-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Food Science and Nutrition Engineering
p-ISSN: 2166-5168 e-ISSN: 2166-5192
2016; 6(3): 62-71
doi:10.5923/j.food.20160603.03

Availability and Utilization of Adequately Iodized Salt by Urban and Rural Households and Associated Factors in Southern Ethiopia, Sidama Zone, Bensa Woreda: A Comparative Cross-sectional Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMasresha Tsegaye1, Dejene Hailu2, Menen Zegeye1
1School of Nutrition, Food Science and Technology, Hawassa University, Hawassa, Ethiopia
2School of Public Health Science, Hawassa University, Hawassa, Ethiopia
Correspondence to: Masresha Tsegaye, School of Nutrition, Food Science and Technology, Hawassa University, Hawassa, Ethiopia.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Elimination of iodine deficiency disorders would be possible if almost all households consume adequately iodized salt. The coverage of iodized salt in Ethiopia is irregularly increasing but the percentage of households who consumed adequately iodized salt was lower from one locality to the other. Community based comparative cross-sectional study was conducted to assess availability of adequately iodized salt, utilization and factors associated to adequately iodized salt among urban and rural households in Sidama zone Bensa woreda during February to March, 2015 using structured and pre-tested questionnaire interview. Multi-stage sampling technique was used. Variables having p<0.25 in the bi-variate logistic regression were entered into multivariate logistic regression analysis and finally, variables having p< 0.05 and 95% Confidence Interval (CI) were considered as significantly associated. About 65.0% urban and 45.2% rural respondents were utilized adequately iodized salt and the proportion of urban households who utilized adequately iodized (≥15ppm) salt was significantly larger than that of rural households (Crude Odds Ratio (COR)=2.25). Buying salt from nearby shops Adjusted Odds Ratio (AOR)(95% CI) = 4.61(2.96 – 7.20), using packed salt AOR(95%CI) = 4.37(1.11–17.24), access to information AOR(95% CI) = 3.99 (2.54– 6.27), income of households AOR(95%CI = 7.16(4.55–11.29), those who attended formal education AOR (95% CI) = 3.34(1.96 - 5.69) and knowledge of the participants about the benefit of iodized salt AOR (95% CI) = 4.66 (3.01 –7.22) were significantly associated with availability of adequately iodized salt during multivariate analysis. Regardless of iodized salt coverage, availability of adequately iodized salt was lower in rural areas than urban. Buying salt from nearby shops, using packed salt, access to information, educational status and knowledge of the participants about the benefit of iodized salt were significantly associated with availability of adequately iodized salt. Households should be sensitized to importance of iodized salt, how to utilize it and its proper handling at the household level by different stakeholders.
Keywords: Adequately iodized salt, Utilization, Availability
Cite this paper: Masresha Tsegaye, Dejene Hailu, Menen Zegeye, Availability and Utilization of Adequately Iodized Salt by Urban and Rural Households and Associated Factors in Southern Ethiopia, Sidama Zone, Bensa Woreda: A Comparative Cross-sectional Study, International Journal of Food Science and Nutrition Engineering, Vol. 6 No. 3, 2016, pp. 62-71. doi: 10.5923/j.food.20160603.03.
