-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Food Science and Nutrition Engineering
p-ISSN: 2166-5168 e-ISSN: 2166-5192
2017; 7(4): 61-69
doi:10.5923/j.food.20170704.01

Nutrient Density of Complementary Foods Formulated from a Blend of Teff, Soybean and Orange-fleshed Sweet Potato
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMesfin W. Tenagashaw1, 2, John N. Kinyuru1, Glaston M. Kenji1, Eneyew T. Melaku3, Huyskens-Keil Susanne4
1Department of Food Science and Technology, Jomo Kenyatta University of Agriculture and Technology, Nairobi, Kenya
2Faculty of Chemical and Food Engineering, Bahir Dar Institute of Technology, Bahir Dar University, Bahir Dar, Ethiopia
3Department of Food Science and Applied Nutrition, Addis Ababa Science and Technology University, Addis Ababa, Ethiopia
4Division Urban Plant Ecophysiology, Faculty of Life Sciences, Humboldt-Universität zu Berlin, Berlin, Germany
Correspondence to: Mesfin W. Tenagashaw, Department of Food Science and Technology, Jomo Kenyatta University of Agriculture and Technology, Nairobi, Kenya.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Both protein-energy malnutrition and micronutrient malnutrition are highly prevalent among infants and children in poor community settings in the developing world, especially the Sub-Saharan African countries. One of the food-based approaches, food-to-food fortification, is now considered to be a good alternative for tackling this problem in a sustainable manner. In addition to breast milk, infants should be provided with energy– and nutrient-dense complementary foods from around the age of six month. In this study, teff, soybean and orange-fleshed sweet potato were separately processed into their respective flours and blended in a percentage ratio of 70:20:10, respectively, to prepare household- and industrial-level complementary foods (CFs). The developed CFs were analyzed for their protein, fat, energy, vitamin A, calcium, iron and zinc contents. Energy and nutrient densities were calculated from the respective laboratory values and compared with recommended levels for 6–8 month-old infants. The energy density of the complementary foods were in the range of 3.70 to 3.76 kcal/g satisfying the minimum requirement set for a cereal-based CF. The protein values of the CFs (3.50 to 4.79 mg/100 kcal) also met recommended levels set by different authorities. Calcium density of the CFs (60.48 to 67.84 mg/100 kcal) were somewhere above 50% of the WHO/FAO recommendation. Both iron (2.42 to 5.19 mg/100 kcal) and zinc (1.41 to 1.49 mg/100 kcal) values were slightly below the recommended levels for infants of 6–8 months of age. In conclusion, the developed teff-based complementary foods were found to be of satisfactory nutrient densities and thus can be recommended to be used by infants in low-income communities together with breast milk so as to minimize the adverse consequences of protein-energy malnutrition and micronutrient deficiency complications.
Keywords: Teff, orange-fleshed sweet potato, Household level, Complementary food, Energy density, Nutrient density, Micronutrient
Cite this paper: Mesfin W. Tenagashaw, John N. Kinyuru, Glaston M. Kenji, Eneyew T. Melaku, Huyskens-Keil Susanne, Nutrient Density of Complementary Foods Formulated from a Blend of Teff, Soybean and Orange-fleshed Sweet Potato, International Journal of Food Science and Nutrition Engineering, Vol. 7 No. 4, 2017, pp. 61-69. doi: 10.5923/j.food.20170704.01.
