-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Food and Public Health
p-ISSN: 2162-9412 e-ISSN: 2162-8440
2015; 5(3): 70-76
doi:10.5923/j.fph.20150503.02
Assessing Iodized Salt Use in Rural Northern Ghana: A Mixed Method Approach
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLDennis Chirawurah, Stephen Apanga, Jerome Addah
Department of community health and family medicine, School of Medicine and Health Sciences University for Development Studies, Tamale, Ghana
Correspondence to: Stephen Apanga, Department of community health and family medicine, School of Medicine and Health Sciences University for Development Studies, Tamale, Ghana.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Iodine deficiency disorders are a major public health concern affecting an estimated 2 billion people worldwide. As part of efforts to achieve the Universal Salt Iodization goal, the Government of Ghana launched the Universal Salt Iodization program backed by an act of parliament to oversee the attainment of this goal. Notwithstanding these efforts, iodine consumption amongst households and individuals is generally low in the Northern region especially in the Gushegu district. We therefore assessed the current iodine coverage and utilization in households and also determined the causes of low iodine use in this district. A mixed method approach of both quantitative and qualitative designs was employed. A quantitative descriptive cross sectional survey was first used to assess current iodized salt coverage, utilization and causes of low iodized salt use in households. The second design was a qualitative Focus Group Discussions and Key Informant Interviews conducted to give an in-depth inside of the causes of low iodized salt use. Rapid salt testing to determine iodine levels was conducted in all the households. In total, 100 household cooks were interviewed whiles 4 focus group discussions and 7 key informant interviews were conducted. Household iodized salt utilization and coverage was around 20%. Approximately 54% received education on iodized salt whiles 97% were unaware of the law on salt iodization. Reasons for the low use of iodized salt included; high cost and non-availability of the iodized salt, not received any education on the importance of iodized salt and ignorance of the law on iodization of salt. Iodized salt coverage and use in households and knowledge levels of the importance iodized salt is low in this district. High cost and unavailability of iodized salt coupled with ignorance of the law amongst others are responsible for the low use of iodized salt in this district.
Keywords: Iodized salt, Northern Ghana, Gushegu, Mixed method approach
Cite this paper: Dennis Chirawurah, Stephen Apanga, Jerome Addah, Assessing Iodized Salt Use in Rural Northern Ghana: A Mixed Method Approach, Food and Public Health, Vol. 5 No. 3, 2015, pp. 70-76. doi: 10.5923/j.fph.20150503.02.
Article Outline
1. Introduction
- Iodine is a trace element and an essential micronutrient that is often required in small amounts for the normal physiological function of the human body. Iodine has been found to be a key component of the thyroid hormones which are necessary for a number of metabolic and enzymatic processes such as control of the body’s metabolic rate; growth and development; and neuron function and development [1]. Iodine deficiency disorders (IDD) which results from insufficient intake of iodine is a major public health concern affecting an estimated 2 billion people worldwide in over 50 countries [2, 3]. IDD include a wide spectrum of disorders such as abortions, stillbirths, congenital abnormalities, cretinism, goitre and impaired mental function, squinting, dwarfism, mutism and increased infant mortality [3-7]. The vulnerable groups particularly at risk of developing IDD include pregnant women, infants, children and some cases the developing foetus is also affected in the womb [7, 8]. It is estimated that about 120,000 children born each year in Ghana are at risk of developing intellectual impairment as a result of iodine deficiency. Approximately 15,600 accounting for 13% of these babies are severely impaired and are unable to develop properly, resulting in an average of 22 million dollars loss in productivity each year in Ghana. Majority of these affected children are also held back by reduced intelligence and mental disorders which tend to have enormous consequences on the Ghanaian educational system and also serve as a negative implication of iodine deficiency [7, 9]. Iodations of all salt known as Universal salt iodization (USI) for both human and animal consumption, is the major global strategy of choice for feasible and effective control of iodine deficiency. Iodization levels are usually measured based on estimated consumption of salt, with an estimated individual average consumption of around 10 g of salt per day in countries where most of the salt in the diet comes from table salt, used for cooking and at the table. It is recommended by the WHO, United Nations Children’s Fund (UNICEF) and International Council for Control of Iodine Deficiency Disorders (ICCIDD) that, 20 mg to 40 mg of iodine per kg salt be added to food products depending on local salt intake [2, 10, 11]. It has subsequently been recommended that a more cost effective way of addressing the problem of IDD for most developing countries is by