Article Outline
1. Introduction
- Iodine is an element needed in small amount for the production of thyroid hormones. It is a critical component of thyroid hormones, which is necessary for controlling metabolic rate, growth and development of body structures, as well as neuronal function and development [21].The human body does not make iodine, so it is an essential part of diet [2]. Iodine is found in various foods such as cheese, cow’s milk, eggs, frozen yogurt, ice cream, Iodine containing multi vitamins, iodized table salt, saltwater fish, seaweeds, shellfish, soymilk and soy sauce[2]. Failure to have adequate iodine leads to insufficient production of thyroid hormones, which affect many different parts of the body, particularly muscle, heart, liver, kidney, thyroid gland, and the developing brain [19]. Inadequate hormone production adversely affects these tissues resulting in the disease collectively known as iodine deficiency disorders (IDDs). These include mental retardation, defects in development of the nervous system, goiter, growth retardation, reproductive failure, increased childhood mortality, and economic stagnation. The most devastating consequences of IDDs affect the development of human brain [19].According to world health organization (WHO) and international council for control of iodine deficiency disorder (ICCIDD) (2007) standard, elimination of IDD will be possible if more than 90% of the households consume adequately iodized salt [22]. But in Ethiopia only 15.4 percent of the households were using iodized salt in 2011 [5]. Furthermore, the percentage of households that use iodized salt was generally low. Only 23.2% of urban and 13.3% of rural households were reported to have used iodized salt [5]. In order to control and prevent micronutrient deficiencies, Ethiopia has set a goal to virtually eliminate IDD by the year 2015 through universal salt iodization (USI) by increasing the proportion of households using iodized salt from 15.4% to 95% [12]. According to the recent [8] report, the coverage of iodized salt at national level, assessed by Rapid Test Kit (RTK) and iodometric titration was 88.8% and 94.4%, respectively. However, households using adequately iodized salts (≥15ppm) were reported to constitute only 42.7%. In the southern nation nationalities and peoples (SNNP) region, the coverage of iodized salt utilization was 80.9% as assessed using RTK and 95.0% as assessed by iodometric titration. The coverage of adequately iodized salt (≥15ppm) was reported to be only 27% and 33.5% using RTK and iodometric titration [8].Iodized salt may be lacking in households of low socioeconomic status and in rural areas [14]. For example, in rural women from Sidama Zone, Southern Ethiopia, all participants reported that they had never consumed iodized Salt [24]. In another study conducted in the same zone but different area showed that, only 21% of households had adequately iodized salt [18]. Clearly, the usefulness of salt as a carrier of iodine needs to be assessed by means of household surveys, particularly in developing countries [14].According to [17], most part of the Bensa woreda (The smaller administrative units of zone) were high land and the staple foods of community include: Inset, maize, barley, wheat and etc. which do not include iodine-rich foods. The most abundant source of iodine is iodized salt. Even though there were no studies regarding prevalence of goiter and cretinism, visible goiter and children with sign of cretinism like dumbness, stunting, children with the problem of hearing and etc were highly prevalent [17].To the best of our knowledge, there were no studies regarding availability and utilization of adequately iodized salt at household level and associated factors in southern Ethiopia, both in urban and rural areas of Sidama zone, Bensa woreda. Thus, in order to reduce current high burden of IDDs and promote effective utilization of iodized salt, this study will assess availability and utilization of adequately iodized salt at household level and associated factors in southern Ethiopia, Sidama zone, Bensa woreda.
2. Materials and Methods
2.1. Description of the Study Area
- The study was conducted in eight urban and rural kebeles (The small administrative units) of Bensa Woreda in Southern Ethiopia. The woreda is located 131 kilometers east of Hawassa and 406 kilometers south of Addis Ababa, the capital of Ethiopia. According to woreda health office, Bensa is one of the 19 woredas in Sidama Zone and has an estimated area of 732.74 square kilometers. The population density in the woreda is 394.7 per square kilometer and is the second densely populated next to Boricha Woreda. In 2014, the total population of Bensa woreda was 315,122 of which 160,712 were women and 154,410 were men. Nearly, above 90% of woreda’s population live in rural areas. Bensa Woreda consists of 40 kebeles of which 37 are rural and 3 are urban. The total number of households at the selected kebeles is about 21,255. The woreda has three agro-ecological zones with 57% Highland, 26% Mid-land, and 17% Lowland. The major crops produced in the woreda include: inset (The name given for false banana plant which is locally staple food), maize, wheat, barley, haricot bean, teff and coffee; important cash crops include coffee, teff, maize, wheat, barley and vegetables such as kale, cabbage, onion and etc [17].Regarding availability of health facilities, there is one governmental (public) referral hospital under construction, eleven health centers and thirty seven health posts. Urban people have an access to private clinics, drug stores and drug venders which are an important source of iodized salt.
2.2. Study Design and Period
- The study employed a community based cross-sectional comparative study. Proportion of households who had availability to iodized salt and utilization were compared between the rural and urban households. In addition, factors associated to availability of adequately iodized salt were examined. The study was conducted from February to March, 2015.
