Tona Zema1, Tafese Bosha2, Tefera Belachew3
1College of Agriculture, Wollo University, Dessie, Ethiopia
2School of Nutrition, Food Scinece and Technology, Hawassa University, Hawassa, Ethiopia
3College of Public Health and Medical Sciences, Jimma University, Jimma, Ethiopia
Correspondence to: Tafese Bosha, School of Nutrition, Food Scinece and Technology, Hawassa University, Hawassa, Ethiopia.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Abstract
Zinc and vitamin A deficiencies are public health problems primarily due to chronic consumption of foods low in vitamin A and zinc. The information on consumption of vitamin A and zinc rich foods is essential to design relevant interventions for prevention of their deficiencies. Therefore, this study intended to assess household cultivation and dietary consumption of vitamin A and zinc rich foods by 6-23 months old children in Sodo Zuria woreda of Wolayta Zone, Southern Ethiopia. Applying two stage cluster sampling technique, 261 mother-child pairs were selected for the study. Mothers were interviewed on household cultivation of vitamin A and zinc rich food items and pumpkin (Cucurbita pepo). Food frequency questionnaire was employed to assess consumption of vitamin A and zinc rich foods by young children. Totally, 47.5% of the study participated households cultivated vitamin A rich fruits, 37.9% vitamin A rich vegetables and 65.1% zinc rich foods items. Among the children participated in the study, 65.9% consumed vitamin A rich foods at least three times and 40.54% zinc rich foods at least once in the last 7-days before the survey. Consumption of vitamin A rich foods, especially from plant-source, by 6-23 months old children was low. Intake of zinc rich foods was also low.
Keywords:
Household cultivation, Dietary consumption, Vitamin A, Zinc, 6-23 months old children, Sodo Zuria
Cite this paper: Tona Zema, Tafese Bosha, Tefera Belachew, A Baseline Survey on Household Cultivation and Dietary Consumption of Vitamin A and Zinc Rich Foods by 6-23 Months of Old Children in Sodo Zuria Woreda of Wolayta Zone, Southern Ethiopia, International Journal of Food Science and Nutrition Engineering, Vol. 5 No. 3, 2015, pp. 115-120. doi: 10.5923/j.food.20150503.02.
1. Introduction
Vitamin A and zinc deficiencies are remaining global public health problems primarily due to long term low intake of foods rich in these nutrients [1, 2]. VAD affects 33% of under five children worldwide [3] compromising immune systems and causing premature death to about one million young children each year in developing world [4]. In 2011, globally 26% and in Africa about 35.6% children were stunted leading to 116, 000 child deaths attributable to zinc deficiency alone [5]. The deficiency of vitamin A and zinc are remaining public health problems also in Ethiopia. The Ethiopian Demographic and Health Survey (EDHS) (2011) indicated that 44% of under five children were stunted in the country with zinc deficiency being one the major causes [6]. Tsegaye et al. indicated that 36.2% of children below 24 months had subclinical VAD in Ethiopia [7]. Another scholar also reported serum retinol level <0.7µmol/L in about 37.6% of under five children among food aid beneficiaries [8].Lack of access to micronutrient-rich foods such as fruits, vegetables, fortified foods and animal products is a major reason for children to suffer from vitamin A and zinc deficiencies in low income communities because they are either locally unavailable or too expensive to buy [9, 10]. Increasing ß-carotene in plant-foods [11], increasing production and consumption of vitamin A rich foods [12], periodic dosing of vitamin A supplements (usually every six months) [4], food fortification [9] and reducing levels of anti-nutrients like phytic acid in cereals and legume and including animal products in complementary foods are evidence-based practical strategies to reduce risk of developing vitamin A and zinc deficiencies in young children. However, there is limited information on household cultivation of vitamin A and zinc rich foods and their consumption by 6-23 months old children and utilization of pumpkin and its seed in complementary food preparations in southern Ethiopia. Therefore, this study intended to assess household cultivation and dietary consumption of vitamin A and zinc rich foods by 6-23 months old children in Sodo Zuria woreda.
