-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Food and Public Health
p-ISSN: 2162-9412 e-ISSN: 2162-8440
2013; 3(3): 147-153
doi:10.5923/j.fph.20130303.06
The Synergistic Effect of Taurine and Caffeine on Platelet Activity and Hemostatic Function
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbishek B. Santhakumar, Nicolette Fozzard, Anthony V Perkins, Indu Singh
School of Medical Science, Gold Coast Campus, Griffith University, Queensland, 4222, Australia
Correspondence to: Indu Singh, School of Medical Science, Gold Coast Campus, Griffith University, Queensland, 4222, Australia.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Several studies have shown the deleterious effects of energy drinks, containing taurine and caffeine, on cardiac health. This study aimed to examine synergistic effect of taurine and caffeine on platelets and haemostasis because platelet hyperactivity is a known predictor of cardiovascular diseases. Blood from twelve healthy volunteers aged 18 – 60 years was incubated with 500 µM taurine and 700 µM caffeine individually or together. Platelet activity was evaluated using platelet aggregation assays induced by ADP and collagen, and, haemostatic function by coagulation profile testing, glucose, lipid profile and inflammation marker C- reactive protein assessment (CRP). The optimal time and doses of taurine and caffeine required to inhibit platelet hyperactivity in vitro were established. A combined action of lower doses of taurine and caffeine (T+C) inhibited platelet aggregation, induced by ADP and collagen, greater than taurine or caffeine individually (p < 0.05). Taurine and T+C increased prothrombin clotting time (PT) significantly (p < 0.05), while caffeine alone decreased PT (p < 0.05). Caffeine alone increased CRP (p < 0.05). No significant change was observed in lipid parameters. These data support our hypothesis that, synergistically lower concentrations of taurine and caffeine, found in much higher concentrations in energy drinks, may be instrumental in reducing platelet activity and prolongation of clot formation.
Keywords: Taurine, Caffeine, Energy Drinks, Platelet Aggregation, Cardiovascular Disease
Cite this paper: Abishek B. Santhakumar, Nicolette Fozzard, Anthony V Perkins, Indu Singh, The Synergistic Effect of Taurine and Caffeine on Platelet Activity and Hemostatic Function, Food and Public Health, Vol. 3 No. 3, 2013, pp. 147-153. doi: 10.5923/j.fph.20130303.06.
Article Outline
1. Introduction
- Energy drinks are beverages that commonly contain about 1000 mg taurine (31 mM/150 mL), 80 mg caffeine (3.4 mM/150 mL), herbal supplements and sugar or sweeteners[1]. Alarmingly, certain energy drinks available as shots contain more than 10 times the average person’s suggested daily limit of taurine and caffeine. They have been marketed to help improve athletic performance, weight loss and stamina. Though these promoted aspects of energy drinks are beneficial, several studies have emphasized on the deleterious effects of the components of energy drinks on cardiac health[2-4]. Caffeine consumption has been reported to have adverse effects on human health such as palpitations, gastrointestinal disturbances, increased blood pressure, insomnia, iron deficiency anemia, higher risk of developing osteoporosis as well as problems in metal absorption, excretion, and reabsorption processes in intestine and kidney[5-8]. It has also been reported that consumption of high concentrations of caffeine used in energy drinks has been associated with seizures, sudden cardiac arrests and strokes especially in children and young adolescents[9]. Nevertheless, caffeine consumption has been reported to enhance performance and endurance in athletes[10], increase alertness and reduce fatigue[11], potentiate postsynaptic neurotransmission in the sympathetic nervous system[12], increase secretion of gastric acid[13], and increase neuromuscular coordination[12]. The purpose of this study is to examine the underlying controversies in the use of energy drinks by evaluating the in vitro synergistic and discrete effects of taurine and caffeine on platelet and haemostatic function, using platelet aggregation, coagulation and lipid profile testing. Platelets are disc shaped cells in the blood that help in the formation of blood clots and play a critical role in cardiac arrests, peripheral vascular disease and strokes. Under normal physiological conditions platelets circulate in close contact to the endothelial lining of the blood vessel wall without adhering to them[14]. However under pathological conditions platelets rapidly respond to the alterations in the endothelial cell wall and attach themselves securely to the site of the lesion. Platelets aggregates (or thrombi) are formed and are associated with cardiovascular ischaemic events[14]. Platelet hyper-aggregation or hyper-activation is one of the known predictors of cardiovascular diseases (CVD)[15]. Hence, reducing platelet hyper-activity could prove to be an effective strategy in reducing the risk factors leading to such ischaemic events. These platelet aggregating agents or agonists as they are commonly called, induce an increase in the platelet production of Thromboxane A2 (TXA2), which amplifies aggregation response and stimulates vasoconstriction[16]. These