Article Outline
1. Introduction
- Every child has the undisputable right to be free from hunger and malnutrition so that it maintains a full physical growth and mental development [1, 2]. Because of the rapid rate of growth and development during the first two years of life, nutrient needs per unit body weight of infants and young children are very high [3]. However, in low-income communities of the developing countries, like those in the Sub-Saharan Africa, millions of infants and children cannot afford these nutrient needs and hence are affected by undernutrition [4]. This is because most foods fed to infants usually lack the recommended densities of the essential macro- and micro-nutrients such as energy, protein, vitamin A, iron and zinc. For example, according to a report by Ferguson and Darmon [5], when the nutrient densities of complementary foods fed to 6-11-month-old infants in many developing countries are compared with WHO recommended levels, less than 15% of the 115 foods examined achieved the recommended nutrient density levels for calcium, iron and zinc.Deficiency of energy and essential nutrients during the complementary feeding period (the age range of 6–24 months) can have serious consequences on the health and wellbeing of infants at a later age in life, some of which are long lasting/irreversible [6]. The issue is even worse during the second six months of life as the challenge for meeting nutrient needs, especially those of micronutrients, is the greatest at this time [7]. Therefore, infants should be provided with energy and nutrient-dense foods during the complementary feeding period, along with appropriate feeding practices and continued breastfeeding so as to ensure long-term optimal growth and development during the infancy period [1, 8-10]. The energy density of a food refers to the amount of calories per unit of volume or weight of the food and is very crucial in infant feeding [11, 12]. However, in the developing world, energy intake of infants and very young children of low-income groups, is considerably below the recommended daily amount [13]. Therefore, fulfilling this energy requirement is critical [14]. Similarly, nutrient density which refers to the amount of a nutrient per 100 kcal, is very vital in complementary feeding as infants need more of the macro- and micro-nutrients because of their rapid growth and development [7, 15]. The period of infancy in one’s life is referred to as the window of opportunity for preventing undernutrition and its long-term adverse consequences and thereby improve health and development [7, 16]. Thus, foods given to infants during this period, formally referred to as complementary foods, are required to adequately provide enough of the required energy, macro- and micro-nutrients including minerals and trace elements, especially iron and zinc [7] so that they will grow and develop to the best level. Therefore, interventions in complementary feeding that are effective at reducing malnutrition during this vulnerable period should be of a high priority [17]. It has been widely recommended that a food-based, comprehensive approach is more effective and sustainable than programmes targeting individual nutrient deficiencies in order to tackle the problem of infant malnutrition [17, 18]. One of the major reasons for the wide-spread problems of malnutrition among infants and children in low-income communities is the use of cereal-based foods that are characterized by low energy and nutrient density [19-22]. However, despite being low in most vitamins and minerals, cereal-based complementary foods are still the crucial sources of nutrients for the majority of infants in low-income countries as access to animal-origin foods or commercially fortified complementary foods is highly limited for a number of reasons [23, 24]. Therefore, there are global recommendations to help improve the nutrient density of such cereal-based complementary foods in a cost effective manner. One important approach is compositing cereals with legumes and tubers that are rich in either of the important macro- and/or micro-nutrients and this food-based strategy is referred to as food-to-food fortification [25, 26]. Moreover, the raw materials should be appropriately processed using recommended techniques that can enhance energy and nutrient densities [27-29]. In this study, complementary foods were developed from a composite of teff, soybean and orange-fleshed sweet potato using household- and industrial-level approaches. The macro- and micronutrient densities of the complementary foods were analyzed. The respective nutrient densities were then determined and compared with recommended levels (average desired nutrient densities) for 6-8 month-old infants.
2. Materials and Methods
2.1. Collection and Processing of Raw Materials
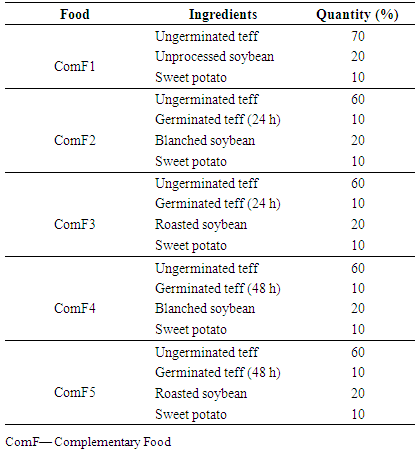
- The raw materials used, processing methods and formulation of the complementary foods were presented in detail in an earlier publication by Tenagashaw et al. [30] and briefly described as follows. Teff (Eragrostis tef), soybean (Glycine max) and orange-fleshed sweet potato (Ipomoea batatas) were used to develop the complementary foods. The teff grains were purchased from an open market and soybean and orange-fleshed sweet potato were obtained from Agricultural Research Centers in Ethiopia. Complementary foods were developed using household-level (combined household strategies) and industrial-level approach (extrusion cooking). In the development of household-level complementary foods, two different types of teff flours were used: ungerminated and germinated. Ungerminated teff grains were first sieved, cleaned, washed with tap water, dried and finally ground to fine flour. Some portion of dried teff grains (described above) were germinated for 24 and 48 h to prepare amylase-rich flour (ARF) following the method described by Badau et al. [31]. Soybean grains were processed using two different methods - blanching and roasting - according to methods described by Iombor et al. [32] and WFP [33], respectively. Similarly, orange-fleshed sweet potato tubers were processed according to the method described by Haile et al. [34]. Finally, the processed raw materials were ground to fine flour and blended to produce household-level complementary foods (ComF2 to ComF5) shown in Table 1.