2.3. The Study Population and Sampling Procedures
- The study population included all randomly selected households living in the selected urban and rural kebeles in Bensa woreda. Sample size estimation was carried out for each specific objective using double population proportion formula and the largest sample size of the specific objectives was taken as the total sample size of this study. Accordingly, the following assumptions were used to determine the largest sample size of the objectives: 95% CI, power of test = 80%, ratio of urban to rural households 1:2, non response rate =5%, (odds ratio =1.96, design effect =2 and 25.2% proportion of knowledge about the benefit of iodized salt [9]). Finally an Epi-Info software version 3.5, Statcalc application with the above assumptions provided a sample size of 909 households (303 urban and 606 rural households) and this was the total sample size of the study. A multi stage sampling technique was used to select a total of 8 kebeles and the corresponding households. At the first stage, 40 kebeles in the woreda were stratified into 3 urban and 37 rural kebeles. Then, since there was only one urban in the woreda, only the 37 rural kebeles were further stratified based on the agro-ecological zones into 21, 10 and 6 highland, midland and lowland kebeles, respectively. In the second stage, 1 out of 3 urban kebele was randomly selected. Similarly, proportionally allocated 4, 2 and 1 rural kebeles were randomly selected from highland, midland and lowland respectively. That would make a total of 8 kebeles (1 urban and 7 rural kebeles). At the third stage, urban households were randomly selected using the list of households available at the kebele office while households in the rural kebeles were proportionally allocated to the selected kebeles based on their population size. Finally, a cluster sampling of gotts (Sub-division of kebele) was applied to select households in the rural settings
2.4. Data Collection
- Data were collected using structured questionnaire by a face-to-face interviewing technique. Structured questionnaire was developed in English and translated into local language, and finally, it was retranslated into English by another language expert for checking consistency. The questionnaire included information on socio-demographic and economic characteristics, knowledge, environmental factors, availability and accessibility of iodized salt. The questionnaire was pre-tested on 10% of actual sample size out of the study population and based on the findings of the pre-test, necessary corrections were incorporated to the questionnaire prior to the actual survey. To assess the use of iodized salt at the household level, interviewers were asked households to provide a teaspoon of table salt used for cooking. The salt samples were tested for iodine content using the iodine rapid test kit (MBI Kits International). Furthermore, approximately 20 gram (2-3 teaspoons) of table salt sample were asked and collected using plastic bags from the houses of each respondent and iodine level was determined using portable digital electronic iodine checker (WYD, UNICEF) at the Hawassa university laboratory to examine absence, inadequacy, adequacy and excessiveness of iodine quantitatively. The samples were tested in duplicate and finally mean of each sample was taken. Data were collected by ten female Diploma and 3 B.Sc nurse supervisors. Data collectors and supervisors were trained for two days prior to the data collection.
2.5. Laboratory Analysis
- Determination of salt iodine using WYD iodine CheckerSalt iodine concentration was analyzed in duplicate using a WYD Iodine checker (National Salt Research Center Tianjin, China). The average of two readings was taken as iodine concentration of the sample. All procedures were performed according to the instructions provided in the WYD iodine Checker manual. Accordingly, after a zero point calibration, the instrument was calibrated using the KIO3 standard solution to liquid crystal display (LCD) reading out of 50±0.1. One gram of salt sample was used for the measurement. The salt was added in 50 ml tube and 10 ml of distilled water, 2ml of KI-starch solution and 2ml of diluted Sulphuric acid (H2SO4) were added. The tube was shaken thoroughly until the salt dissolved, then distilled water was added to make 50ml and the tube was shaken once again. A sample of each salt solution was placed specifically in the cell for the WYD iodine checker and the cell was inserted in to the cell holder of the instrument. The concentration was directly displayed on the LCD of the iodine checker.
2.6. Data Management and Analysis
- Data were entered in to SPSS statistical software version 16.0. Before the analysis, data were checked for completeness then were cleaned. Descriptive statistics was run using tables, graphs, and percentage points were calculated to describe household iodized salt coverage of study area. Binary logistic regression was used to identify factors associated to availability of adequately iodized salt. All independent variables that had a p-value <0.25 in the bivariate analysis were the candidates for multivariable logistic regression. Multivariable logistic regression model was used to identify factors affecting the availability of adequately iodized salt at household level. Comparison of urban and rural households’ utilization of adequately iodized salt, knowledge and utilization pattern/practices were made using Crude Odds Ratio (COR). P-value less than 0.05 was considered statistically significant. The degree of association between dependent and independent variables was reported using Adjusted Odds Ratio (AOR) and 95% CI.
2.7. Ethical Considerations
- Ethical clearance was obtained from Institutional Review Board of the Hawassa University. A formal letter of permission was written to Regional Health Office, Sidama Zonal Health Department, Bensa Woreda Health Office, and to each selected kebele (Small administrative units) administration. After explaining the purpose of the study, verbal consent was obtained from each study participant. Interviews were carried out privately in a separate room. Participants were also informed that participation was on voluntary basis and that they can withdraw at any time if they are not comfortable. Names or personal identifiers were not included in the questionnaires to ensure participants’ confidentiality. Health education on the importance and source of adequately iodized salt and proper handling of it at household level was given by the data collectors for households with inadequate iodized salt and with non iodated salt.
