-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Food Science and Nutrition Engineering
p-ISSN: 2166-5168 e-ISSN: 2166-5192
2015; 5(3): 141-146
doi:10.5923/j.food.20150503.05
The Role of Orange Fleshed Sweet Potato (Ipomea batatas) for Combating Vitamin A Deficiency in Ethiopia: A Review
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLHenok Kurabachew
School Nutrition, Food Science and Technology, Hawassa University, College of Agriculture, Hawassa, Ethiopia
Correspondence to: Henok Kurabachew, School Nutrition, Food Science and Technology, Hawassa University, College of Agriculture, Hawassa, Ethiopia.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Vitamin A deficiency (VAD) is a serious public health problem in developing countries like Ethiopia. To combat this problem, food-based intervention is an appropriate and sustainable approach under Ethiopian circumstance along with supplementation of capsule and food fortification. Thus, orange-fleshed sweet potato (OFSP) which is rich in β-carotene has the potential to mitigate vitamin A deficiency problem. Given its high provitamin A content, low input requirements and adaptation to African farming systems, orange-fleshed sweet potatoes can make a sustainable and significant contribution to satisfy the vitamin A dietary requirement of the resource poor Ethiopian. In this regard different food product was developed in Tigray and Southern Ethiopia, from flours of OFSP blended with flours of other crops such as maize and wheat at different proportion. The developed food products were found to be rich in vitamin A content compared to the local staple food (which is poor in vitamin A) and reported to meet the daily RDA of the different age groups upon consumption of the products in the study areas. Therefore, much effort is required to popularize the crop, develop different recipes and food product which the rural community can use to combat vitamin A deficiency.
Keywords: Beta-carotene, Ipomeabatatas, Orange fleshed sweet potato, Vitamin A
Cite this paper: Henok Kurabachew, The Role of Orange Fleshed Sweet Potato (Ipomea batatas) for Combating Vitamin A Deficiency in Ethiopia: A Review, International Journal of Food Science and Nutrition Engineering, Vol. 5 No. 3, 2015, pp. 141-146. doi: 10.5923/j.food.20150503.05.
Article Outline
1. Introduction
- Vitamin A deficiency is of public health significance in the developing world. Globally, 190 million preschool children and 19 million pregnant women at risk of vitamin A deficiency (VAD) [1]. Countries of South-East Asia have the highest prevalence of VAD followed by Africa (49.9%), (17.3%) and (44.4%), (13.5%) in preschool children and pregnant woman, respectively [1]. This micronutrient deficiency also known as, hidden hunger, it not only prevents people from surviving and thriving as productive members of society, but also holds countries back in a cycle of poor nutrition, poor health, lost productivity, persistent poverty, and reduced economic growth [2]. Ethiopia has a population of about 85 million and is the second-most populous country in sub-Saharan Africa. The poor nutritional status of children and women continues to be a serious problem in Ethiopia. Approximately 14% are children under five years of age [3]. These children and their mothers suffer disproportionately from the poor health and nutrition situation in the country. In fact, malnutrition is the underlying cause of 57% of child deaths in Ethiopia [4]. As for women in the country, over a quarter had a low body mass index (BMI) (<18.5) in 2005; nearly one third among women 15-19 years of age. Contributing factors to under nutrition include widespread poverty, limited employment opportunities, poor infrastructure, high population pressure, low education levels, inadequate access to clean water and sanitation, high rates of migration and poor access to health services [5, 6]. Different national surveys and studies conducted in recent years affirm the presence of malnutrition to the degree that it is a major public health problem [7]. There has been a substantial decline in the proportion of children stunted and underweight in the last 15 years and a smaller decline in the prevalence of wasting. The 2014 Ethiopian Mini Demographic and Health Survey (EMDHS) indicated that 40% of children under age five were stunted, 9% were wasted and 25 % underweight in the country [8]. Besides the apparent macronutrient deficiencies, lack of sufficient vitamin A intake is a serious national problem that can lead to impaired sight or blindness, increased morbidity and mortality in young children and increased illness in pregnant and lactating women. Vitamin A deficiency (VAD) is a serious public health problem in Ethiopia [9] occurring mainly among children and women of childbearing age [10]. Furthermore the 2010 Nutrition Baseline Survey for the National Nutrition Program (NNP) indicated that the VAD problem is severe in Ethiopia, with an estimated prevalence of 61% among under five children years old [11]. Strategies to control vitamin A deficiency include dietary diversification, food fortification, and vitamin A supplementation [12]. Periodic and massive dose supplementation strategy was developed as a short-term life-saving intervention to deal with VAD. Though supplementation has been playing a great role in preventing VAD, people living in the remotest villages are sometimes beyond the reach of conventional supplementation programs as limited infrastructures make it less possible to establish and maintain reliable distribution [13]. Furthermore; this approach tends to be sustainable only through continued financial support from outside donors. The second approach is that of fortifying common foods with a micronutrient has been used successfully in some instances. But in Sub Saharan African countries where markets for foods are not well developed, it is difficult to identify appropriate foods to fortify in order to reach the consumers who are most at risk. Moreover, legal infrastructure has to be sufficiently strong to ensure that manufacturers comply with fortification laws [14]. Therefore, food-based intervention which improves dietary quality and quantity through diversification of crops (crops rich in ß - carotene) is the safest and most sustainable way of combating VAD in areas where chronic deficiencies are common [15]. The goal is to achieve and maintain an adequate intake of micronutrient-rich foods in the context of an adequate total diet [16]. Thus, food-based intervention is now proposed in the Ethiopia national VAD control framework as the long term option. This is important in order to make the gradual transition from subsidized periodic capsule-distribution effort to a more sustainable agricultural food-based intervention. In this regards orange fleshed sweet potato has the potential to be one of the most important crop used to combat vitamin A deficiency both in children under five years old and lactating women in Ethiopia.