|
2.2. Nutrient Composition Analysis
2.2.1. Determination of Macronutrients
- Macronutrients were analyzed according to AOAC International standard methods [35]. Moisture and ash were determined by the hot-air circulating oven (method #925.09) and through incineration (550 ºC) in a muffle furnace (method #923.03), respectively. Crude protein was determined by the micro-Kjeldahl method (method #979.09) and its content was obtained by multiplying the corresponding total nitrogen content by a factor of 6.25 [36]. Crude fat and crude fiber were determined following the AOAC methods, method #930.09 and method #962.09, respectively. Available carbohydrate was determined by difference whereas energy was calculated using the Atwater’s calorie conversion factors: 4 kcal/g for crude protein, 9 kcal/g for crude fat and 4 kcal/g for available carbohydrate [36].
2.2.2. Determination of Micronutrients
- β-Carotene was determined according to the method described by Rodriguez-Amaya and Kimura [37]. Calculations were made from a standard curve (R2 = 0.9993) drawn using β-carotene standard. The results were converted to retinol equivalents (RE) or vitamin A values using the conversion factor of 6 μg β-carotene: 1μg RE as described by FAO/WHO [38]. Calcium, iron and zinc were determined according to the method of AOAC International [35] Method #968.08.
2.2.3. Determination of Nutrient Density
- The nutrient density of the complementary foods were determined from the nutrient contents obtained through the laboratory analyses described above. The respective values of energy and nutrients were converted into energy density (kcal/g) and nutrient density (g/100 kcal) as described in the WHO/UNICEF guideline [12]. Energy density was determined by simply dividing the energy contents of the complementary foods by 100 whereas nutrient density was obtained by dividing the respective nutrient content of the complementary food by its energy content and then multiplying by 100.
2.3. Statistical Analysis
- The results are reported as mean values ± standard deviations of three independent determinations. Data were analyzed by one-way analysis of variance using IBM SPSS for Windows (Version 21). Tukey’s HSD test was used to compare differences between means when significant (p ≤ 0.05).
3. Results and Discussion
3.1. Energy Density
- As depicted in Figure 1, the energy density of the developed complementary foods were in the range of 3.70 to 3.76 kcal/g with no significant difference (p = 0.114) among the values. According to the Codex standard for processed cereal-based foods for infants and young children [39], the energy density of a cereal-based complementary food should be ≥ 0.8 kcal/g. Therefore, the complementary foods considerably met the minimum stipulated daily energy requirement for the targeted groups of infants. Therefore, a 6–8 month-old, infant can fulfill its energy requirement from the complementary foods by consuming two to three times a day with the option of adding snacks once or twice, which depends on the child’s appetite and signs of hunger and satiety, as recommended by PAHO/WHO and Dewey and Adu-Afarwuah [3, 17].
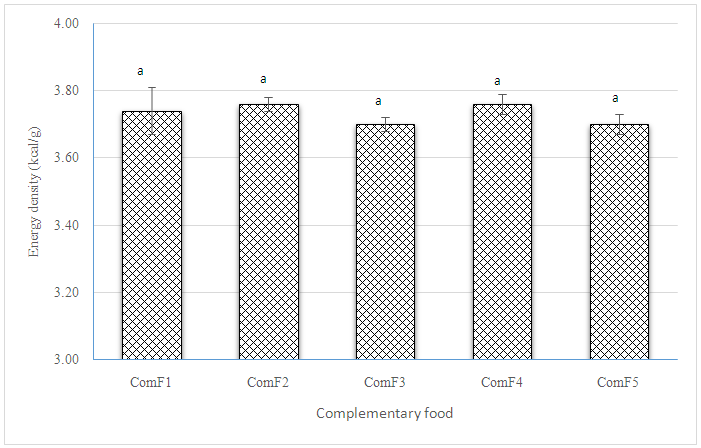 | Figure 1. Energy density of the complementary foods. Bars bearing different letters are significantly different at p ≤ 0.05 |
3.2. Macronutrient Density
- The protein density of the complementary foods was in the range of 3.50 to 4.79 g/100 kcal (Figure 2). This indicates that they are close to the upper limit of the recommended level described in the Codex standard (5.5 g/100 kcal) [39] for complementary feeding of infants aged between 6 and 24 months. However, compared to protein density recommendations by other researchers, these values are by far higher. For instance, according to Giugliani and Victora [11], the minimum protein density of plant-based complementary foods is 0.7 g/100 kcal. Similarly, Dewey and Brown [40], reported a protein density of 1.0 g/100 kcal for 6-8 month-old infants, which is still very low. As expected, the protein density of the extruded complementary food (ComF1) is significantly higher (p < 0.001) than those of the household complementary foods.