3. Results
3.1. Socio-Demographic and Economic Characteristics of Respondents
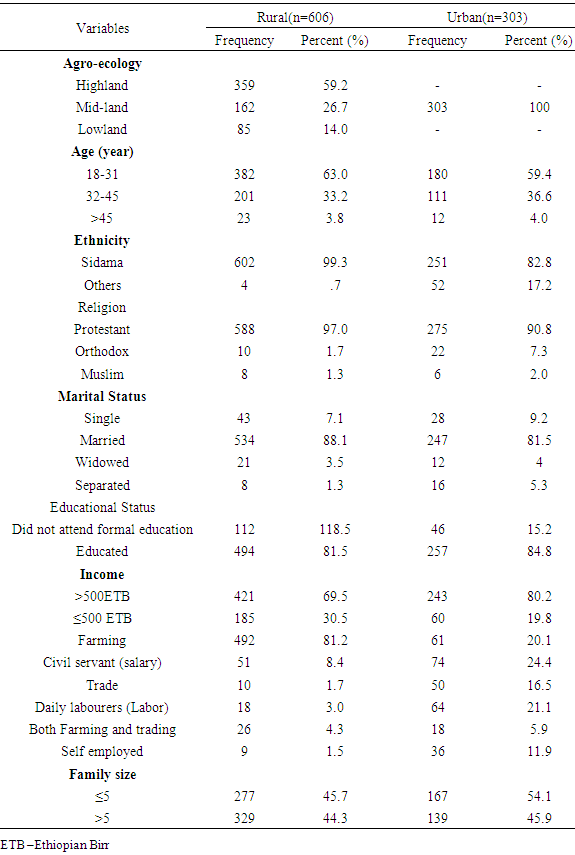
- A total of 909 (606 rural and 303 urban) households were included in this study with a response rate of 100%. The mean (±standard deviation) age of mothers who responded to the questionnaire was 30.9(±7.7) years for rural and 30.8(±9.2) years for urban respondents. Of 606 rural and 303 urban participants, 602 (99.3%) and 251(82.8%) were Sidama by ethnicity respectively. Five hundred eighty- eight (97%) rural and 575 (90.8%) urban residents were Protestant Christians, 534 (88.1%) rural and 247(81.5%) urban were married, 43(7.1%) rural and 28(9.2%) urban were single, 494(881.5%) rural and 257(84.8%) urban participants had attended formal education. Details of background characteristics of the respondents are presented in Table 1.
|
3.2. Availability and Adequacy of Iodine in Household Salts
- This study revealed that almost all the 594(98.0%) rural and 299(98.7%) urban households used iodized (>0ppm) salts. However, out of households who used iodized salts, only 274(45.2%) of the rural and 197(65.0%) of the urban households used adequately iodized salt (≥15 ppm) during the survey.No iodine was found in salts used by 12(2.0%) rural and 4(1.3%) urban households. The mean (±SD) iodine concentration of salt samples from urban households was 41.84(±5.1) ppm and that of rural was18.08 (±1.6) ppm. The proportion of urban and rural households who utilized adequately iodized salt (≥15ppm) was 65.0% and 42.1% respectively.This study showed that the proportion of urban households who utilized adequately iodized (≥15ppm) salt was significantly larger than that of rural households (COR=2.25). The overall concentration of iodine in the salts collected from the households ranged between 0 ppm and 231.5ppm which significantly deviates from the recommended range of 20 to 40 ppm at household level in order to provide adequate iodine [22] (Figure 1). Recommended range of 20 to 40 ppm at household level in order to provide adequate iodine [22] (Figure 1).