2. The Problem: Vitamin A Deficiency
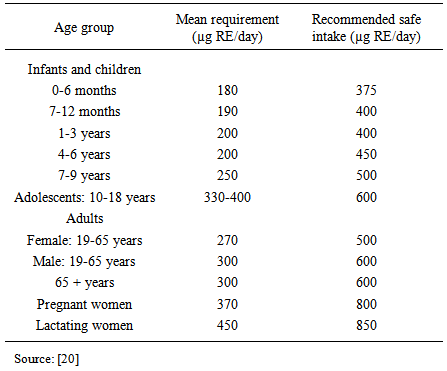
- Vitamin A is essential for good health and eyesight. When the body gets more vitamin A than it needs, the extra/excess vitamin A is stored in the liver. VAD occur due to a diet that provides too little bio-available vitamin A to meet physiologic needs which may be exacerbated by high rates of infection, especially diarrhea and measles [1]. It is a major nutritional concern in poor societies, especially in lower income countries. Vitamin A deficiency is one of the most important causes of preventable childhood blindness and is a major contributor to morbidity and mortality from infections. VAD is very common among young children than adults because children grow more quickly and suffer more from infections and severe malnutrition than adults do and also in pregnant and breastfeeding women [17, 18]. VAD can limit growth, weaken immunity, cause xeropthalmia leading to blindness, and increase mortality [19].In order to tackle vitamin A deficiency, daily nutritional need in vitamin for different class-ages was evaluated by FAO/WHO. The mean requirement intake is the minimum intake to prevent xeropthalmia in the absence of clinical or sub-clinical infection. Recommended safe is the average intake of vitamin A to permit adequate growth and other vitamin A dependent functions and maintain an acceptable total body reserve of the vitamin [20]. Recommended safe intake is also called Recommended Dietary Allowance (RDA). These requirements in microgram retinol equivalent per day (µg RE/day) are summarised as follows (Table 1).
|
3. Orange Fleshed Sweet Potato
- Sweet potato (Ipomea batatas [L.] Lam.) is a dicotyledons plant from the family Convolvulaceae that grows in tropical and subtropical areas. It occupies an important place in the agricultural production of Sub Saharan Africa countries, covering about 3.2 million hectares with a production estimated at 13.4 million tons of tubers 2005 [24]. Sweet potato generates large amounts of food per unit areas per unit time during relatively short rainy periods, tolerates occasional dry spells, and produces greater yields even in less fertile soil than crops such as maize [25].In Ethiopia, sweet potato is one of the most important crops for at least 20 million Ethiopians. It is produced in South, South Western and Eastern parts of the country, mainly in Oromia and Southern Nations, Nationalities and People Regional states (SNNPR) [26, 27]. The total area under sweet potato production in Ethiopia is 75000 ha with an average productivity 8t/ha. White fleshed sweet potato is a staple food for 13 million people in the Southern Regional State [13]. In contrast, orange-fleshed sweet potatoes are a relatively new crop to the country which is known to be a good source of vitamin A. OFSP is also a good source of energy (293 to 460 kJ/100 g) [28] easy to cultivate, vegetatively propagated, and fairly drought resistant once established. These characteristics make OFSP an excellent food security crop. Sweet potato is less labor intensive than most other staple crops and can be planted over a broad range of time without considerable yield loss.
