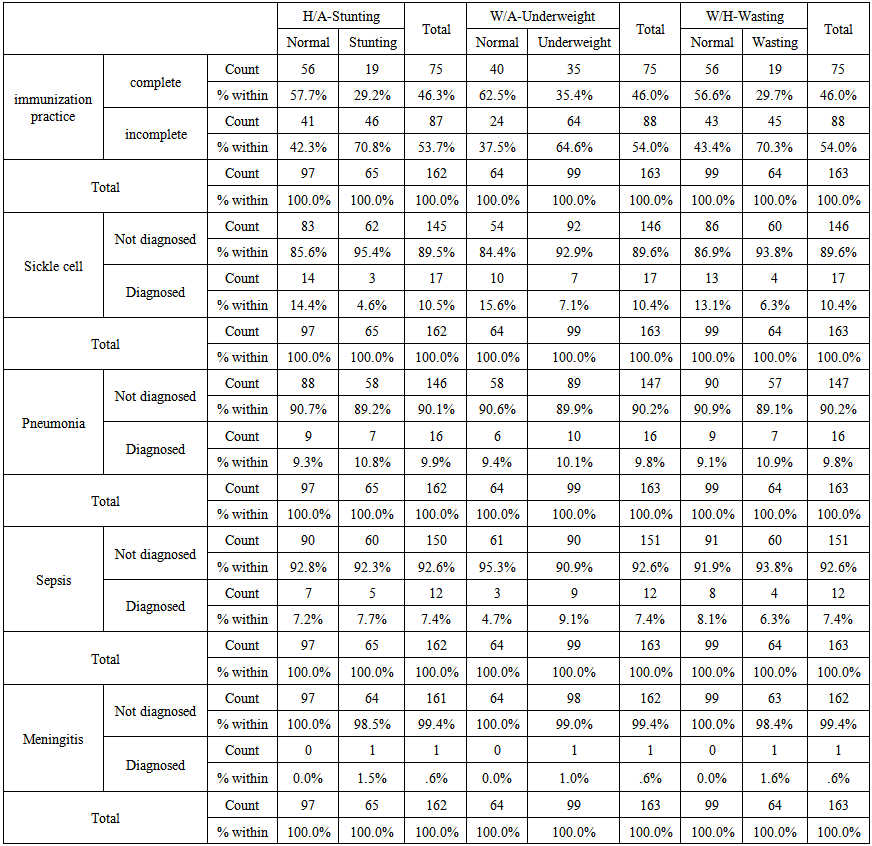
- Immunization practices was the first to be considered by this study and results are seen in table 3.3 below. Our study found that, of the total 163 children, only 75 (representing 46.0%) completed their immunization dose with the remaining 88 (representing 54.0%) failing to complete theirs. According to James et al., (1999) there is a need for improved public health services and improved immunization and growth monitoring programmes. Ayaya et al. (2004) found that incomplete immunizations were a risk factor for the development of malnutrition and Iqbal et al. (1999) found that incomplete Bacille Calmette-Guerin (BCG) vaccination against tuberculosis (TB) increased the risk for the development of severe protein energy malnutrition (PEM) in Bangladesh.
 | Table 3.3. Immediate factors affecting Malnutrition --1 |
3.1.2. Diseases and Infections
- Most deaths of children 6-59 months old are related to malnutrition and infection (Torún, 2006, p.882). Caulfield et al. (2004) found that the principal causes of deaths in young children globally in 2004 were: diarrhoea (60,7%), pneumonia (52,3%), measles (44,8%) and malaria (57,3%). All of these can also worsen malnutrition. Some additional causes associated with child mortality were found by Müller and Krawinkel (2005) and UNICEF (2009, p. 12) and include perinatal causes, acute respiratory infections and others.Our study found that, of the total 163 children, only 17 (representing 10.4%) were actually diagnosed of sickle cell with the remaining 146 (representing 89.6%) being found not to be sickle. It is also observed that, a large percentage of children who were found not to be sickle were either stunting, underweight or wasting. For instance, 62, 92 and 60 of the total 146 children who were found not to be sickle were still found to be stunting, underweight and wasting respectively. Surprisingly, an appreciable percentage of children who were actually diagnosed of sickle cell were found to be normal. For instance, 14, 10 and 13 of the total 17 children who were diagnosed with sickle cell were found not to be neither stunting, underweight nor wasting respectively.On pneumonia, our study found that, of the total 163 children, only 16 (representing 9.8%) were actually diagnosed of pneumonia with the remaining 147 (representing 90.2%) being found not to be with pneumonia. It is also observed that, a large percentage of children who were found not to be pneumonia were either stunting, underweight or wasting. For instance, 58, 89 and 57 of the total 147 children