-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Food and Public Health
p-ISSN: 2162-9412 e-ISSN: 2162-8440
2013; 3(4): 191-194
doi:10.5923/j.fph.20130304.03
Health Status, Blood Pressure and Physical Activity Pattern of Undergraduates in South West Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLS. Nupo Sedodo1, J. Akinlotan Victoria1, P. Olunusi Abosede2
1Food Technology Department Moshood Abiola Polytechnic Ojere Abeokuta
2Tai Solarin University of Education Ijagun Ijebu Ogun state. Home Economics Department
Correspondence to: S. Nupo Sedodo, Food Technology Department Moshood Abiola Polytechnic Ojere Abeokuta.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
This study was carried out to assess the Health status, blood pressure and physical activity pattern of undergraduates in South West Nigeria.. A representative sample of two thousand (2000) undergraduate students was surveyed from two Nigerian Polytechnics using simple random technique. A pretested interview guide was used to collect information. Waist to Hip Ratio (WHR) was calculated from anthropometric measurements and used to classify subjects’ nutritional status. The blood pressures of the subjects were measured using sphgmanometer. Physical activity and energy expenditure was computed and compared with the energy expenditure classification of lifestyles based on Physical activities level (PAL) as described by FAO/WHO/UNU (1). Data were analyzed using descriptive statistics; SPSS software package version 16.0.The result of the WHR showed that 71% of the subjects had normal nutritional status, 8% of the female were overweight while 8% of the male students were obese. Blood pressure measurements revealed that 40% of the subjects were at pre hypertension stage, 11% had stage 1 hypertension while 7% had stage 2 hypertension. The subjects had low physical activity pattern.
Keywords: Health Status, Hypertension, Anthropometric Measurements, Undergraduates
Cite this paper: S. Nupo Sedodo, J. Akinlotan Victoria, P. Olunusi Abosede, Health Status, Blood Pressure and Physical Activity Pattern of Undergraduates in South West Nigeria, Food and Public Health, Vol. 3 No. 4, 2013, pp. 191-194. doi: 10.5923/j.fph.20130304.03.
Article Outline
1. Introduction
- Obesity which is defined as a condition of abnormal or excessive fat accumulation in adipose tissue, to the extent that health is impaired (2) in absolute terms, and its distribution in the body - either around the waist and trunk (abdominal, central or android obesity) or peripherally around the body (gynoid obesity) - has important health implications. A central distribution of body fat is associated with a higher risk of morbidity and mortality than a more peripheral distribution (3). Excess body weight is the sixth most important risk factor contributing to the overall burden of disease world wide (4). Obesity is a common public health problem in most of the developed and developing world today in that it is linked directly with several chronic disease processes. These diseases include hypertension, cardiovascular diseases, type 2 diabetes mellitus, cancer and many other diseases. Obesity is also known to reduce life expectancy (5).The relevance of obesity and hypertension as an important public health challenge is increasing worldwide (6). The growing prevalence of obesity is increasingly recognized as one of the most important factors for the development of hypertension. Obesity combined with hypertension is associated with cardiovascular risk (7). The precise mechanism linking obesity to hypertension, increased cardiovascular risk and many chronic diseases are not fully understood. However, factors derived from adipose tissues are believed to play a major role. According to Wiecek et al.(8) adipose tissue may elaborate angiotensio secretion from its own local rennin-angiotensio system. Also Aneja et al.(9) highlighted that adipose tissue is not merely an interactive organ for storage of energy but it also secretes a host of factors which interact with each other and may result in development of increased blood pressure. According to Rahmoni et al.(10) obesity per se may also have structural effects on the kidneys which may perpetuate hypertension.Maintaining ideal body weight, decreasing sedentary lifestyle and provision of high- quality health-care services have been emphasized to effectively reduce the risk of adverse clinical outcomes of hypertension (11). Thus assessment of the nutritional status of patients with hypertension to detect and treat overweight and obesity was emphasized as a crucial therapeutic measure of hypertension (10). High blood pressure in adults has a high impact on the economy and on the quality of life of individuals with important implications for resource expenditures. A number of studies revealing the prevalence of hypertension in populations of West African origin have been reported (12). Not much has been done to determine the magnitude and epidemiological characteristics on undergraduates in Nigeria. Effective interventions will prevent increase of the cardiovascular risk factors and raise first alarm of the condition which can help to monitor, control and provide palliative measures of the burden of hypertension among the undergraduates’ students. To this end, a cross-sectional survey was carried out to estimate the health status, blood pressure, nutrient intake and physical activity pattern of undergraduates in South West Nigeria
2. Materials and Methods
- A cross sectional study was carried out in Ogun state and Lagos state, South west Nigeria. A structured pretested questionnaire was used to randomly select two thousand undergraduate students from Moshood Abiola Polytechnic and Lagos state Polytechnic. The questionnaire form was adapted from FANTA (13).
