-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Food and Public Health
p-ISSN: 2162-9412 e-ISSN: 2162-8440
2013; 3(6): 284-288
doi:10.5923/j.fph.20130306.04
Nasal Carriage of Enterotoxigenic Staphylococcus aureus and Risk Factors among Food Handlers-Egypt
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMoustafa El-Shenawy1, Lobna El-Hosseiny2, Mohamed Tawfeek1, Mohamed El-Shenawy3, Hoda Baghdadi2, Ola Saleh1, J. Mañes4, J. M. Soriano4
1Department of Food Microbiology, National Research Center, Dokki, Cairo, 12311, Egypt
2Department of Environmental Studies, Institute of Graduate Studies and Research, Alexandria University, Egypt
3Department of Microbiology, National Institute of Oceanography and Fisheries, Alexandria, Egypt
4Observatory of Nutrition and Food Safety in Developing Countries, Department of Preventive Medicine and Public Health, Faculty of Pharmacy, University of Valencia, Burjassot, 46100, Spain
Correspondence to: Moustafa El-Shenawy, Department of Food Microbiology, National Research Center, Dokki, Cairo, 12311, Egypt.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
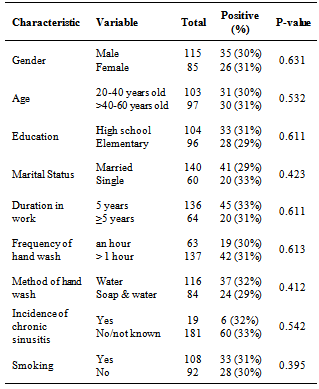
Food handlers play a major role in the transmission of food borne diseases which represents a global health burden. Carriage of Staphylococcus aureus, in general, and enterotoxigenic strains, in particular, is an important risk factor for the contamination of food. This study was undertaken to determine the prevalence and risk factors associated with nasal carriage of Staphylococcus aureus among 200 food handlers working in 3 different food processing plants in Egypt. Sixty-one (31%) persons were found to be carriers of Staphylococcus aureus of which twenty-one (34.4%) harboured enterotoxigenic staphylococcal strains. The most frequently found enterotoxins were Types A and C (12 isolates each), followed by Type B and Type D (7 isolates, 5 isolates) respectively. A combination of two or three enterotoxins was produced by some of the isolates. The three processing plants recorded statistically significant differences amongst examined personnel in nasal carriage, however neither of the risk factors assessed including age, gender, marital status, education, duration in work, frequency and method of hand wash, incidence of chronic sinusitis and smoking were significant risk determinants of S. aureus nasal carriage. The obtained results should be of public health concern and highlights the need for primary health care and hygiene among food handlers.
Keywords: Enterotoxigenic S. Aureus, Nasal Carriage, Risk Factors, Food Handlers
Cite this paper: Moustafa El-Shenawy, Lobna El-Hosseiny, Mohamed Tawfeek, Mohamed El-Shenawy, Hoda Baghdadi, Ola Saleh, J. Mañes, J. M. Soriano, Nasal Carriage of Enterotoxigenic Staphylococcus aureus and Risk Factors among Food Handlers-Egypt, Food and Public Health, Vol. 3 No. 6, 2013, pp. 284-288. doi: 10.5923/j.fph.20130306.04.
Article Outline
1. Introduction
- According to the World Health Organization (WHO), up to 30% of the populations of developed countries are affected by food-borne illness each year. The problem is more widespread in developing countries where most of these cases are not reported, and thus the true dimension of the problem is not known[1]. In these countries, errors made in food processing plants and settlements emerge as important causes of foodborne disease[2].Food handlers are potential causes of infections by many food borne pathogens since many diseases arecommunicable and caused originally by microorganisms carried into their bodies[3]. It is estimated that 30-50% of the human population carries Staphylococcus aureus and its main habitat is the nasopharynx, a site where strains can persist as transitory or persistent members of the normal microbiota without causing any symptomatology. Accordingly, body carriage of S. aureus by food handlers can be an important source of contamination of the food product via respiratory secretions or direct contact via hands during manufacture and handling of the food product[4]. Staphylococcus aureus is an extraordinary versatile pathogen and the major causative agent of numerous infectious diseases. The disease spectrum includes abscesses, septicemia, endocarditis, osteomyeltis, pneumonia, in addition to various toxin mediated diseases as toxic shock syndrome and staphylococcal food poisoning. The variety of such spectrum of clinical manifestations is mostly dependant on the numerous virulence factors produced by each strain[5]. The ingestion of the preformed toxins produced by enterotoxigenic strains in food often leads to the development of food poisoning. The symptoms typically have a rapid onset (2–6 h) and may include nausea, vomiting, diarrhea and abdominal pain[6]. Consequently, the rising concerns over food safety and the lack of research into the proportion of Egyptian food handlers colonized by S. aureus have formed the impetus for investigation of the incidence and potential risk factors associated with nasal carriage of S. aureus amongst personnel working in three different food processing plants.
