-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Food and Public Health
p-ISSN: 2162-9412 e-ISSN: 2162-8440
2014; 4(3): 93-98
doi:10.5923/j.fph.20140403.04
Complementary Feeding Practices among Mothers of Children under Five Years of Age in Satellite Town, Lagos, Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLOlatona F. A. 1, Odozi M. A. 1, Amu E. O. 2
1Department of Community Health and Primary Care, College of Medicine, University of Lagos, Nigeria
2Department of Epidemiology and Community Health, Ekiti State University, Ado-Ekiti, Ekiti State, Nigeria
Correspondence to: Olatona F. A. , Department of Community Health and Primary Care, College of Medicine, University of Lagos, Nigeria.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
In Nigeria, only 30 percent of infants ages 6-23 months are fed in accordance with the recommendation for infant and young children feeding practices despite the fact that it has been shown that complementary feeding is one of the most important preventive measures that would reduce the excess mortality for children under the age of five years. This study determined the complementary feeding practices, among mothers of children under the age of five years in satellite town, Lagos. It was a descriptive cross sectional study which employed a multistage sampling method to select 358 mothers whose last confinement was not more than five years to prevent recall bias. Data was collected using structured interviewer-administered questionnaires and analyzed using Epi-Info version 6 computer software. Most of the respondents (65.0%, n= 227) have completed tertiary while only 1.2 % (n = 3) had no formal education. Less than half of the respondents (48.4%) introduced drinks or foods at age 6months. Even though majority (91.9%) continued breast feeding after introducing other foods, more than half (57.1%) discontinued it before 12 months. Twenty four hours dietary recall revealed that the commonest food given was cereals (65.9%) followed by fruits (46.4%) and tubers (42.7%). Most of the respondents fed the child responsively (70.3%) and prepared foods hygienically (75.1%). Complementary feeding practices though better than in many other communities within and outside Nigeria were inadequate compared to the recommended standards. Complementary feeding education using various media especially health facilities is very important for mothers of infants.
Keywords: Complementary feeding, Practices, Mothers of under-five, Nigeria
Cite this paper: Olatona F. A. , Odozi M. A. , Amu E. O. , Complementary Feeding Practices among Mothers of Children under Five Years of Age in Satellite Town, Lagos, Nigeria, Food and Public Health, Vol. 4 No. 3, 2014, pp. 93-98. doi: 10.5923/j.fph.20140403.04.
1. Introduction
- In Nigeria, under-nutrition remains a public health problem. According to the 2008 National Demographic and Health Survey, 23% of children are underweight, 14% are wasted and 41% are stunted [1]. The development of children’s full human potential depends on adequate nutrition during infancy and early childhood. Exclusive breastfeeding is adequate for the first six months of life but timely introduction of nutritionally-adequate, safe, age-appropriate complementary feeding at sixth month of age is recommended for better health and development of infants [2]. The World Health Organization recommends that breastfeeding should continue with appropriate complementary feeding from 6 months to 2 years and beyond [3].According to the Nigeria Demographic and Health Survey 2008, only 30 percent of infants aged 6-23 months and living are fed in accordance with the recommendation for infant and young children feeding practices [1]. Problems associated with complementary feeding in particular include poorly timed introduction of complementary foods (too early or too late), bottle-feeding, infrequent feeding, unsupervised feeding, poor feeding methods, poor hygiene, and child care practices [4, 5].Malnutrition is responsible for more than 41% of the deaths that occur annually in children from 6 to 24 months of age in developing countries which total approximately 2.3 million [6]. Moreover, one third of deaths among children under five years of age are attributable to nutrition and well above two thirds of these deaths, often associated with inappropriate feeding practices, occur during the first year of life [6]. Inadequate feeding of girls affects nutrient stores, leading to poor obstetrics outcome when they are having children later in life. Other consequences include growth failure and stunting, delayed sexual development, reduced muscle mass and strength, impaired intellectual development, weakened immune system, poor cognitive performance and learning achievement and increased lifetime risk of osteoporosis [7]. Every year, more than 200 million children under five years old fail to reach their full cognitive and social potential [6]. Most of these children live in South Asia and sub-Saharan Africa [6].Among preventive measures that would reduce the excess