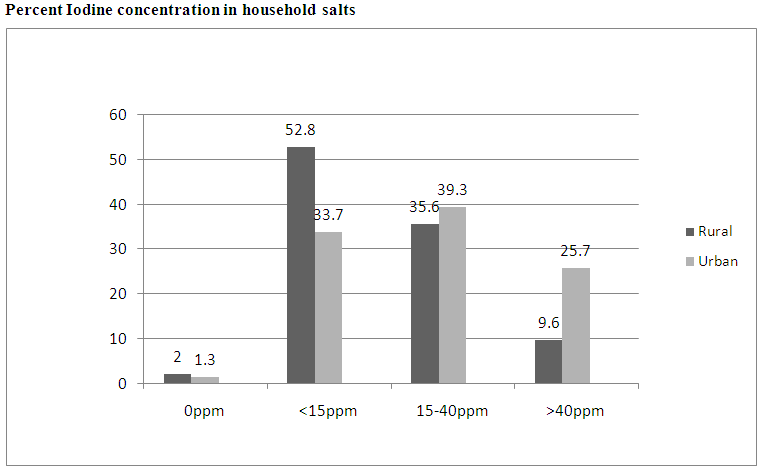 | Figure 1. Proportion of urban and rural residents utilizing iodized salt, Bensa Woreda, Sidama Zone, South Ethiopia, 2015 |
3.3. Knowledge and Utilization Pattern of Adequately Iodized Salt
3.3.1. Knowledge of Respondents Regarding the Importance of Iodized Salt
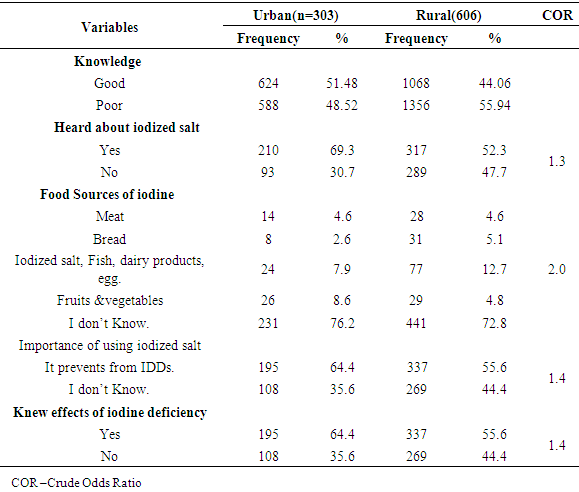
- Hundred ninety-five (64.4%) of urban and 337(55.6%) of rural participants said iodized salt prevents from IDDs and knew about iodine deficiency disorders and their effects on human beings.When asked if they have ever heard about iodized salt, 210(69.3%) urban and 317(52.3%) rural respondents said that they have heard about iodized salt from different sources.Fifty-four (17.8%) urban and 75(12.4%) rural participants have got the information from mass media (Radio and Television), and 101(16.7%) rural participants got from rural kebele Health Extension Workers (HEWs). The remaining 93(30.7%) urban and 289(47.7%) rural participants had not heard about iodized salt. In terms of knowledge of food sources of iodine, only 24(7.9%) urban and 77(12.7%) rural respondents mentioned iodized salt while 231(76.2%) urban and 441(72.8%) rural respondents did not know.Overall, 44.1% rural and 51.5% urban households had good and about 55.9% rural and 48.5% urban households had poor knowledge regarding the benefit of iodized salt, dietary sources of iodine and its effect on human beings respectively. The knowledge gap between urban and rural households is also statistically significant (Crude odds ratio=1.3) (Table 3).
|
3.3.2. Utilization Pattern/Practices/ of Iodized Salt
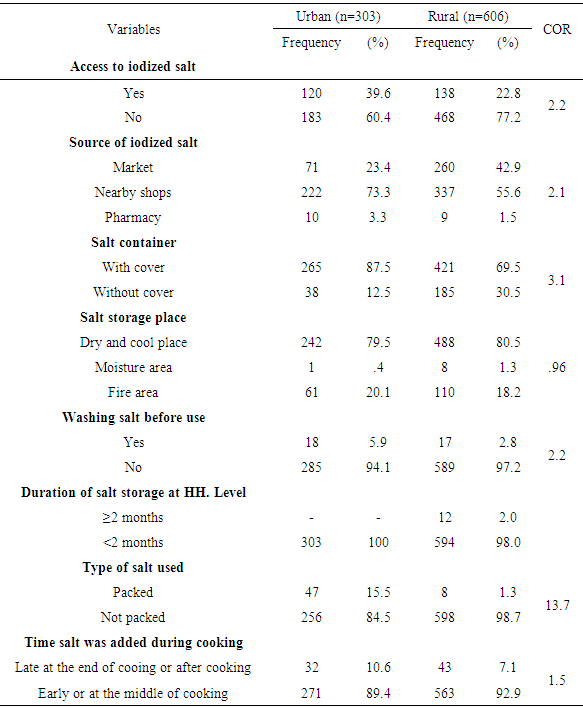
- Before testing the salt, the participants responded to a question that assessed the availability of iodized salt. About 183(60.4%) urban and 468(77.2%) rural participants said that they did not have iodized salt while only 120(39.6%) urban and 138(22.8%) rural participants reported that they have adequately iodized salt. The majority 222(73.3%) of urban and 337(55.6%) rural participants have got iodized salts from nearby shops.The main reasons that urban and rural respondents gave for not having adequately iodized salt were lack of knowledge about the benefit of iodized salt (38.6%, 76.9%), being expensive compared with table salt (17.6%, 2.4%), shortage of iodized salt in the market at certain times (9.4%, 8.5%), being less salty (2.6%, 0.0%), and not giving attention to it (31.8%, 12.2%) respectively.After testing the salt samples, the number of households who did not have adequately iodized salt decreased from 60.4% to 35.0% for urban and from 77.2% to 