who were found not to be with pneumonia were still found to be stunting, underweight and wasting respectively. Surprisingly, an appreciable percentage of children who were actually diagnosed of pneumonia were found to be normal. For instance, 9, 6 and 9 of the total 16 children who were diagnosed with pneumonia were found not to be neither stunting, underweight nor wasting respectively.Also on Sepsis, our study found that, of the total 163 children, only 12 (representing 7.4%) were actually diagnosed of sepsis with the remaining 151 (representing 92.6%) being found not to be with sepsis. It is also observed that, a large percentage of children who were found not to be with sepsis were either stunting, underweight or wasting. For instance, 60, 90 and 60 of the total 151 children who were found not to be with sepsis were still found to be stunting, underweight and wasting respectively. Surprisingly, an appreciable percentage of children who were actually diagnosed of sepsis were found to be well nourished. For instance, 7, 3 and 8 of the total 12 children who were diagnosed with sepsis were found not to be either stunting, underweight or wasting respectively.Finally on Meningitis, our study found that, of the total 163 children, only 1 (representing 0.6%) was actually diagnosed of Meningitis with the remaining 162 (representing 99.4%) being found not to be with Meningitis. It is also observed that, a large percentage of children who were found not to be with Meningitis were either stunting, underweight or wasting. For instance, 64, 98 and 63 of the total 162 children who were found not to be with Meningitis were still found to be stunting, underweight and wasting respectively. The only one child who was actually diagnosed with Meningitis was found to be severely malnourished.
 | Table 3.4. Immediate factors affecting Malnutrition --2 |
3.1.3. Breastfeeding Practices
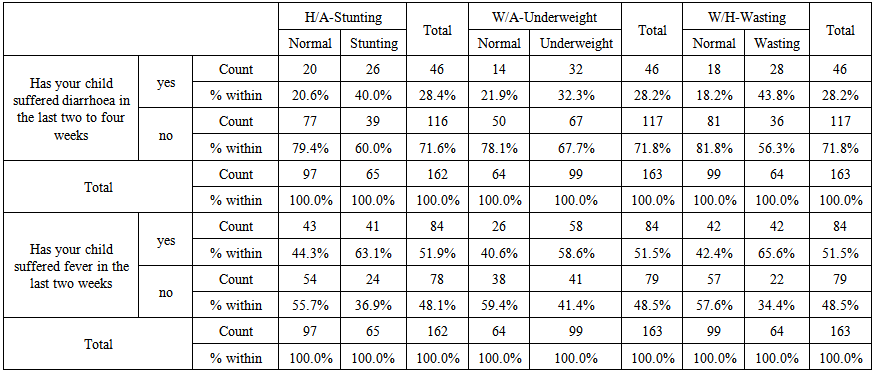
- Even though diarrhoea causes about 30-50% of deaths in developing countries, the risk of death due to persistent diarrhoea is related to a lack of breastfeeding, systemic infections, malnutrition and young age (Ochoa et al., 2004). From table 3.5 below, we sort to find out whether mother started breastfeeding the child immediately after birth, and did exclusive breast feeding. Insufficient dietary intake may refer to poor breastfeeding practices, early weaning, delayed introduction of complementary foods and insufficient protein in the diet. The inadequate intake can also be linked to neglect and abuse (UNICEF, 2004; Williams, 2005, p.405).