adding iodine to universally consumed products such as common salt, as done in most industrialized countries [7, 12-15].A number of baseline studies have been conducted in the past two decades concerning iodized salt use in Ghana. For example in 1994, IDD was found to be 33% in 110 districts surveyed. In this survey, adequate iodized salt use amongst households in Jirapa and Bongo districts in Northern Ghana were found to be only 38.5% and 36.3% respectively [16, 17]. Surveys conducted by the Ghana Health Service to assess the consumption levels of iodized salt in households in 2002, 2003, 2005 and 2006 also revealed that, only 49.1%, 41.5%, 74.1% and 50.8% respectively of households in the country consumed iodized salt [18]. It was later on found that, only 32.4% of households consumed iodized salt adequately in the 2006 survey [18]. In 2005, the Ghana Health Service set a national household iodized consumption target of 90% to be attained by the end of 2005 and sustained by 2011. However a study conducted in 2008 by the service revealed that, only 74% of households consumed iodized salt which fell below the national target [19]. As part of efforts to achieve the Universal Salt Iodization (USI) goal, the Government of Ghana launched the USI program in 1995 backed by the food and drugs amendment act (1996), act 523 established by the parliament of Ghana to oversee the success of the Universal Salt Iodization [2, 7]. Notwithstanding all these efforts, Iodine consumption amongst households and individuals is generally low in the Northern region according to officials of the foods and drugs board in the region [20]. A survey by UNICEF in 2007 indicated that, almost 95% of households in the Gushegu district did not consume iodized salt [21]. Apart from this survey in 2007, no other study has been conducted in the Gushegu district to assess iodized salt use amongst households. Also, most of the surveys concerning iodized salt use have tend to adopt only a quantitative approach, with rarely any qualitative study in Ghana especially Northern Ghana ever carried out to determine the causes of the low use of iodized salt in households. The objectives of this survey were therefore to assess the current iodized salt coverage and utilization in households and also to determine the causes of the generally low use of iodized salt in the Gushegu district which has the lowest iodized salt household use in the northern region of Ghana. The findings of this study would not only be useful to the District Health Management Teams (DHMT) which plans promotional and educational programs on the utilization of iodized salt in Ghana, but will go a long way in helping all stake holders in this field to implement cost effective strategies towards achieving the national household iodized consumption target of 90% by 2015.
2. Methodology
2.1. Study Area
- This study was conducted between June and July 2012 in the Gushegu district which is the third largest district in the northern region of Ghana and located at the North-eastern corridor of the region. There are five administrative sub districts in the district, namely; Gushegu, Katani, Nabuli, Kpatinga and Zinindo sub districts, with two hundred and seventy (270) communities all with similar socio-demographic characteristics and a population of 111,259 according to the 2010 population census.
2.2. Study Design
- This survey employed a mixed method approach in the form of a convergent parallel mixed methods design [23]. This type of design collects quantitative and qualitative data in parallel, analyzes them separately, and then merges the two data sets at the point of interpretation. The integration of quantitative and qualitative data maximizes the strengths and minimizes the weaknesses of each type of these research designs [23]. The first design was a quantitative descriptive cross sectional survey used to assess the current iodized salt coverage, utilization and causes or reasons for the low iodized salt use in households within the district. The second design was a qualitative Focus Group Discussions (FGDs) and Key Informant Interviews (KIIs) conducted to give an in-depth inside of the causes of low iodized salt use.
2.3. Sample Size and Sampling Procedure
- The quantitative sampling involved a random sampling of 100 households from 2 randomly selected sub districts out of the 5 sub districts using OpenEpi [24], with a population size of 111259, hypothesized % frequency of outcome factor in the population of 5% [21] and 10% none response rate. The qualitative sampling comprised of FGDs and KIIs.Due to the multiple strata (sub- districts, communities and households structure) nature of the district, a combination of cluster and simple random sampling techniques was used to select households, household cooks and other participants for the study. From each of the 2 randomly selected sub-districts, 4 communities (2 from each community) were randomly selected after which 25 households and household cooks were chosen for the survey. The KIIs were conducted amongst representatives from the Food and Drugs Board; Ghana` Standards Board; District Assembly; Ghana police service; District Nutrition Officer; District Disease Control Officer and the head of one health facility whiles women’s FGDs were conducted in each of the 2 selected sub districts. Each women’s FGD comprised of 10 members in a group.