2. Materials and Methods
2.1. Description of Study Area
This study was conducted in Sodo Zuria woreda of Wolayta zone from December 2013 to January 2014 using a community-based cross sectional study design. The area is located 380km from capital city (Addis Ababa) in Southern Ethiopia. According to the woreda health department, the woreda covers an area of 46,006 hectare and have 31 kebeles with total population of 19, 4460 (92,368 male and 102,092 female). Total number of under two years children was 10,224. According to the woreda agriculture office, the area is characterized by 5% low land (Dega) and 95% highland (Woinadega) with annual minimum and maximum rain fall of 30,447ml and 35,541ml respectively. Average maximum temperature is 28°C with minimum 18°C. Agriculture is the major economic activity of the area. Potato (Solanum tuberosum L.), sweet potato (Ipomoea batatas), cassava (Manihot esculenta), yam (Dioscorea alata), banana (Musa acuminate), enset (Enset ventricosum), maize (Zea mays L.), haricot bean (Phaseolus vulgaris), teff (Eragrostis tef (Zucc.) Trotter), sorghum (Sorghum bicolor L. Moench), pumpkin (Cucurbita pepo), broad bean (Vicia faba L., major), peas (Pisum sativum), kidney bean (Vicia faba) and chick-pea (Cicer arietinum) are main food crops growing in the area.
2.2. Sampling
The source population for this study was mothers in Sodo Zuria woreda who had 6-23 months children and lived at least six months in the area before the date of survey. The study population was randomly selected mother-child pairs from the source population. Sample size, 261, was calculated using a single population proportion formula considering design effect of 1.5 and margin error 0.05. Two stage cluster sampling technique was employed. Firstly, three kebeles were selected. Then, mothers having 6-23 months old children were indentified using children’s immunization card and by home to home visit. Sampling frame was prepared and study participants were selected by simple random sampling technique.
2.3. Data Collection
Structured questionnaire was adopted from EDHS 2011[8] and modified to the context of study area and objective. The questionnaire was translated in to local language, Wolaytigna, by a native speaker. Pre-testing was conducted by 5% of the total sample size in one kebele not included in the study. Native speakers of Wolaytigna who have completed grade 10 were recruited from each study kebele and trained for data collection. Sociodemographic and economic characteristics, child feeding practices and vitamin A supplementation were assessed. Moreover, home gardening of pumpkin, vitamin A and zinc rich foods items and incorporating pumpkin seed in complementary food preparations were studied. Young children’s consumption of vitamin A and zinc rich foods was assessed using food frequency questionnaire (FFQ). Mothers of 6-23 months old children were interviewed in selected households. Data collection was supervised.
2.4. Data Analysis
SPSS software version 20.0 was used for data entry, cleaning and analysis. Frequencies, percents, means and standard deviations were computed. Statistical significance was tested at p-value <0.05. Results were displayed using tables and graph.
2.5. Ethical Consideration
Ethical clearance was obtained from ethical review board of Hawassa University (HwU). Permission was obtained from the woreda health department. Informed consent was obtained from study participants.
3. Result
3.1. Sociodemographic and Economic Characteristics of Study Participants in Sodo Zuria
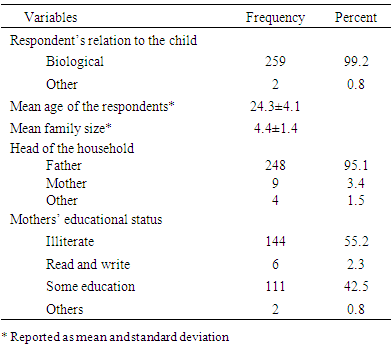
Response rate of the data collection was 100%. Almost all were biological mothers by relationship to the children with mean age of 24.3 years. Above 95% of the mothers were married living in male headed family with 4.4±1.4 members. More than half of study participated mothers didn’t receive formal education (Table 1). Table 1. Sociodemographic characteristics of study participants at Sodo Zuria