3.1. Utilization of Orange-fleshed Sweet Potato to Combat Vitamin A Deficiency in Ethiopia
- An ex ante impact assessment indicated that orange fleshed sweet potato could make a major contribution to alleviating vitamin A malnutrition in Sub Saharan Africa [14]. The poor households in Sub-Saharan countries like Ethiopia cannot afford to consume the highly bioavailable vitamin A animal food source on a regular basis. In this regard OFSP is believed to represent the least expensive, year-round source of dietary vitamin A available to poor families [29]. OFSP is known to have an excellent amount of β -carotene which is highly bioavailable and converted into vitamin A (retinol) in human body [30, 31]. Just 100-125 g of boiled or steamed OFSP meet the daily recommended intake levels of vitamin A for children under five years of age [32]. Moreover, unlike many vegetables, the sweet potato has significant amounts of energy as well as vitamin A. So, OFSP is considered as an important staple food crop that can tackle the problem of inadequate caloric intake as well as vitamin V deficiency.Some earlier studies estimated that 6µg of β-carotene from plant sources were providing one retinol equivalent (RE). However, [33] suggested that the appropriate conversion factor varies by plant species and might be much lower. The conversion factor published by [34] stated that 12 µg β-carotene (or 24 µg of other carotenoids such as α-carotene and β-cryptoxanthin) found in foods corresponds to one retinol activity equivalent (RAE). A recent study in mashed sweet potato reported a conversion factor of 13:1 (13 µg β-carotene in mashed sweet potato equivalent to 1 µg retinol equivalent (RE) [30].OFSP is naturally bio-fortified crop and it has great potential to be used in food-based intervention programs to address vitamin A deficiency. The crop is a promising solution to vitamin A deficiency because it is rich in β-carotene and substantially better absorbed than others leaves and vegetables [35]. Among the ways to incorporate OFSP to foods, OFSP flour appears to be the most effective way for increasing the vitamin A content of OFSP enriched food products [36].In Tigray, Northern Ethiopia VA enriched bread was developed for pre-school children from blends of OFSP and locally available whole wheat flours (WWF) using a combination of OFSP: WWF of 0:100, 10:90, 20:80 and 30%:70% [37]. Accordingly, bread enriched with 30% OFSP flour contributed to 75-85 % of vitamin A daily requirement of children 3-6 years of age. The nutrient analysis of the formulated breads showed that moisture, ash, fiber, β-carotene increased significantly as proportion of OFSP flour increased; while protein, fat, carbohydrate and energy content decreased. This result suggests that, OFSP flour enriched breads have added advantages nutritionally since it provided the vitamin A which indicated the vital role of OFSP for alleviation of VAD [37].Another experiment done in Tigray indicated that the importance of mobile kitchens in increasing the consumption of OFSP as a nutritious food [38]. During the intervention period of 2010-2012, 7,700 households in 7 communities were covered to assess cost-effectiveness and adoption rates of OFSP in new communities using community women development groups as the primary extension agents. Accordingly, it was reported that 6,000 households were reached at an average cost of US$ 1.75 per household leading to the adoption of improved nutrition behavior among 5,000 households of the population in the targeted communities [38]. This evidence suggests that mobile kitchens are an effective tool for reaching large numbers of remote rural populations at a relatively low cost and in a short period of time. They can also lead to behavioral changes that will allow the adoption of OFSP in daily diets.Different researchers conducted studies on OFSP in Southern Ethiopia in different age groups. In line with this complementary food (porridge) was developed, which is rich in vitamin A, composed of bean, maize and OFSP for children of aged 6-23 months [39]. The combination of the complementary porridge was: maize (processed): bean: OFSP flours were (50:25:25), (45:25:30), (40:25:35) and the control complementary porridge was prepared from 100% raw maize flour. Sensory evaluation analysis showed that all formulated porridges were organoleptically accepted. On fresh weight basis, the complementary porridges in which OFSP was incorporated provided higher vitamin A (30.45 μg RAE/ - 85.52 μg RAE per 100 Kcal) than the control which provided 0.00 μg RAE per100 Kcal. Furthermore, a similar study was conducted on the consumption of vitamin A rich flat bread that was developed from flours of maize-OFSP for a lactating woman. The study began by interviewing 565 lactating woman to assess: their consumption of vitamin A rich foods, their awareness on vitamin A rich foods, assess and select the most common staple food of lactating mothers in the study area. Accordingly, it was reported 63.9% of the lactating mothers consumed vitamin A rich foods 3 times or more in the past 7 days preceding the survey [40]. In addition flat bread (unleavened bread) which was prepared from maize was found to be their main staple food for 88.14% of the lactating mothers. Therefore, flat bread food was prepared to improve the vitamin A content of the staple food from three combinations of maize-OFSP flours (25%,75), (30%, 70%), (35%,65%) and traditional maize-based flat bread served as a control. Result of the sensory evaluation indicated that all the formulations were accepted both by the laboratory panelists and lactating woman at community levels. The vitamin A contents (μg RAE) of maize and OFSP flours were found to be 0 and 