actions favour thrombosis but are balanced under normal physiological conditions by nitric oxide (NO), prostacyclin (PGI2) and vasodilation[14]. We speculate that taurine and caffeine together may help in reducing platelet aggregation and hence may alleviate the risk of thrombus formation. Taurine (2-aminoethane sulphonic acid) is a conditionally essential amino acid, which helps in a variety of bodily functions such as, bile acid conjugation, osmoregulation, membrane stabilization, modulation of cellular calcium levels and antioxidation[17, 18]. Taurine added in vitro to platelets are known to stabilize themselves against a wide range of aggregating agents via a mechanism involving Ca2+ flux[19]. Taurine has been demonstrated to have a protective effect against the hyper-coagulative state in gestosis patients with edema, proteinuria and hypertension by inhibition of platelet aggregation[20]. Our previous study suggests that taurine as an antioxidant inhibits platelet activity and may be instrumental in reducing the risk of thrombosis[21]. Caffeine a member of the methylxanthine family, is a natural alkaloid found in coffee beans, tea leaves, cocoa beans and cola nuts[22]. Methylxanthines are non-selective adenosine receptor blockers. Adenosine receptors have been classified into 5 subtypes – A 1, A2A, A2B and A3[23]. Caffeine has been shown to most potently act on the A2A receptor, which has been identified as being specifically expressed on platelets[24, 25]. Under homeostatic conditions, the A2A receptors in platelets are sufficiently activated by adenosine in the blood. However, caffeine competitively inhibits the action of adenosine, which normally would bind the adenosine A2A receptor, thus altering the platelet function and increasing receptor activity[26]. This increased receptor activity subsequently causes an increase in cyclic adenosine monophosphate (cAMP) which acts directly to inhibit platelet aggregation[27]. Varani et al. demonstrated the up-regulation of A2A receptors by caffeine accompanied by increase in cAMP levels and inhibition of aggregation and calcium levels[28]. The effect of caffeine consumption on platelet function has also been demonstrated to be dependent on both the dose and the duration of the treatment, which subsequently reduces platelet aggregability in vivo[29]. Nevertheless, as elucidated earlier, caffeine is also known to have adverse effects on cardiac health. Since taurine’s and caffeine’s varied health effects have been a widely debated topic, it is essential to determine their combined health potential and the beneficial dosages to be used in energy drinks. The hypothesis of our study is that taurine, an antioxidant, may be able to effectively attenuate the risk of thrombosis by inhibiting platelet aggregation, and caffeine, a competitive antagonist of the adenosine A2A receptors subsequently leading to an inhibition of platelet aggregation, synergistically may be able to significantly reduce platelet and hemostatic activity, instrumental in reducing the risk of thrombosis. The aim and objective is to evaluate the synergistic and discrete effects of taurine and caffeine on platelet activity using platelet aggregation assays (stimulated by ADP and collagen); and haemostatic function by testing prothrombin time, activated partial thromboplastin time coagulation assays, lipid profile and inflammation markers.
2. Materials and Methods
- This study was performed at the School of Medical Science, Griffith University, Gold Coast campus, Queensland, Australia. The Human Research Ethics Committee, Griffith University, approved this study.
2.1. Volunteers
- Twelve healthy (6 male and 6 female) volunteers between the ages of 18 and 60 years were recruited for this study. All volunteers provided written informed consent to participate in the study. The criteria for volunteer recruitment for the study included healthy, non-smoking males or females with no history of CVD or diabetes. Volunteers were screened by means of a questionnaire, which requested information regarding the level of physical activity, medical history, diet and use of aspirin-type products, non-steroidal anti-inflammatory drugs, blood pressure and other drugs. Volunteers were also requested not to consume any polyphenol rich foods, omega-3 polyunsaturated fatty acid rich foods, alcohol, cocoa products, coffee or energy drinks. For this in vitro study, compliance was only confirmed by the volunteer’s statement on the questionnaire before they signed informed consent for phlebotomy. This study did not involve any additional dietary supplement intake.
2.2. Study Design
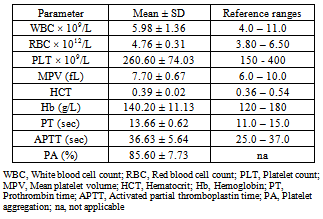
- The collected whole blood (WB) was screened for hemoglobin (Hb), hematocrit (Hct), white blood cell count (WBC), platelet count (PLT) and mean platelet volume (MPV) before analysis. Platelet Rich Plasma (PRP) and Platelet Poor Plasma (PPP) were obtained by centrifugation of WB. The obtained plasma was then used to determine platelet aggregation, coagulation profile, lipid profile and C-reactive protein (CRP) following treatment with taurine, caffeine, and taurine combined with caffeine (T+C). The optimal incubation time and dosage of taurine and caffeine to significantly stimulate platelet function in PRP was established.