mortality for children under the age of five years, exclusive breast feeding and good quality complementary feeding have been listed as first and third, respectively, with a calculated 600,000 deaths per year preventable by good complementary feeding (i.e. 6% of deaths) [8]. Growth faltering occurs mainly in the first two years of life because of high nutritional needs for growth and development between 6-24 months [9]. In fact, the percentage of children who are underweight almost doubles from 14% among children less than 6 months of age to 26% among children age 12-17 because complementary foods are introduced to children in the latter group, thus increasing exposure to infections and susceptibility to illness [1].In Delta State, Nigeria, a little above half (54.0%) of nursing mothers feed their infants with complementary foods three times daily, and 2.4% and 37.3% feed their infants using their hand and feeding bottle respectively.[10] In Osun State, many women (48.8%) terminate breast feeding because they feel children were old enough at age 12 months. Children are fed only when they are hungry (49.9%) and 89.2% used feeding bottle for feeding [11]. In some parts of Nigeria, complementary foods are introduced to majority of children much earlier at third month (41.2%) and some others at 1-2 months (17.8%) compared with the 6th month recommended [12].However, little is known about complementary feeding practices among urban dwellers in Lagos, Nigeria. This study determined the complementary feeding practices among mothers of under-five in an urban area of Lagos State. The result will be useful for health educators to identify areas of focus for health education when educating the masses and policy makers in establishment and implementation of effective policies.
2. Methods
- A cross-sectional descriptive study was conducted among mothers of children under-five years of age in Satellite town, Lagos. The minimum sample size calculated using prevalence of appropriate infant and young child feeding practices in Nigeria, (30%) was 332 [1], however 358 mothers were selected for the study to make up for attrition and improperly completed questionnaire, using multi-stage sampling technique. In Satellite town there are seventy five (75) closes, fifteen (15) company owned estates, ten (10) privately owned estates and fifty (50) streets. Using the systematic sampling method with a sampling interval of five (5), every 5th close was selected out of the seventy five (75) closes. Fifteen (15) closes were therefore selected. Balloting was done to pick one between the two ends of each close to determine the starting point. One mother was interviewed from each household. All eligible mothers in the households in each close were interviewed until six (6) mothers were interviewed in each close to obtain ninety (90) respondents from the closes. Two (2) streets were selected out of the fifty (50) streets using the balloting method. The average number of houses on each street was one hundred (100). Using the systematic random sampling with a sampling interval of two (2), every second (2nd) house was selected on each street to get fifty (50) houses. One (1) household was selected from each house using balloting method, to obtain fifty respondents from each street and therefore a total of one hundred respondents (100) from the streets section. One (1) estate each from the company owned and privately owned estate was selected through balloting. Two (2) estates were therefore selected. The households in the estates did not have a systematic arrangement so all eligible mothers were interviewed until eighty five (85) mothers were interviewed in each estate to obtain one hundred and seventy (170) respondents from the estate section. A mother and child were included in the study if the youngest child was at least one year and less than 5 years of age. The youngest child was taken as the index child and all the responses obtained were based on this child. If more than one mother who met the inclusion criteria was seen in a household, one (1) mother was selected by the balloting technique.
|
|

|
|
- Data was collected in May 2013, using a pre-tested structured interviewer administered questionnaire. The questionnaire contained questions on complementary feeding practices. Four interviewers (secondary school leavers) were trained on how to administer the questionnaires correctly. If the interviewers didn’t meet an eligible woman in the house at the time of visit, then they went back at a later time in the evening or at a later date. The completed questionnaires were inputted and analysed using Epi Info Statistical software (version 3.5.1).Ethical approval was obtained from the Health Research and Ethics Committee of Lagos University Teaching Hospital and permission to conduct the research was obtained from the Local Council Development Area. Informed written consent was obtained from each respondent before administering the questionnaire. Utmost confidentiality of information obtained was ensured.