2.4. Data Collection Instruments and Procedures
- Quantitative data was collected using a corrected structured pre-tested questionnaire. Pre-testing was conducted in one community that was not included in the actual survey. Qualitative data was collected using an interview guide for the KIIs and a tape recorder for the FGDs.In each of the 100 households, permission was sought to run tests on samples of the salt used for cooking to determine their iodine levels. The tests were conducted using the rapid testing kits. To determine the iodine levels in the salt samples, colour charts on the kit corresponding to values of 0.1-25 PPM, 25.1-50 PPM, 50.1-75 PPM and 75.1-100 PPM were used [25, 26].
2.5. Data Analysis
- Quantitative data was cleaned, entered and analyzed using the Statistical Package for the Social Sciences (SPSS) programme software (version 15.0) with descriptive statistics carried out and summarized in the form of texts and tables.Responses from the KIIs were manually written in interview guide sheets whiles FGDs were recorded and transcribed verbatim from the local language into English for analysis. This data was analyzed manually using themes. The investigators read through all the transcripts exhaustively and coded them. The codes were matched and generated into common themes and sub-themes for the write-up.
2.6. Mixed Methods
- After analyzing the qualitative and quantitative datasets, the results from each were compared at the point of interpretation to identify areas of convergence (similarity) and divergence (difference). Equal priority was given to each type of dataset during the analysis. After merging results and identifying areas of convergence and divergence, recommendations for interventions by stakeholders were subsequently identified.
2.7. Ethical Considerations
- Approval for this study was gotten from the Department of Community Nutrition of the School of Medicine and Health Sciences, University for Development Studies; the District Health Management Team and the District Assembly. Permission was also obtained from the chiefs and elders of the two sampled communities through a community entry process.
3. Results
- A total of 100 people were interviewed for the quantitative data analysis whiles 7 KIIs and 4 women FGDs after saturation was reached were conducted for the qualitative data analysis.
3.1. Quantitative Survey Results
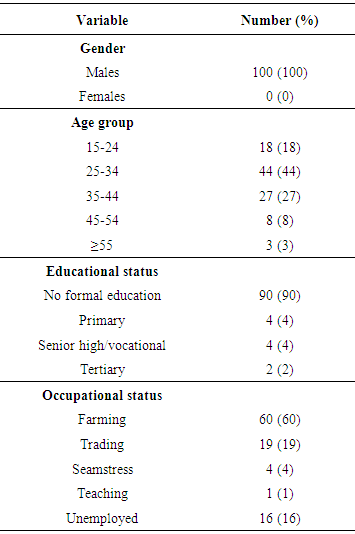
3.1.1. Socio-demographic Status of Respondents
- The socio-demographic characteristics of the respondents are presented in table 1. All the household cooks in this study as shown in table 1 were females. This finding is a reflection of a typical northern Ghanaian setting as women are the ones who tend to prepare meals. Table 1 also shows that 90% of the respondents do not have any formal education.
|
3.1.2. Iodized Salt Utilization, Education and Coverage
- Out of the one hundred (100) respondents interviewed, 23% use iodized salt for household cooking whiles 77% do not. Rapid salt testing in the 100 households showed that 20% of households use iodized salt for cooking whiles 80% do not cook with iodized salt. Responses from household cooks revealed that 54% of them had received education on iodized salt, with the rest not receiving any form of education on iodized salt. Approximately 97% of the respondents were unaware of the law on salt iodization.
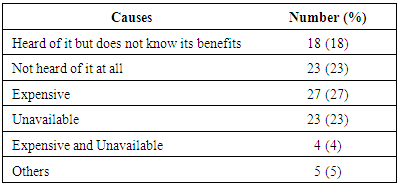
3.1.3. Causes of Low Iodized Salt Use
- A number of reasons were given by the respondents as being responsible for the low or none use of iodized salt in this setting and are presented in table 2. From table 2, the high cost of iodized salt accounted for its low or none use. Approximately 9% of the respondents gave other reasons such as: used to the crystal salt (none iodized salt), both crystal and iodized salt sold together in the market amongst others as being responsible for the low or none use of iodized salt.