2.3. Blood Collection
- A total of 24 mL of venous blood per volunteer was collected by a trained phlebotomist at the School of Medical Science, Griffith University, Australia. WB was collected into tri-potassium ethylene diamine tetra-acetic acid (EDTA) (1.8 mg/mL) tubes for full blood examination (FBE), tri-sodium citrate (3.8%) tubes for platelet aggregometry and serum separator tubes (SST) for Lipid profile and CRP testing. WB was collected into EDTA tubes before tri-sodium citrate tubes to avoid the risk of collecting platelets activated by venipuncture. Care was taken to ensure minimal specimen handling and agitation.
2.4. Full Blood Examination (FBE)
- EDTA anti-coagulated whole blood was analyzed for Hb, Hct, WBC, PLT and MPV using Beckman Coulter ACTTM 5Diff CP hematology analyzer (Coulter Corporation, Miami, Florida, USA) within 10-15 minutes of venipuncture. Prior to FBE each day, the performance of the analyzer was validated and calibrated. Volunteers with Hct, WBC, PLT and MPV within reference ranges were included in the testing process.
2.5. Taurine and Caffeine Working Solution
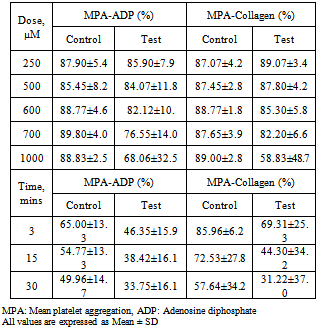
- The optimal sub maximal concentration of taurine (500 μM) that inhibits platelet hyperactivity in PRP was determined in our previous study[21]. The working solution (WS) of taurine was prepared from commercially available taurine (ICN Biomedicals Inc, Ohio). The extent of platelet aggregation exhibited by different concentrations of caffeine and the optimal dose (700 μM) required to cause inhibition of platelet aggregation was determined from the dose response curves constructed (Table 1). The WS of caffeine was prepared from commercially available caffeine (Sigma-Aldrich Inc, Australia) in modified Tyrode’s buffer (MTB).
|
2.6. Platelet Aggregation Assay
- PRP used in the testing, was obtained by the centrifugation of WB at 180 × g for 10 minutes. After separating PRP, PPP was obtained by further centrifugation of WB at 2000 × g for 10 minutes. Three different groups (taurine, caffeine and T+C) with controls were prepared, all having a final concentration of 500 μM taurine and 700 μM caffeine. The appropriate volumes of taurine and caffeine were then incubated with the separated PRP (37°C) for 60 minutes and 3 minutes respectively. The optimal incubation time was established for taurine from previously published data by Santhakumar et al[21]and for caffeine from the time response curve (Table 1). ADP (final concentration- 5 μM) and collagen (final concentration- 1 μg/mL) were used to stimulate platelet aggregation and the percentage of aggregation was recorded for 6 minutes using the Helena AggRam Platelet Aggregometer (Helena laboratory, Beaumont Texas, USA). These investigations were carried out within 2 hours post venipuncture.
2.7. Coagulation Assay
- Platelet poor plasma was analyzed using the C4 coagulation analyzer (Helena Laboratory, Beaumont Texas, USA) to evaluate the factors contributing to the coagulation cascade using the two most common assays: prothrombin time (PT) and cctivated partial thromboplastin time (APTT). Three different groups (taurine, caffeine and T+C) with controls were prepared, all having a final concentration of 500 μM taurine and 700 μM caffeine. The appropriate volumes of taurine and caffeine were then incubated with PPP (37°C) at 60 minutes and 3 minutes respectively. Appropriate volumes of PT, APTT reagent and calcium chloride were added to measure coagulation.
2.8. Lipid Profile and C-reactive Protein (CRP) Assays
- Serum obtained as a result of centrifugation of the SST was analyzed using the Cobas Integra 400® plus Biochemistry Analyzer (Roche diagnostics, Switzerland) to determine the effect of taurine, caffeine and T+C on cholesterol, triglycerides, glucose and CRP.