2. Materials and Methods
- This work was done over a period of 10 months (Jan. 2012-Nov.2012). Two-hundred food handlers, working in three different food processing plants, participated in this work. These include 42 personnel working in milk and dairy products plant, 67 working in meat and poultry products plants and 91 working in frozen/canned juices and vegetables processing plant. Prior to sample collection a demographic data sheet was collected from each participant.The Staphylococcus spp. nasal carriage study was carried out using sterile swabs, which were inserted in both anterior nares and transferred to a tube containing sterile brain heart infusion broth. Tubes were incubated at 37℃ for 24 h, streaked onto the surface of Baird-Parker Agar Base plates (Oxoid CM0275, Basinggstoke, Hants, UK) supplemented with egg-yolk tellurite emulsion (Oxoid SR 0054) and aerobically incubated at 37℃ for 24-48 h. Three colonies per sample, showing typical colonial morphology of coagulase- positive Staphylococci, were subjected to Gram staining, coagulase and catalyse tests. Gram, coagulase and catalyse positive strains were confirmed with an agglutination Staphyloccci Plus test (Oxoid) thereafter biochemically identified with API staph identification System for Staphylococcus aureus (bioMerieux Marcy – I'Etoile, France). Definitive identification was based on the presence of DNA using DN-ase test, the presence of protein A and clumping factor using SLIDEX Staph plus (bioMerieux Marcy – I'Etoile, France). A strain of S. aureus NCTC 10788 (obtained from food science department, University of Wisconsin-Madison, US) was used as a reference strain. Only one identified isolate per positive samples was investigated using an immunological technique to verify its ability to synthesize staphylococcal enterotoxins. The strains were grown in 10 ml of tryptone soya broth (CM0219B, Oxoid) by shaking aerobically for 16-18 h at 37℃. After centrifugation at 9000 x g for 20 min at 4℃, the supernatant was tested for presence of staphylococcal enterotoxins and typed using Staphylococcal Enterotoxin Test Reversed Passive Latex Agglutination (SET-RPLA) (TD900 Oxoid Basinkstoke, Hampshire, UK) as recommended by the manufacturer's protocol. Negative controls were used with all the tested samples. Data collected were statistically analysed using SAS version 8 (SAS Institute, Cary, NC, US). Proportions were compared using Pearson Chi-Square tests. The level of statistical significance was set at a P-value ≤ 0.05.
3. Results and Discussion
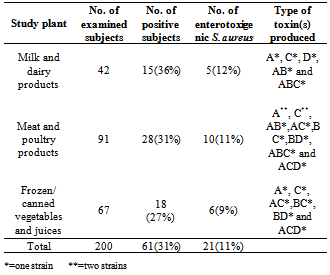
- Table (1) illustrates the number of persons screened for nasal carriage of S. aureus in the investigated food processing plants. The overall prevalence of the pathogen in the two hundred examined personnel was about one third (31%). Subjects working in the milk and dairy processing plant recorded the highest prevalence rate (36%) of colonization by S. aureus followed by the other two processing plants; meat and meat products (31%) and frozen/canned vegetables and juices (27%) plants respectively. The difference in prevalence rates amongst the three study plants were significant (P = -0.028), however this prevalence cannot be exactly compared due to differences in sample size, habits and other environmental conditions that may exist in these plants.
|
|
4. Conclusions
- In conclusion, a relatively high prevalence rate of S. aureus nasal carriage was recorded among the investigated food handlers. Moreover, 11% of the investigated carriers harboured enterotoxigenic strains in their anterior nares increasing the likelihood of transmission of the pathogen to the handled food. These findings resurges the imperative need for protective measures including increased public awareness programs, regular monitoring of food handlers for food borne pathogens and intensive training on primary health care and hygiene. Finally, the current findings clearly highlight the significance of implementation of efficient quality control systems in areas of direct contact with food product as good manufacturing practices and standard operational procedures and future research addressing effective methods for sustained eradication of staphylococcal nasal carriage are clearly warranted to reduce the high risk of subsequent infection.
ACKNOWLEDGEMENTS
- Financial support for this research was provided by the Agencia Espa˜nola de Cooperaci ´on Internacional para el Desarrollo (A/019106/08, A/025113/09 and A1/035779/11).