 |
| |
|
3.2. Economic Characteristics of Study Participants in Sodo Zuria
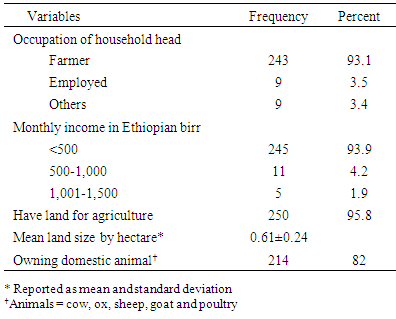
About 93% of the households were depending on agriculture with monthly income less than 500 Ethiopian birr. Though small, majority had land for farming and 82% owned at least one domestic animal (Table 2).Table 2. Economic characteristics of the study participants at Sodo Zuria
 |
| |
|
3.3. Household Cultivation of Vitamin A and Zinc Rich Food Items in Last 12 Months
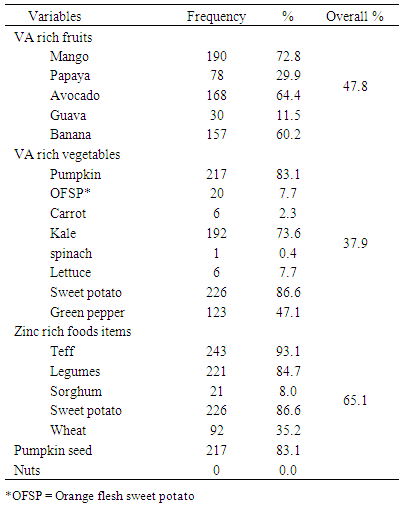
About 65% produced zinc rich food items and 41.7% vitamin A rich fruits and vegetables, in last 12 months before the date of survey. Many cultivated mango (72.8%), avocado (64.4%) and banana (60.2%), pumpkin (83.3%), kale (73.6%), sweet potato (86.6%) and green pepper (47.1%). Regarding zinc rich foods, four in every five households produced teff, legumes and pumpkin seed. Less number of households produced wheat and sorghum. None cultivated nuts and soybean (Table 3).Table 3. Household cultivation of vitamin A (VA) and zinc rich food items in last 12 months before the date of survey in Sodo Zuria
 |
| |
|
3.4. Home Gardening and Incorporating Pumpkin and its Seed in Complementary Food
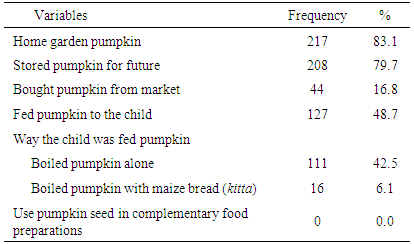
Majority cultivated pumpkin and 79.7% stored for future use. Few households, not cultivating, bought pumpkin from local markets. Nearly half feed boiled pumpkin to their children. However, use of pumpkin seed in complementary food preparation was not common in the area (Table 4).Table 4. Home gardening and incorporating pumpkin and its seed in complementary food preparations in Sodo Zuria
 |
| |
|
3.5. Child Feeding Practices in Sodo Zuria
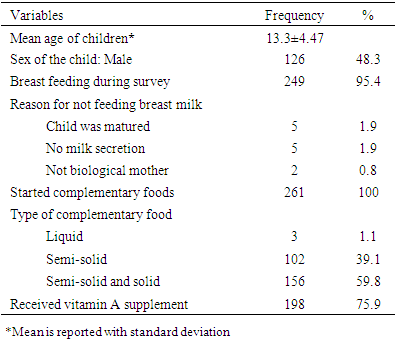
Among the children participated in study, 48.3% were male with mean age of 13.3 (±4.47) months. Almost all were living with their biological mothers at the time of survey, 95.4% being breast fed. All children started complementary food with more than 98% fed semi-solid or both semisolid and solid foods. About 75.9% of the children took vitamin A supplement. Few were sick two weeks before the survey (Table 5).Table 5. Feeding practices of children participated in the study in Sodo Zuria
 |
| |
|
3.6. Consumption of VA and Zinc Rich Foods by Children Participated in the Study in Sodo Zuria
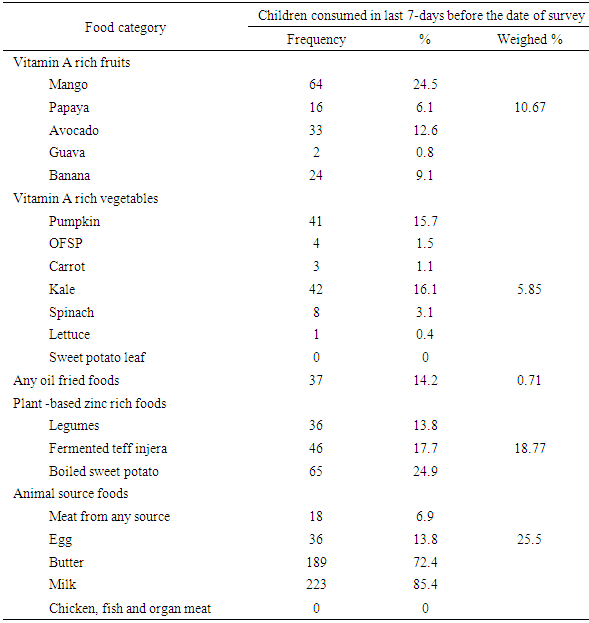
Only 16.52% of the study participated children consumed vitamin A and zinc rich foods, 18.77% zinc rich plant-based foods at least once in 7-days before the survey. None of the children consumed any fortified cereals. Among vitamin A rich fruits and vegetables; mango was consumed by almost one fourth of the children. Consumption of avocado, banana, pumpkin and kale was low. Similarly, boiled sweet potato was consumed by about one fourth. None of the children ate pumpkin seed, soybean, lentils, fermented wheat and sorghum injera. Over all only 25.5% consumed zinc and vitamin A rich animal source foods. Above 85% consumed milk, 72.4% butter, but few ate egg (13.8%) and flesh meat (6.9%). None consumed chicken, fish and organ meat. In total, 65.9% of the children consumed vitamin A rich foods at least three times and 40.54% plant and animal source zinc rich foods in last 7-days (Table 6 and Figure 1). Table 6. Consumption of vitamin A and zinc rich food by children participated in the study in last 7-days before the survey in Sodo Zuria
 |
| |
|
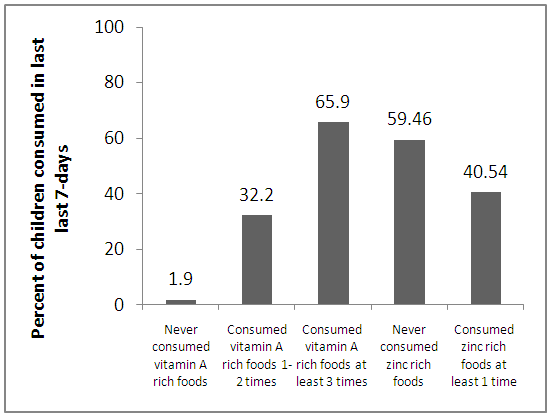 | Figure 1. Consummation of vitamin A and zinc rich foods by 6-23 months old children in the last 7-days before the survey in Sodo Zuria |
4. Discussions