2.9. Statistical Analysis
- IBM© SPSS© Statistics software version 19 was used to perform a mixed-model ANOVA where gender was defined as the between-subjects factor, and treatment (defined as taurine, caffeine, or taurine and caffeine) and group (defined as control or treated) where specified as within-subject measures. Assumption testing of sphericity was not violated. To further elucidate the significance of pair-wise differences between these comparisons, paired t-tests were performed where necessary. Graphs were generated using GraphPad version 5.00 for Windows, GraphPad Software, San Diego California USA. Statistical significance was established when p < 0.05. Any significant statistical interactions were included in the analysis where applicable.
3. Results
- Baseline parameters for FBE, platelet aggregation, and coagulation profile were within normal reference ranges for all volunteers (Table 2). A significant inhibition of platelet aggregation induced by ADP was observed with caffeine (p=.025) and taurine combined with caffeine (p=0.001) treated samples (Fig. 1).
|
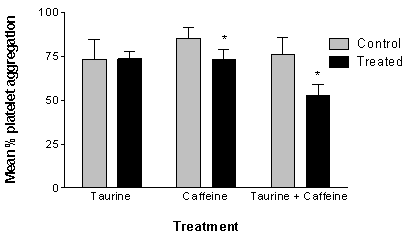 | Figure 1. The effect of taurine, caffeine and taurine combined with caffeine (T+C) on platelet aggregation induced by ADP. Significant inhibition of platelet aggregation is observed post treatment with caffeine (p=0.025); T+C treated samples. However, a greater inhibition of platelet aggregation is seen with the treatment of T+C (p=0.001). N= 11 (males = 5, females = 6). *Treated samples exhibit a statistically significant (p<0.05) in vitro inhibition of platelet aggregation when compared to its respective control samples. The error bars represent 95% confidence interval |
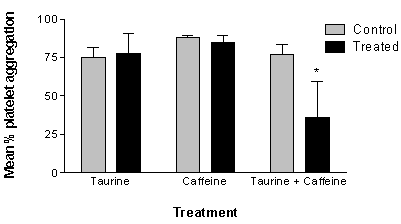 | Figure 2. The effect of taurine, caffeine and taurine combined with caffeine (T+C) on platelet aggregation induced by collagen. Significant inhibition of platelet aggregation is observed post treatment with T+C (p=0.001). N= 11 (males = 6, females = 5). *Treated samples exhibit a statistically significant (p<0.05) in vitro inhibition of platelet aggregation when compared to its respective control samples. The error bars represent 95% confidence interval |
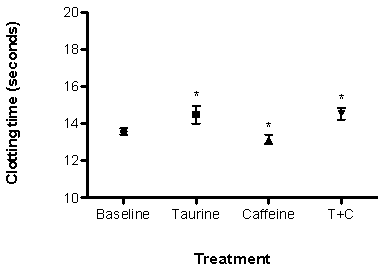 | Figure 3. The effect of taurine (500 µM), caffeine (700 µM) and taurine combined with caffeine (T+C) on Prothrombin clotting time (PT). Treatment with taurine and T+C increased PT while treatment with caffeine decreased clotting time. N= 11 (males = 6, females = 6). *Treated samples exhibit statistically significant (p < 0.05) changes to clotting time. The error bars represent 95% confidence interval |
4. Discussion
- The aim of the study was to evaluate the in vitro synergistic and discrete effects of taurine and caffeine on platelet activity and haemostatic function, using platelet aggregation, coagulation and lipid profile. The results from this study demonstrate a significant decrease in platelet aggregation in PRP with the treatment of caffeine and taurine combined with caffeine (T+C) induced by ADP (5 μM). A significant decrease in platelet function induced by collagen (1 μg/mL) was observed with the treatment of T+C only. These findings show that the synergistic activity of taurine and caffeine alleviated platelet aggregation greater than taurine or caffeine alone. In addition, platelet aggregation was carried out using minimal optimal doses of taurine (500 μM or 0.625 g/L) and caffeine (700 μM or 1.35 g/L) as opposed to high concentrations used by previous studies[29-31]. It has been reported that a 4g oral supplementation of taurine results in a plasma concentration of 690 μM or 0.86 g/L[32]. Hence, the concentration of taurine used in this in vitro study is similar to the plasma concentration of taurine after consuming concentrated shots of energy drink. The plasma concentration of caffeine used in our study is greater than that attainable after intake of concentrated shots of energy drinks. However, this concentration (700 μM) of caffeine synergistically with lowered doses of taurine has shown potential in attenuating platelet activity. Usually a biphasic platelet aggregation response, that is, a primary and secondary wave of aggregation, is evident after being induced by ADP platelet agonist. The exogenous ADP agonist initiates the primary wave of aggregation and the secondary wave by the endogenous ADP released by platelets[33]. In our study, it was seen that a considerable number of subjects demonstrated a loss of the secondary wave of aggregation response to ADP after treatment with T+C. Collagen platelet agonist induces only a single wave of platelet aggregation. It initiates a platelet shape change from discoid to a more spherical form characterized by a lag phase before the start of platelet aggregation[33]. It was also observed that, T+C alone considerably prolonged the initial lag phase and inhibited the platelet aggregation response. Further in vivo mechanistic studies would be required to verify the exact mechanism by which T+C