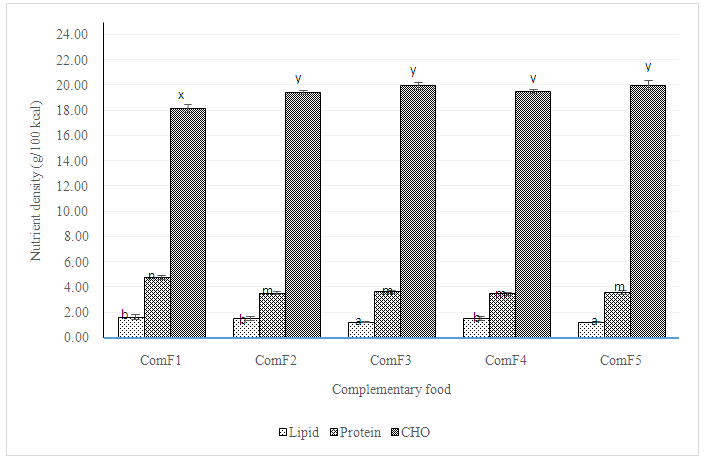 | Figure 2. Lipid, protein and carbohydrate density of the complementary foods. Bars with different letters in each case are significantly different at p ≤ 0.05 |
- In this study, the levels for lipid density ranged from 1.26 to 1.66 g/100 kcal (Figure 2). However, the maximum level of lipids required from cereal-based complementary foods stipulated by Codex is 4.5 g/100 kcal [39]. Thus, all complementary foods didn’t meet the minimum requirement of lipid density. Lipid densities of ComF3 and ComF5 are lower compared to the values of the other complementary foods which could be a result of the corresponding lower fat contents in the respective complementary foods [30]. However, the lipid density of complementary foods can be enhanced to a higher level through addition of a small quantity of fat/oil during the preparation of the complementary porridge [12, 22]. This also helps to enhance energy density without resulting in an overly thick preparation of the porridge [12]. The results for carbohydrate density in this study were within the range of 18.22 - 20.05 g/100 kcal (Figure 2). There is no recommended level of carbohydrate (CHO) density for plant-based complementary foods by Codex Alimentarius Comission. However, Koletzko et al. [41] recommended a range of 9–14 g/100 kcal. The higher carbohydrate values of the complementary foods in this study could be results of the appreciable degradation of starch to simple sugars during processing. However, this is advantageous to infants as the sugars produced can impart more sweetness to the complementary porridge thereby enabling the infant to take more of the food per feeding and minimize addition of table sugar during preparation of the porridge [42].
3.3. Micronutrient Density
- The vitamin A density of the complementary foods are presented in Figure 3. The values ranged from 24.55 to 42.81 RE/100 kcal. The minimum stipulated vitamin A density of cereal-based complementary foods for 6-8 month-old infants is 31 μg RE/100 kcal [40]. Therefore, all complementary foods except ComF1, had met this minimum requirement of vitamin A. The lower vitamin A density of ComF1 (24.55 RE/100 kcal) could be because of the relatively higher degradation of β-carotene during the extrusion cooking (a high temperature process) [43] compared to the values for the household-level complementary foods (40.19 - 42.81 RE/100 kcal) in which case the flour from orange-fleshed sweet potato was not exposed to a high temperature. However, in order to fully utilize the retinol from the β-carotene in the food, it is recommednded that plant-based complementary foods are fed together with breastmilk [11]. In general terms, the results in this study clued the importance of orange-fleshed sweet potato in fighting vitamin A deficiency disorder among infants and children in low-income countries. Moreover, it has been reported that β-carotene from sweet potato is substantially better absorbed / bioavailable than the one from leaves and vegetables in general [18, 44].