3. Results and Discussion
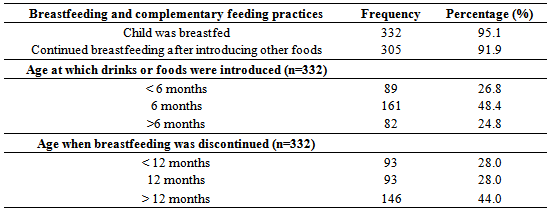
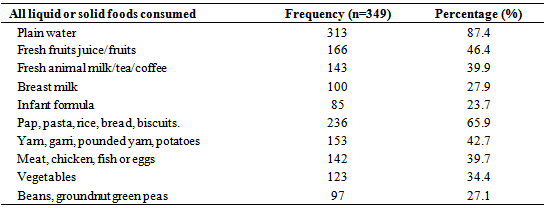
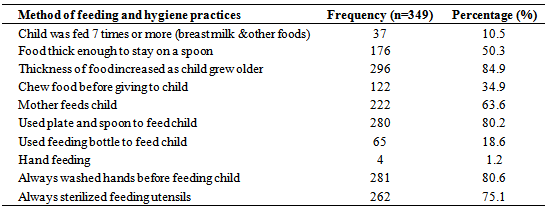
- Most of the respondents (65.0%, n= 227) have completed tertiary while only 1.2% (n = 3) had no formal education. Almost all the respondents (95.1%) breastfed their children. This is similar to the findings of a study conducted in Mauritius in which 93.4% of the respondents breast fed their babies [13]. This probably means that most of the mothers in this community have embraced baby friendly initiative. Almost half of the respondents (48.4%) introduced drinks or foods at age 6 months. The proportion who introduced complementary feeding at the age of 6 months is lower than that reported among mothers of under two children in Kassena-Nanka region of Ghana (61.2%) but slightly higher than the 37.6% reported in Brong Ahafo region in Ghana and 33.5% reported in South-West Nigeria [11, 14, 15]. It however contrasts with that reported in India where only 13% of the respondents had introduced complementary feeds at 6 months [16]. The higher responses reported in this and the Kassena-Nanka region of Ghana studies can be explained by the higher educational levels of the respondents and better access to information than those in the other studies. Only about a quarter (26.8%) of the respondents in this study introduced complementary foods before the age of 6 months. This contrasts with the results obtained from some studies conducted in Gaza Strip, South-South, North-West and South-West regions of Nigeria where 79.9, 79.0 and 80.1 and 53.0% respectively introduced complementary feeding before the expected 6 months of age [10, 11, 12, 17]. The mothers in this study were probably more exposed to infant feeding education and knew the danger of introducing meals before six months of age. Introduction of feeds before 6 months is fraught with the dangers of infections, allergies, digestive problems and obesity later in life and therefore should be discouraged [7, 18].About a quarter, (24.8%) of the respondents equally introduced complementary foods after the age of 6 months which contrasts with that of a study conducted in India in which 63% of the respondents introduced complementary foods after 6 months [16]. After six months, breast milk is no longer sufficient to meet the nutritional requirements of an infant. Late introduction of complementary feeds leads to growth faltering which can predispose to overt malnutrition especially when associated with recurrent infections which are common about this stage [9].A large percentage (91.9%) continued breast feeding after introducing other foods but well over half (56.1%) of them equally discontinued before or at 12 months; while only 43.9% discontinued after 12 months. The Kassena-Nanka Ghanaian study reported similar findings with 96.3% continuing breast feeding after introducing complementary feeds [14]. It is recommended that breast feeding should continue after introducing complementary feeds until child is two years old. This will give the necessary nutritional support while the child gradually gets accustomed to eating solid food [19]. Most of the respondents (70.3%) fed their children responsively while others fed their children at scheduled times or during family meal times. Responsive feeding is advocated by WHO and UNICEF as the best approach to ensure that infants are appropriately fed and has been shown to be associated with better mental development compared to traditional complementary feeding [7, 20].As convenient as scheduled meal times may be, they might not coincide with the period of hunger in the infants, such that they might either refuse to eat, or take less or more than what they would ordinarily have eaten. Baby-led approach in complementary feeding may encourage greater satiety-responsiveness and healthy weight-gain in infants [21].The World Health Organization (WHO) recommends certain age-specific frequencies of complementary feeding based on theoretical estimates of the energy provided by complementary foods. Infants should be fed initially 2-3 times a day between 6-8 months, increasing to 3-4 times daily between 9-11 months and 12-24 months with additional nutritious snacks offered 1-2 times per day, as desired [1]. In this study, only 37.3, 49.7 and 51.2% of the infants were fed according to these requirements at age 6-8, 9-11 and 12-24 months respectively. Some studies conducted in Nigeria, India and Ghana similarly reported that the mothers did not know the appropriate age-specific frequency of feeding with complementary foods as stipulated by the WHO [10, 15, 16]. Most of them just fed their children as frequently as it seemed appropriate to them irrespective of the ages of the infants. This