exerts this effect on platelet aggregation induced by ADP and collagen.Prothrombin time (PT) and activated partial thromboplastin time (APTT) are common laboratory tests to evaluate the time taken for clot/thrombi to form in plasma. It helps to diagnose for blood coagulation disorders and the effectiveness of anticoagulant therapy. Our hypothesis is that taurine and caffeine synergistically will help in attenuating the rate of clot formation by retarding the deposition of fibrin on established thrombi or by preventing the formation of new thrombi. A considerable prolongation in prothrombin clotting time (PT) was observed after the in vitro administration of taurine and T+C but a significant decrease was seen after the treatment with caffeine. Though statistically significant, the effect on PT is not clinically significant as it remained within the normal reference ranges (11-15 seconds for adults). An increase or decrease in PT above or below the reference ranges is associated with an increased bleeding tendency or increased thrombotic tendency respectively. Due to the lack of a clinically significant impact on the clotting factors, taurine and T+C cannot be considered as effective anticoagulants but can be described as a haemostasis stabilizer and caffeine alone, a possible precursor to thrombotic tendencies. APTT remained unchanged after the treatment process, suggesting that neither taurine nor caffeine affected the intrinsic haemostatic pathway. This finding is in agreement with the study by Miglis et al. which demonstrated a statistically significant increase in thrombin time (TT) by taurine, while leaving PT and APTT unchanged[30]. However, the above results were not clinically significant since these measures were within normal reference ranges. Treatment with taurine or caffeine or T+C did not have an effect on cholesterol, triglycerides or glucose but a significant increase in C-reactive protein (CRP) was observed post caffeine treatment. CRP is an acute phase protein found in blood, the levels of which escalate during an infectious or inflammatory condition, cardiovascular disease or malignancy. This effect of caffeine on CRP is in accordance with the study by Ganapathi et al. where the investigators evaluated the effects on caffeine on acute-phase proteins (CRP being one of those proteins)[34]. According to this study, 2 mM of caffeine had led to a significant potentiating of CRP induction, ranging from 40 to 180–fold increase above the controls. Although the exact mechanism by which caffeine exerts its biological effects are not fully understood, it is believed to be mediated through increases in intracellular concentrations of cyclic adenosine monophosphate (cAMP) or calcium. This increase in cAMP by caffeine correlates to the inhibition of platelet activity demonstrated in our study. Further studies may be required to elucidate the relationship between caffeine and plasma CRP levels. Previous studies have shown that taurine[21, 30, 35] and caffeine[24-27, 36, 37], major components of energy drinks, individually attenuates platelet function, but a synergistic effect of taurine and caffeine (T+C) on platelet activity or hemostatic function have not been demonstrated. The results from our study suggest that T+C have a greater potential to inhibit platelet function than taurine or caffeine alone. This considerable alleviation of platelet aggregation by T+C may possibly attribute to reduce the hyper-coagulative states in cardiovascular risk population. In recent times, higher doses of anti-coagulant therapy have been responsible for causing a variety of side effects such as hemorrhagic strokes[38], gastric mucosal injury[39] and renal toxicity[40]. In addition to its sensitivity, it has been noted that in patients with stable CVD receiving anti-platelet therapy, some have been found to have incomplete inhibition of platelet aggregation or in other words resistance to the drug[41]. Taking into account their sensitivity and resistance, a supplement that would efficiently function alongside these drugs in alleviating platelet aggregation and reduce their dosage administered to CVD patients would prove to be effective and safe anti-platelet therapy.
5. Conclusions
- These data support our hypothesis that the synergistic effect of taurine and caffeine may be instrumental in reducing platelet activity and hence these components of energy drinks could be beneficial and effective in reducing platelet activity and thrombotic risks. Further in vivo mechanistic and interventional studies are required to examine the pathway involved in support of beneficial role of taurine and caffeine as a supplement to antiplatelet therapy in prevention of risk factors leading to CVD. In vivo synergistic effect of varying doses of taurine and caffeine will also be evaluated to obtain most effective and cardio-protective doses for energy drinks.
ACKNOWLEDGEMENTS
- We sincerely thank Osama Mohammed D Alshehri for technical support and all the volunteers for their participation in this study.