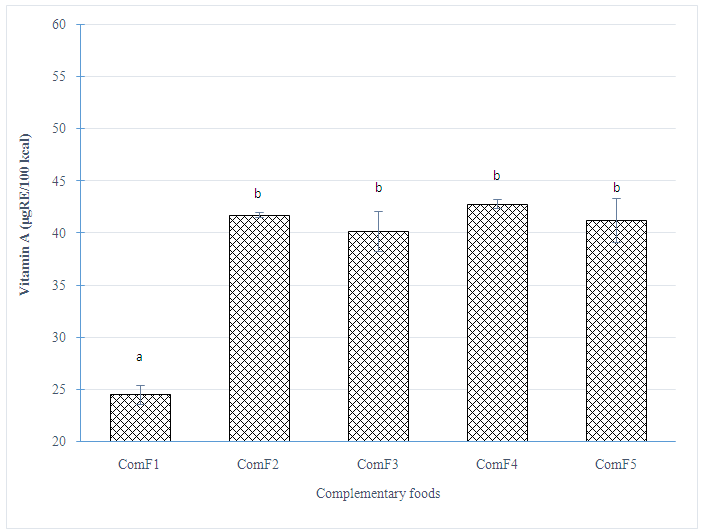 | Figure 3. Vitamin A density of complementary foods. Bars bearing different letters are significantly different at p ≤ 0.05 |
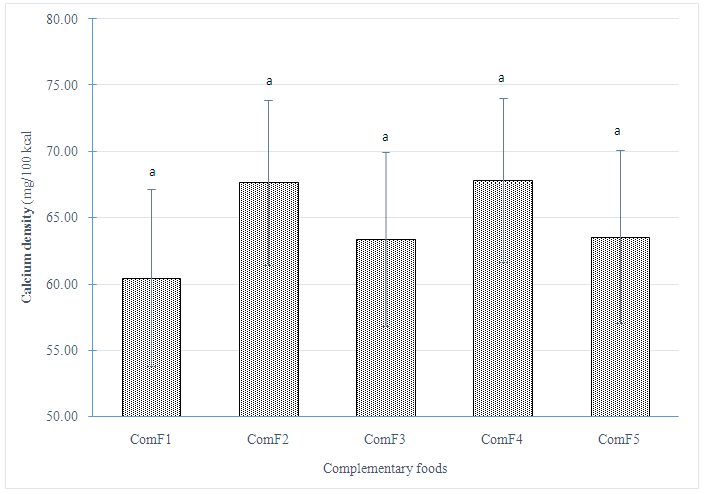 | Figure 4. Calcium density of complementary foods. Bars bearing different letters are significantly different at p ≤ 0.05 |
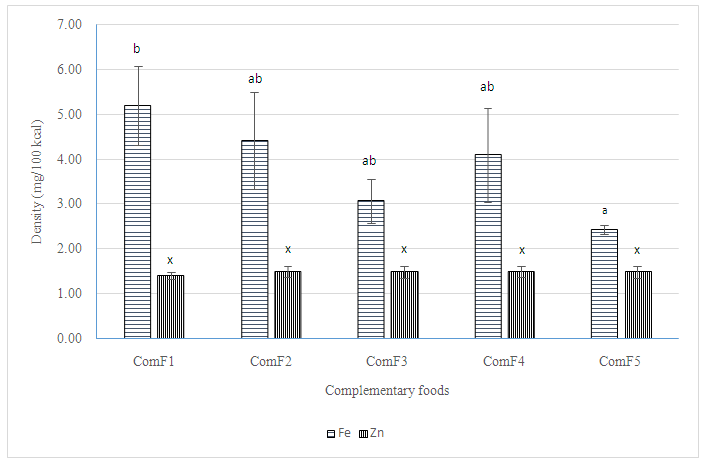 | Figure 5. Iron and zinc density of the complementary foods. Bars bearing different letters are significantly different at p ≤ 0.05 |
4. Conclusions
- This study revealed that blending of ungerminated and germinated teff with either blanched or roasted soybean and orange-fleshed sweet potato and also extrusion cooking of a blend of teff-soybean-sweet potato can produce complementary foods with improved energy and nutrient densities. The values obtained for energy and other vital nutrients (protein, fat, carbohydrate, vitamin A, iron and zinc) closely met the requirements for 6-8 month-old infants. The processing methods applied (soaking, germination, blanching, roasting, dehulling, extrusion) are promising in improving the nutrient densities of plant-based complementary foods. The satisfactory nutrient densities obtained in the complementary foods are indications of the importance of both appropriate processing of the raw materials, teff, soybean and sweet potato, and also their blending into composite flours.
ACKNOWLEDGEMENTS
- The fellowship awarded to the first author from RUFORUM/DAAD for conducting this research is highly acknowledged.