54.4% for rural households. Furthermore, among those who said that they had iodized salt, 158(61.2%) households have adequately iodized salt. Out of 651urban and rural respondents who said that they did not have iodized salt, the salt samples showed that 309(47.5%), 330(50.7%) and 12(1.8%) were ≥ 15 ppm, <15 ppm, and 0 ppm respectively. Two hundred fifty six (884.5%) urban and 598 (98.7%) rural households used non-packed salt; of these, 103(40.2%) urban and 332(55.5%) rural households used inadequately iodized salt. The remaining 47(15.5%) urban and 8(1.3%) rural households used packed salt. Out of urban and rural packed salt users, 44(93.6%) urban and 8(100%) rural households used adequately iodized salt. As compared to rural, better utilization of packed salt was shown by urban households (COR=13.7). In addition to type of salt, 265 (87.5%) of urban and 421(69.5%) of rural participants were used cover for their salt containers and urban households were performed better (COR=3.1). Majority 242(79.5%) of urban and 488(80.5%) of rural participants, stored salt in a dry place away from humidity and fire area. In this regard, both urban and rural households showed almost the same performance (COR=1). All the 303(100%) of urban and almost all 594(98.0%) of rural participants were stored salt for less than two months. However, 271(89.4%) of urban and 563(92.9%) of rural participants exposed their salt to heat by adding salt when the boiler/pot is on fire and. More urban households didn’t expose their salt to heat by adding salt late at the end of cooking or after cooking than rural households (COR=1.5). Moreover, almost all 285(94.1%) of urban and 589(97.2%) of rural respondents did not wash iodized salt but 18(5.9%) from urban and 17(2.8%) of rural washed salt to remove its impurities like Calcium carbonate (Table 4).
|
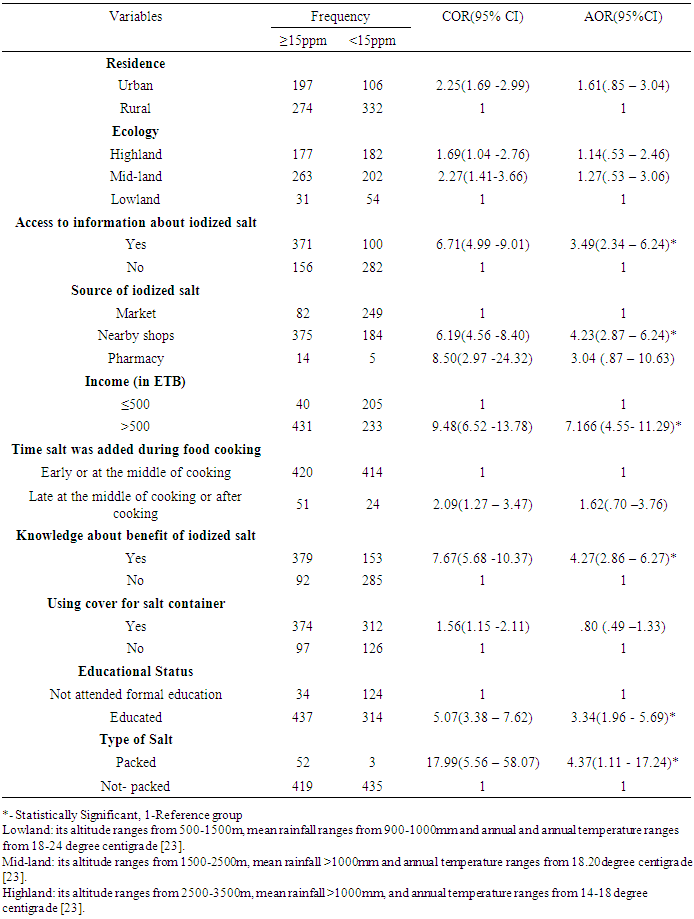
3.4. Factors Associated with Availability of Adequately Iodized Salt
- The bivariate analysis showed that being urban resident, living in highland or midland, income, educational status, source of iodized salt, using packed salt, salt not exposed to heat, using cover for salt container, knowledge about the benefit of iodized salt and access to information were significantly associated with availability to adequately iodized salt. However, having monthly income >500 ETB, buying salt from nearby shops, using packed salt, access to information, educational status and knowledge of the participants about the benefit of iodized salt were significantly associated with availability of adequately iodized salt in multivariate analysis (Table 5).