2.1. Blood Pressure
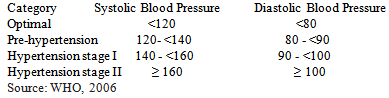
- Blood pressure of the subjects was measured with OMRON digital automatic blood pressuresphygmomanometer (Model HEM-712C). The blood pressure was measured on the left arm after the subjects have rested for 5 minutes in a seated position. The blood pressure reading was taken, the higher number represents the systolic pressure (the pressure at the peak of each heart beat) and the lower number represents the diastolic pressure (the pressure when the heart is resting between beat). The systolic blood pressure (SBP) and diastolic blood pressures (DBP) was recorded to the nearest 2mm Hg. The values of SBP and DBP were related to the reference standard (14). The World Health Organization (15) criteria for classifying blood pressure measurement were adopted to determine the rate of the various categories of hypertension both systolic and diastolic among respondents. The definition of the categories of hypertension adopted by WHO are as follows:
2.2. Waist-Hip Circumference
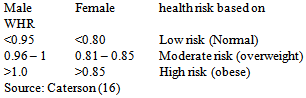
- Subjects waist to hip ratio was determined using the protocol described by Caterson, (16). The measurement was taken to the nearest 0.1cm.Waist Hip Ratio of the subject was be expressed as the

2.3. Waist Hip Ratio Classification
- The Waist – Hip Ratio of the subject based on their sex and age was classified as
2.4. Physical Activities Pattern
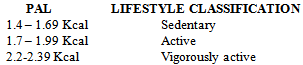
- Each subjects’ daily activity pattern was recorded through the use of questionnaire with a recall method (1). This involved the pattern of activities right from the time they wake up till bedtime at night. The energy expended on each activity was calculated using FAO/WHO/UNU (1) table of energy expenditure. This was carried out on three occasionsThese were computed and compared with the energy expenditure classification of lifestyles based on Physical activities level (PAL) as described by FAO/WHO/UNU (1)
 Waist – Hip Ratio and Mid Upper Arm Circumference of the Subjects
Waist – Hip Ratio and Mid Upper Arm Circumference of the Subjects3. Results
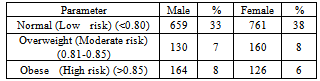
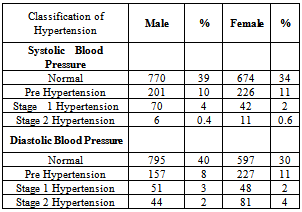
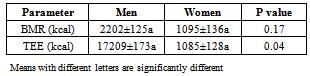
- Table 1 presents the waist to hip ratio and mid upper arm circumference of the subjects. The results show that most (71%) of the subjects had normal waist to hip ratio and were at low risk of malnutrition, out of which 38% were female, fifteen percent (15%) were overweight and were at moderate risk of malnutrition out of which 8% were female , 10% of the female were obese and had high risk of malnutrition.Table 2 shows the prevalence of hypertension among the subjects. A higher proportion (73%) of the subjects had normal systolic blood pressure, of which 39% were male, 10% of male and 11% of female were at the stage of systolic pre hypertension, 4% of male had Stage 1 hypertension while 2% of female students also had Stage 1 Hypertension. Only 1% had Stage 2 hypertension Most of the subjects (70%) had normal diastolic blood pressure out of which 40% were male. Moreover, few (19%) of the subjects had diastolic pre hypertension, 5% had stage 1 diastolic hypertension while 6% had stage 2 diastolic hypertension.Table 3 presents the mean of energy expenditure of the subjects. The mean of the Basal metabolic rate (BMR) were 2202±125a and 1095±136a kcal for male and female respectively. The total energy expenditure for male was 17209±173a kcal while for female it was 1085±128a kcal; male had higher energy expenditure than female (P< 0.05). The physical activity level for male was 1.61±2.31a while female had 1.67±0.2.
|
|
|
4. Discussion
- The present study examined the health status, blood pressure, nutrient intake and physical activity pattern of undergraduates in South West Nigeria. The results of the Waist – Hip Ratio of the Subjects showed that 15% of the subjects were overweight while 14% were obese. Obesity was higher in male student than female as observed in the study.This finding supports the observation of other authors who reported higher percentage of obesity among male students than female (17, 18, 19 ). The study revealed that most of the subjects had normal blood pressure. Regulation of normal blood pressure is a function of cardiac out put and peripheral vascular resistance; these variables are influenced by multiple factors such as excessive dietary energy, salt intake and sedentary lifestyle. All these factors may interact to produce hypertension and limit its controls [20). However, few of the subjects had hypertension. There are inconsistent reports on the prevalence of hypertension in Nigeria among adult population, a survey of cardio vascular risk factors in Nigeria conducted 15 years earlier reported the age-adjusted prevalence of hypertension to be 11.2%, using a qualifying BP level of 160/95 mmHg [21]. Using the same qualifying BP level, other workers found the prevalence ofhypertension to be 12.4% in south western Nigeria[22]. Extrapolations from the Non Communicable Diseases data and from other studies suggest an urban prevalence rate of around 20% using the current cut-off point of 140/90 mmHg [12, 23]. In a survey of cardiovascular risk factors in middle aged Nigerians aged 50-54 years, hypertension was found in 25% of males and 16.4% of females [24]. The prevalence of hypertension among the undergraduate students was 19%. The level of the prevalence obtained in our study was higher than what other researchers reported in other part of West African [25,26]. However the overall prevalence of hypertension in this study was an indication that hypertension rate is gradually becoming a burden among the undergraduates.This study had identified prevalence of pre- hypertension (BP < 130/85mmHg) among the study population. This risk factor will probably increase the burden of cardiovascular disease in the near future in the South West Nigeria if primordial and primary prevention are not instituted early enough. These observations have been reported among adult population in India and Indonesia [27]. The physical activity pattern among the undergraduate was low, likewise the total energy expenditure. This observation could be due to their rigorous academic activity of the period during which the data was collected.
5. Conclusions and Recommendations
- There exist a few double burden of malnutrition among the undergraduates and onset of cardiovascular risk factors. In the study, it was discovered that overweight and obesity is high among the study population especially the male students. Only a small percentage of the subjects had hypertension. The physical activity pattern and energy expenditure of the subjects were low. There is need for nutritional education and medical intervention.