|
3.2. Qualitative Survey Results
3.2.1. Key Informant Interviews
- During the KIIs, they identified none compliance to the law on salt iodization to be bad and therefore accounting for the low coverage and utilization of iodized salt in the district. Majority (80%) of the key informants believed that ignorance of the salt iodization law and benefits of iodized salt was responsible for none compliance to the law.“So many people especially those who sell salt in the market are not aware of the existence of the salt iodization law. They do not even know that flouting this law could lead to their arrest. A major contributory factor to the non compliance to the law is because those who flout this law are not being arrested” (key informant, representative of Ghana police service).The remainder 20% was of the opinion that a combination of both ignorance and poverty are responsible for non compliance to the law.On responses from a posed question on how to improve on compliance to the law, six (83%) key informants recommended that more education on the law and benefits of iodized salt be embarked on whiles the remaining one key informant thought people will learn when they see others use iodized salt and its beneficial effect manifests on their bodies.“The only way to improve on compliance to the law is to make sure that we educate and continue to educate community members about the salt iodization law and benefits of iodized salt” (key informant, representative of Foods and Drug Board).
3.2.2. Focused Group Discussion
- The FGDs were conducted amongst 4 female groups (10 members in each group) after a saturation point was reached in each of the two districts to give a deeper understanding of the reasons or factors responsible the low use of iodized salt in the Gushegu district. The responses from these discussions are summarized and presented into various thematic areas.Availability and costBoth groups indicated that iodized salt was not readily available in the market and the few that is even available is often expensive for them.“The powder or iodized salt is usually too expensive. I am able to use fifty (50) pesewas wealth of the crystal salt for one month. However if I were to spent the same amount of money on the iodized salt, it will only last for just one week” (FGD, woman in Garichie No. 1 community).“When you go to the market to buy salt, you only see the crystal one and not the powdered one and so you are compelled to buy what is available. So you see, if even you able to raise the money to buy the powdered salt, you hardly can find some in the market” (FGD, woman in Salinwei community).Lack of knowledge about iodized saltLack of knowledge about the benefits of iodized salt was identified as one of the key contributing factors to the very low usage of iodized salt in both FGDs. Whiles some members of both FGDs indicated that they had no idea of the benefits of iodized salt, some also had no knowledge on the specific benefits of iodized salt and only said they heard from health personnel that too much salt gives poor health. “I was told in the hospital not to use too much salt in cooking. I was also told to use the powdered salt only since it gives ‘alaafe’ (good health)” (FGD, woman in Garichie No. 1 community).Some women from both communities said they were only educated during antenatal care on the need to reduce their salt intake since it has adverse effect on their pregnancy.“Health workers always advise that we reduce salt intake when we have swollen feet but they do not educate us on the importance or benefits of iodized salt” (FGD, woman in Salinwei community).
3.3. Mixed Method Results
3.3.1 Convergence
- Quantitative and qualitative data converged when the results of each data set were similar. Convergent data analysis shows that the reasons or factors mentioned by focus group participants and key informants as being responsible for the low or none usage of iodized salt were also reflected as frequency items in the quantitative survey such as: unavailability, high cost and lack of knowledge of the benefits of iodized salt.
3.3.2. Divergence
- Quantitative and qualitative data diverged when the data sets were dissimilar. After comparing both data sets, the only point of divergence had to do with the knowledge levels of the law of salt iodization by key informants. This difference was to be expected since key informants tend to have much knowledge into the subject area.