|
4. Discussion
- At household level, the recommended iodine concentration in salt should be 20-40 ppm in order to provide adequate iodine [22]. However, iodine level in the salt examined in this study was clearly not iodized in accordance with this recommendation. The iodine concentration of salt varied from 0 to 231.5ppm, which indicates the need to further improve the quality of iodized salt at the point of production. This might be due to traditional salt production process and manual iodization, manual mixing does not achieve the required uniformity throughout the salt pile and spraying KIO3 on to salt piles with knapsack sprayers may cause uneven iodine level. In addition to this raw salt with high level of impurities, high moisture, large crystal agglomerates may not be able to maintain the quantity and homogeneity of iodine [4].This study showed that iodized salt was found in almost all 594(98.0%) rural and 299(98.7%) urban households. But, adequately iodized salt (≥15 ppm) was found in 274(45.2%) rural and 197(65.0%) urban households.The observed percentages of both urban and rural areas were more or less similar to [8] report regarding iodized salt coverage but high as compared to Southern Nations Nationality and Peoples (SNNP) regional adequacy. According to the report, the coverage of iodized salt at SNNP regional level was 80.9% by Rapid Test Kits (RTK) and 95.0% by iodometric titration, but adequacy (≥15ppm) was reported to be only 27% and 33.5% using RTK and iodometric titration respectively [8].On the other hand, observed iodine adequacy percentages of both urban and rural areas were higher than researches carried out by different researchers in some urban and rural parts of the country. For instance, researches carried out in rural Maychew district reported (33.3%) in Tigray region [10], Gondar town (28.9%) [9], Ethiopian Demographic and Health Survey (EDHS) 2011 report which revealed the national coverage of iodized salt in Ethiopia was 15.4% and 12.2% for SNNP region [5] and that of Hawassa town, where more than half of the participants did not know the importance of iodized salt and no households were using adequately iodized salt [11]. The difference was statistically significant (p<0.001). This difference might be due to the number of reasons such as study area differences, current house to house educational strategy through health extension workers organized both in the urban and rural communities and media also played important role especially in urban areas of Ethiopia. But this finding had few similarities with EDHS (2011) report. Both our research and EDHS 2011 were conducted in urban and rural areas. In both cases, urban households had somehow better opportunity to utilize iodized salt. According to [5] report, the iodized salt users’ percentage of urban and rural dwellers was 23.2% and 13.3% respectively. This better availability and utilization of iodized salt in the study area might be due to urban dwellers had more access to information, proximity to nearby shops in order to buy iodized salt and better financial opportunities than rural communities.Using packed salt at the household level was significantly associated with availability of adequately iodized salt. Study conducted in Canada showed that iodine content of the salt remained constant and its distribution remained uniform for many months when the salt is packed and kept dry, preferably in a cool place and away from strong light [6]. Another similar study in Iraq showed that packed salt was mostly adequately iodized compared with non packed salt [7]. It’s clear that exposing iodized salt to sunlight gradually reduces iodine concentration in salt due to its’ volatile nature. But, iodine content will remain relatively constant if the salt is packed dry with an impermeable lining such as polyethylene bags.Knowledge of participants about the benefit of iodized salt was significantly associated with availability of adequately iodized salt. Similarly study conducted in Gondar town, North western part of Ethiopia reported that knowledge of participants about the iodized salt was significantly associated with availability of adequately iodized salt [9]. Another study conducted in Ghana showed the result of increased knowledge regarding the importance of using iodized salt and the effects of its deficiency in the diet of an individual; there has also been an increase in the consumption rate of iodized salt [3].In this study, knowledge of respondents about the benefit of iodized salt and effect of IDDs was noted to be poor. Overall, 48.5% urban and 55.9% rural participants had poor knowledge. Similarly, low level of communities’ knowledge was reported at another area in the country ([9], [11]). Unless households get access to information about iodized salt, know the importance of it and the consequences of shortage, they can’t consume and the reduction of iodine deficiency disorders will be unpredictable. Therefore, to build the communities knowledge is critical intervention of IDDs. Those respondents attended formal education were more likely to use adequately iodized salt. Similar study from Northern Ethiopia Laelay Maychew district reported that