underscores the need for regular nutrition education at various contact points where the mothers can be reached. Feeding less than the required number of times can lead to under-nutrition while feeding more than the recommended number of times can lead to over nutrition and later on obesity. The twenty four hours (24 hours) dietary recall revealed that majority of the respondents gave cereal (65.9%) followed by fruits (46.4%) and then tubers (42.7%). Animal proteins in form of (meat fish or eggs) and vegetables were given by few people. A study conducted among children in Northern Uganda similarly reported that majority of the respondents (35.2%) were given cereals in the last 24 hours. However, the proportion that gave fruits and vegetables (31.1%) and beans (22.4%) was lower. The proportion that gave meat and milk /milk products were even much lower than that of the present study (1.8 and 0.5%) respectively. [22] Cereal based foods alone are not sufficient; in order to prevent micronutrient deficiencies, milk, meat products, legumes, fruits and vegetables should be integral parts of the complementary foods of children. Breast feeding should also be continued up till two years in order to further support their growth [6]. Only 10.5% of respondents fed their children more than 7 times as expected. This may be as a result of ignorance about this recommendation or because the parents could not afford to feed the infants more than seven times per day. This is similar to the report of a study conducted among returnee children in Northern Uganda in which majority of the children were fed only twice irrespective of their ages, in the 24 hours preceding the survey [22]. Majority of the children were fed by the mothers (63.6%). Mothers are better at practicing responsive feeding than other care givers some of which might be the older siblings. In responsive feeding the mother responds to the child’s hunger and satiety cues, interacts with the child, experiments with different food combinations, tastes, textures, and methods of encouragement in case the child refuses many foods, and minimizes distractions during feeding. All these skills help to ensure that the child takes enough especially when ill [8, 23].Only half of the respondents (50.3%) made the complementary food to be of the right consistency though majority (84.9%) increased the thickness as the children grew older. In the Brong Ahafo region study in Ghana however, only about one-third of caregivers reportedly gave thick, nutrient dense foods to children after 6 months of age while only 33.2% of them increased the thickness as the children grew older [15]. It is recommended that at the beginning of complementary feeding, foods should be semi-solid and soft (in the form of a puree) and should be crushed or mashed, never sifted or blended [24]. The consistency should then be gradually improved, considering the infant’s eating skills and age. It should be noted that improper food consistency compromises the appropriate intake of nutrients by the infant [3].About four-fifth of the respondents always washed their hands before feeding their children while three-quarters of them always sterilized their feeding utensils. This contrasts with the report of a study conducted in Northern Nigeria in which only 28% of the respondents always washed their hands before feeding the children and only 19% always sterilized the feeding utensils [12]. The respondents in this study were more hygienic compared with their Northern counterparts. The fact that most of the mothers had tertiary education, higher socio-economic statuses and better access to amenities such as water and electricity compared to their counterparts in the North can explain the difference. It is expected that clean utensils be used to feed children in order to avoid introducing dirt and germs that might cause diarrhoea and other infections [24].
4. Conclusions
- Less than half of the respondents (48.4%) introduced other drinks or foods at age 6 months. Even though majority (91.9%) continued breast feeding after introducing other foods, more than half (57.1%) discontinued it before 12 months. Complementary feeding practices in this study though better than in many other communities within and outside Nigeria were inadequate compared to the recommended standards. WHO guidelines on complementary feeding, should be communicated using various media to mothers of infants. Moreover, government should encourage female education so that more mothers will be educated and empowered to practice adequate and safe complementary feeding.
Conflict of Interest
- We, the authors of this manuscript declare that there is no conflict of interest that might bias our work or inappropriately influence our judgment.