888.01μg RAE per 100 gm, respectively. Among the flat breads samples in which OFSP flour was incorporated, the vitamin A content was 175.8, 197.2 and 269.6 μg RAE for 25%, 30% and 35%, respectively. The flat bread developed in this study weigh 100g in dry weigh basis and the total number of flat bread needed (per 100g) to meet the RDA was found to be 7,6,4 following 25:75, 30:70 and 35:65 proportion, respectively. Therefore, incorporating 35% flours of OFSP during preparation of traditional maize based flat bread can serve as a potential food source of vitamin A for lactating mothers residing in the study area.In another experiment an increase in the vitamin A level was observed with an increase in the proportion of OFSP flour and the vitamin A content ranged from 277.58 -344.33 μg/100 g for OFSP incorporated maize flat-bread [41]. The vitamin-A RDA for under-five children: 2-3 and 4-5 years of age was reported to be 400 µg/day and 450 µg/day, respectively [42]. Thus, if 2-3 years old children eat the 25, 30 and 35% OFSP incorporated maize flat- bread daily, they can get 69.3, 78.6 and 86.1% of the daily RDA of vitamin-A respectively. If 4-5 years old children can eat the same flat-bread daily they can get 61.6, 69.8 and 76.5% of their daily RDA of VA, respectively [41].Additional report on consumption of cookies developed from OFSP and wheat flours 40:60% combination, indicated that consumption of 12 and 6 cookies by pregnant/lactating woman and children (6-59 months) can provide 100% of their RDA of vitamin A [43]. The measured weight of cookie produced in this study was 61 g in dry weight basis and one can get 800µg β carotene or 67 µg vitamin A or RE for RDA by consuming one cookie. In another experiment, [44] developed OFSP-based juice products through blending with ginger and manjo juice following this combinations: product-1 (100% OFSP), product-2 (99% OFSP and 1% ginger), product-3 (90% OFSP and 10% mango juice), product-4 (80% OFSP and 20% mango juice), product-5 (89% OFSP, 10% mango juice and 1% ginger), product-6 (79% OFSP, 20 mango juice and 1% ginger) and product -7 (commercial mango juice). Results of the physico-chemical and nutritional analysis indicated that products flavoured with ginger had lower pH, higher acidity and ash, enhanced taste and mouth feel, colour and appearance. The phytate and bioavailability of iron and zinc was at acceptable range in ginger containing products. Products containing both ginger and mango juice had better physico-chemical, nutritional and sensory acceptability. Generally, in development of orange fleshed sweet potato juice combinations ingredients should be considered to improve overall acceptability and stability of products. Several beta-carotene-rich sweet potato based products were also developed in other African countries which were involved in the vitamin A for Africa initiative. In Uganda dried chips, flour and juice [45], golden bread [14] were produced as well as baby weaning food [15]. At house hold level, product development included chapatti (similar to pancakes), mandazi (similar to doughnuts), fired chips, cakes and crackies [15, 45, 46]. In Kenya mandazi’s, chapatti, crackies, onion bites, crisps and buns were produced [47, 45]. Thus, substitution of wheat flour with sweet potato in golden bread and mandazi’s made the product more profitable to vendors.Thus, promotion of food based agricultural interventions is particularly effective in reducing vitamin A deficiency in low income countries. In this regard, International Potato Centre (CIP) is working on the reduction food insecurity and malnutrition through the promotion of potato and OFSP in SNNPR and Tigray region, Ethiopia. CIP trained farmers on sweet potato agricultural practices such as vine multiplication, root production and utilization which will increase the productivity of the crop in the target areas [48]. In addition, women development groups leaders and farmers received training on different sweet potato food recipe preparation, nutritional value and agro-processing techniques of OFSP which will increase the knowledge level of the target group society on the cultivation and relevance of the crop in mitigating vitamin A deficiency. In, Ethiopia the crop has gaining more recognition due to its nutritional potential for combating vitamin A deficiency. In line with this, the Ethiopian Sweet Potato Research and Development Program launched breeding program for developing Vitamin-A rich OFSP in collaboration with CIP/PRAPACE which is based at Southern Agricultural Research Institute (SARI).
4. Conclusions
- In general, this review confirm that in Ethiopia poor dietary habit that depends on cereals coupled with poverty does not allow the poor majority to get vitamin-A rich foods even in years when food is plenty. Therefore, this calls for food diversification and modification of the existing staple through introduction of new food recipes incorporating nutrient-dense ingredients. In this regard OFSP, which is naturally rich in ß-carotene and excellent food source of provitamin A, is a good candidate crop for this approach. Therefore, this crop can be used for the long-term and sustainable food-based intervention to prevent vitamin A deficiency in Ethiopia. Thus, much should be done on recipe development, nutrition education and popularization of OFSP as food-nutrition security and income generating crop to the rural community where supplementation capsule and food fortification is not consistently available to solve the deep-rotted vitamin A deficiency problem the country is facing.
ACKNOWLEDGEMENTS
- The author would like to thank the Irish and USAID for their financial support for most of the research paper reviewed in this manuscript.