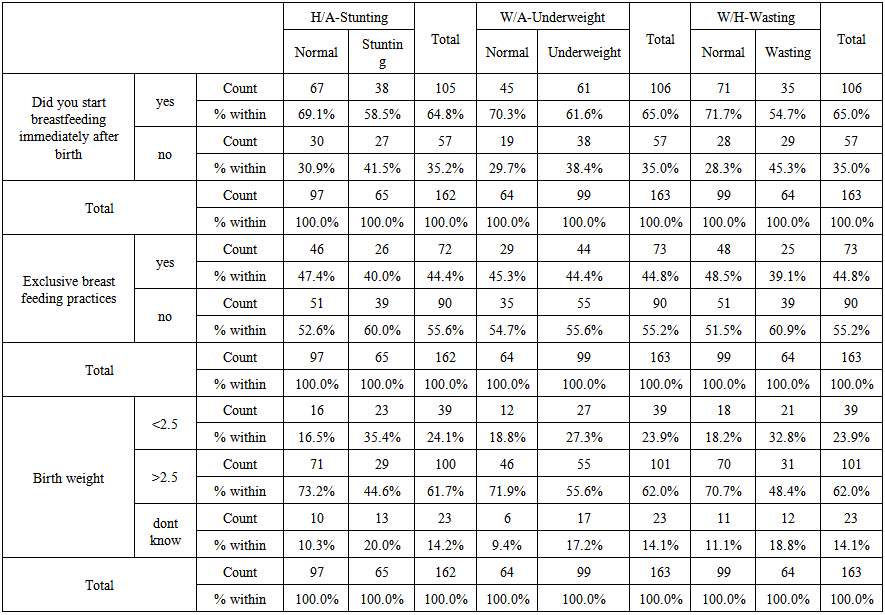 | Table 3.5. Immediate factors affecting Malnutrition --3 |
4. Conclusions
- More males were malnourished than females. With 74.7% of children who completed their immunization found to be normal, we conclude that immunization practices significantly reduces the incidence of child malnutrition moderately. Again, Sickle, Pneumonia, Sepsis, diarrhoea, fever and meningitis were all found to affect malnutrition badly. We again conclude that, over 53.9% of children with birth weight below 2.5kg were actually malnourished.We therefore recommend that, Decisions regarding nutrition related issues should be based on effective collection of data, monitoring and evaluation. International data is, however, also important for guiding national policies and programmes. If no data is available on important interventions, countries will never know if the coverage excludes those that are really in need of programme. Currently availability of reliable data is still a challenge. Infant feeding should not only be the responsibility of the mother. Programmes should address support and approval of the male partner and the maternal grandmother.Interventions directed to parents or caregivers, should include