respondents who attended formal education were significantly different in availing adequately iodized salt in the household [11]. Another study conducted in Basra city of Iraq reported that household members with university education used iodized salt in the household than those with illiterate ones. This is due to the fact that education enhances awareness and decision making power of community [6]. Therefore, education should be one of the main ways of communicating information to eliminate IDDs.Having monthly income >500 ETB was significantly associated with availability of adequately iodized salt. The study conducted in Ghana revealed that compared to the richest category, all other lower levels of wealth were more likely to use non-iodized salt. It also shows that wealth is a significant determinant of one’s likelihood of using adequately iodized salt or not [1].A similar study conducted in Pakistan reported that income plays an important role and is the most important determinant in achieving adequate nutrition in the household [13]. And also study conducted in South Africa showed that households in low socio-economic categories comprised a vulnerable subset of the population at risk of being exposed to salt with low level of iodine [15]. According to the survey report of this research, majority of rural and one third of urban respondents realized that their income increase during cash crop harvesting time and they purchase quality food as well as goods only at this time. Furthermore, income source for 81.2% of rural and 20.1% urban households was only their farm and the family size for 44.3% rural and 45.9% urban respondents was ≥5. These all had its own negative influence on their income and finally unwillingly forced them to some extent to consume lower quality salt. Buying salt from nearby shops was significantly associated with availability of adequately iodized salt. This means prevention of exposing salt to sunlight and humidity increases iodine retention. Study conducted in Kazakhstan revealed that iodized salt slowly loses its iodine content when exposed to sunlight. The halogen iodide over time and exposure to excess oxygen and carbon dioxide slowly oxidizes to metal carbonate and elemental iodine which then evaporates [20]. A study conducted in Indian town, Delhi showed that there was about 31% iodine loss from iodized salt when exposed to sunlight [16]. As evidenced from this study, more than one third of the participants realized that they bought their salt from open markets. This means, individuals in these households were not getting adequately iodized salt since considerable amount of iodine was potentially lost. Therefore, creating awareness as there were options to buy salt from shops will lead them to avail adequately iodized salt in order to be prevented from IDDs. Access to information was significantly associated with availability of adequately iodized salt. Study done in Tigray showed that the most frequently mentioned sources of information on iodized salt were health workers (60.8%) [10]. Another study conducted in Ghana also showed media’s role; where access to formal education opportunities were not available, access to information through media served as an important instrument to educate the public and increase the community’s knowledge on the nutritional value of consuming adequately iodized salt [1]. Furthermore, currently there are good opportunities to inform community using both urban and rural Health extension workers and using community language-based mass media to build up households’ knowledge regarding the importance of iodized salt, proper handling and use of salt at household level, effects of IDDs and how to control it.
5. Conclusions
- Based on the findings of this study, the following conclusions are drawn:1. Although the coverage of iodized salt both in urban and rural areas was high, availability of adequately iodized salt at households level was low in study area.2. Majority of households did not have any information as well as knowledge about iodized salt and its importance but almost all households have been using iodized salt3. There was a wide variation in iodine concentration of both urban and rural salt samples. 4. Buying salt from nearby shops, attending formal education, access to information, knowledge about the benefit of iodized salt, monthly income, and using packed salt, were identified as factors associated with availability of adequately iodized salt at household level.
ACKNOWLEDGEMENTS
- The Authors would like to thank ENGINE/USAID/project of Hawassa University for their financial support of this research project. We are very grateful and would like to extend our thanks to Bensa Woreda administration, health and finance and economic development office’s management team for their support and encouragement. We would like to thank also study participants, data collectors, supervisors who participated in the study. We are very grateful and would like to extend our thanks to Professor Barbara Stoecker, for her suggestions and endless encouragement, Mr. Mesele Kifle for his unique contribution and Hawassa University School of Nutrition, Food Science and Technology (SNFST) Staff.