4. Discussion
- This study looked at both a quantitative and qualitative approach of assessing iodized salt use in an area with low iodine use in rural Northern Ghana. Household cooks in this study were mainly informal uneducated women and therefore any intervention strategies especially those that seek to promote the consumption of iodized salt should have to target this group the most. Buxton and Baguune also found that females were responsible for meal preparations in a study to determine the knowledge and practices of people in the Bia District of southern Ghana with regard to iodine deficiency disorders and intake of iodized salt [7]. Our finding of 20% coverage of iodized salt use in the Gushegu district shows a marked improvement over that reported in the UNICEF survey since 2007 where about 95% of households were found not to be using iodized salt. This figure however falls far short of the national target of 90% to be achieved in 2015 [19]. Our finding was also low as compared to what was found in Jirapa and Bongo which are considered to be the lowest in terms iodized salt use and coverage in Ghana as reported previously [16, 17].Our study also shows that some knowledge gaps exits in terms of awareness creation and education on the importance of iodized salt in this typical rural northern Ghanaian setting. Our findings of 46.5% of respondents not having any knowledge about iodized salt is however an improvement of an earlier study conducted by the University of Ghana in collaboration with the Ministry of Health of Ghana, from 1991-1993 on IDDs in Ghana where 98% of the respondents had no knowledge about iodized salt [27]. A study in a southern district of Ghana however found knowledge about iodized salt amongst respondents to be 90.4% which is higher than that found in our study. This high knowledge level was attributed to the Food and Drugs Board amendment Act, Act 523 of 1996 on universal salt iodization and the propagation of health education by the Ministry of Health and the Ghana Health Service creating awareness about the importance of iodized salt [7]. Following a collaborative effort by UNICEF and the Ghana Health Service in the Bolgatanga areas of northern Ghana using radio campaigns to teach the community about the benefits of iodized salt, there was a marked improvement of adequate household consumption of iodized salt from 24% in 2009 to 63% in 2011 [28, 29]. Therefore intensifying health education by the Ministry of Health, Ghana Health Service and other stake holders such as the media among others could go a long way in increasing awareness of the importance of iodized salt and also improving compliance to the law as suggested by some key informants in this study.The generally high cost of iodized salt cannot be overemphasized. Yamada et al. (1998) asserted that, iodized salt costs more than common salt because of the additional processing cost involved in fortifying common salt with iodine [30]. High cost of iodized salt as indicated by respondents in both the quantitative and qualitative surveys is the main reason for the low use of iodized salt in this setting. This finding was supported by a research carried out in 2006 by world vision international in Walewale in the northern region of Ghana where non-iodized salt was two to ten times cheaper in some rural areas and preferred to iodized salt [31]. Similarly in southern Ghana, the low cost of non-iodized salt as compared to iodized salt influenced the decision to consume common (non-iodized) salt among some non-users and occasional users of both iodized and common salt [7].Although Ghana has passed a law on salt iodization, the absence of strict enforcement of this law and ineffective monitoring could serve as one of the main drawbacks for Ghana achieving the ninety per cent (90%) household usage of iodated salt goal by 2015. In this study, one of the main reasons given for the low household usage of iodized salt was non compliance to the law mainly due to failure to arrest those violating this law. A UNICEF study in 2012 [29] also identified weak enforcement of the law and limited availability of potassium iodide amongst others as being responsible for the inadequate usage of iodized salt in Ghanaian households. These findings were consistent with those of our study where non-availability of iodized salt in the market and non-compliance to the law resulting from the lack of its enforcement were identified as some of the reasons responsible for the low use of iodized salt in households. Adapting this mixed methodological approach has maximized the strengths and minimized the weaknesses of each of the research designs employed in this study.
5. Conclusions
- Iodized salt coverage and use in households was approximately 20% with 46.5% of household cooks not receiving any form of education at all on iodized salt. The survey revealed that knowledge levels about the existence of the law on salt iodization were very low. Some of the reasons accounting for the low use of iodized salt in households included; the high cost of iodized salt, non-availability of iodized salt, not received any education on the importance of iodized salt and ignorance of the law on iodization of salt amongst others.
6. Recommendations and Suggestions for Further Study
- Based on the findings of this survey, we recommend that Ministry of Health, Ghana Health Service and other stake holders such as the media should embark on a massive educational campaign in the district with much focus on women and those with no formal education in other to increase the awareness of the importance of iodized salt and also improve on compliance to the law. Regular and routine monitoring by the District Health Management Team, District Assembly and the Food and Drugs Board in conjunction with the Ghana police service should be conducted to ensure that salt sellers sell only iodized salt and those found selling non-iodized salt are arrested and prosecuted. This will go a long way in ensuring compliance to the law. The Food and Drugs Board at the national level should ensure that all salt producers iodized their salt before they are released into the open market. Since iodine deficiency is a public health concern, the government could support local salt producers to have their salt iodized and thereby helping to regulate the price. This will invariably lead to low cost of iodized salt being sold in the market.We suggest that further studies are conducted to assess the iodine status in the most vulnerable groups of iodine deficiency disorders such as school children and pregnant women in particular, using the determination of Urinary Iodine Concentration (UIC) levels as recommended by the WHO.
ACKNOWLEDGEMENTS
- Our profound gratitude goes to Mr Geoffrey A. Ayambire and Mr. Emmanuel Enyonam Zeye who were actively involved in the field activities. The authors are very grateful to all households’ cooks and women who took part in the focus group discussions. We are also grateful to the representatives from the District Assembly, Ghana Health Service, Foods and Drugs Board, Ghana Standards Board and the Ghana Police Service. The authors are equally grateful to the district nutrition and disease control officers of the Gushegu district.