nutrition counselling on feeding and care practices, the use of locally available food, improved access to quality foods through grants, the distribution of micronutrients and macronutrient supplementation.
Supplementary Tables for Significant Tests for Associations
- NOTE: Phi and Cramer's V are both tests of the strength of association. It ranges from weak association (0.00) through moderate association (0.2-0.5) then to strong association (0.6 – 1.0).
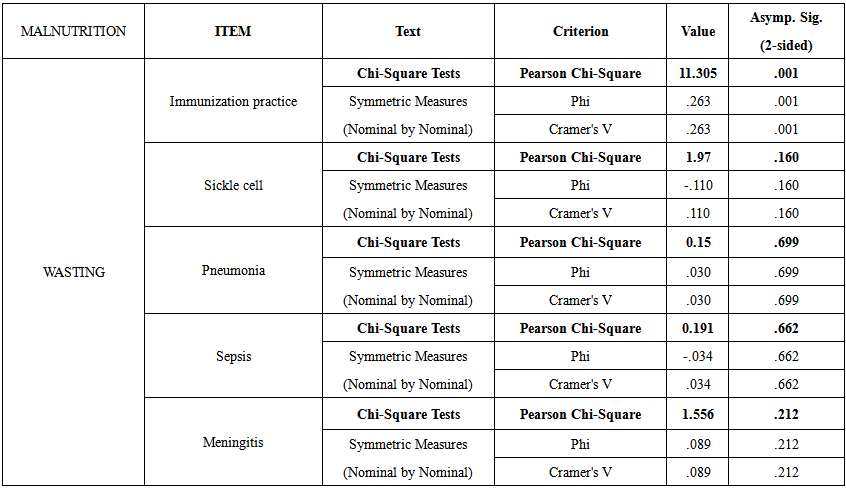 | Table 3.6. Chi-square test results for association between diseases and child malnutrition (wasting) |
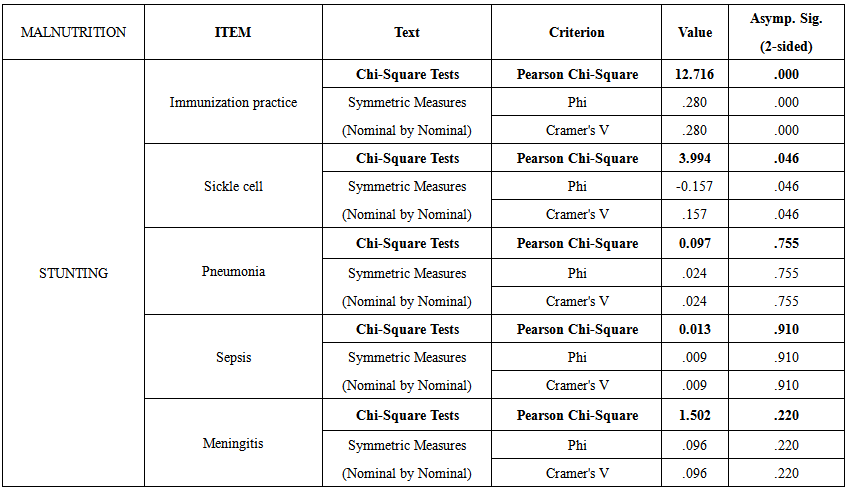 | Table 3.7. Chi-square test results for association between diseases and child malnutrition (stunting) |
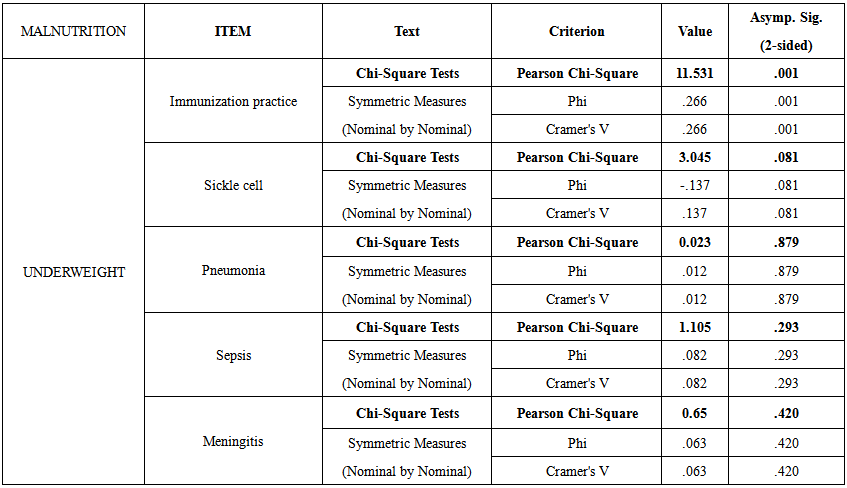 | Table 3.8. Chi-square test results for association between diseases and child malnutrition (underweight) |
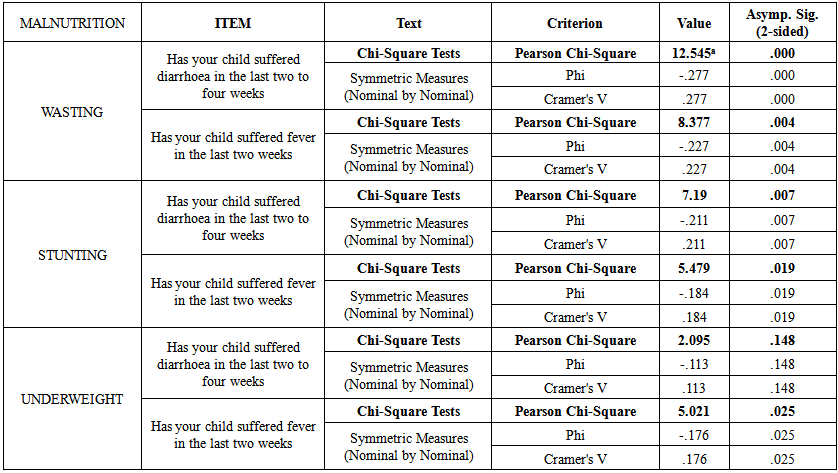 | Table 3.9. Chi-square test results for association between diseases (diarrhoea & fever) and child malnutrition |
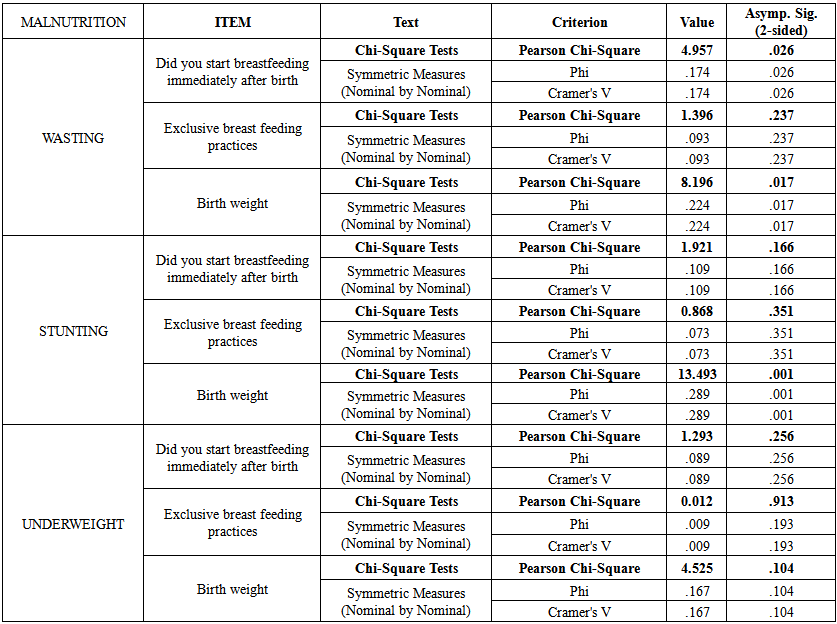 | Table 3.10. Chi-square test results for association between diseases (breastfeeding practices & birth weight) and child malnutrition |