The mean family size, 4.4±1.4, found in the current study is slightly lower than the reported 5.5 by Ethiopian Health and Nutrition Research Institute (EHNRI) [14]. This difference may be due to difference in scope of the study, sample size, sampled participants and inclusion criteria. The observed 57.5% prevalence of illiteracy among mothers is nearly similar with the EDHS 2011 report (56.1%) [8]. It was found that the main occupation of household heads was farming accounting 93.1% which is comparable with 92.5% reported by Oumer et al. on similar community [15]. The mean land size, 0.61 hectare, reported in current study is also supported by the same scholar’s finding (0.65 hectare) [15]. About 95.4% of the children participated in this study were breast fed from birth to the survey date which is also comparable with the 98.8% reported elsewhere on similar age group [16]. The observed low income (less than 500 ETB) [17], large family size and small land holding [6], seasonal variation [18] together with the high illiteracy of mothers could contribute to the observed low consumption of vitamin A and zinc rich foods among young children in the study area. Vitamin A supplementation coverage, 75.9%, was slightly lower than the reported 83.1% by Samson et al. on 6-59 months children [19]. This variation might be due to the difference in study population. It was found that cultivation of fruits was slightly lower but that of vegetables was higher than the reports of Tsegaye et al. [6]. Also vitamin A rich fruits and vegetables consumption by young children was a little bit lower. These differences may be due to the difference in scopes of the two studies and seasonal variations. A community-based cross-sectional study conducted on a similar rural community reported that 4.4% of the young children consumed animal source foods and 12.7% vitamin A rich fruits and vegetables in 24 hours preceding the survey [13]. The observed increase in consumption of these foods in the current study might be due to the efforts of health extension workers visiting home to home and counselling mothers.The observed poor utilization of pumpkin, which is a good source of vitamin and zinc, in complementary food preparations may due to lack of mother’s awareness and observed low educational level. The current study revealed low consumption of animal source foods, especially meat, fish and poultry which are rich sources of vitamin A and zinc by young children. This finding is in line with the report of EDHS 2011 [8].Consumption of zinc rich plant-source food items like legumes, sweet potato and teff injera was lower than what was reported by Malde et al. [20] in Wonji Shoa Sugar Estate, Ethiopia. This variation might be due to the difference in sample size, sampling technique, agro-ecology and seasonal variations. The current study found that vitamin A rich food consumption was below (65.9%) the WHO indicator of a community at risk for VAD. Accordingly, a community can be considered at risk for VAD, if less than 75% of 6-71 months old children consume vitamin A rich foods at least three times in 7-days [21]. This result is consistent with that of Tsegaye et al. who noticed that many of Ethiopian communities are at risk for VAD [6].
5. Conclusions
This study revealed that more than half of the households did not cultivate vitamin A rich fruits and vegetables. Also cultivation of zinc rich foods was not high. It also showed that pumpkin production was high in the area, but pumpkin seed was not used in complementary food preparations. The study also identified a lower consumption of vitamin A rich foods, especially from plant-source, by 6-23 months old children. It also discovered low intake of zinc rich foods in the same age group.
ACKNOWLEDGEMENTS
The researchers gratefully thank USAID, ENGINE project, Wollo University and HwU for funding this research. We also highly acknowledge our study participants and data collectors.
References
| [1] | International Vitamin A Consultative Group (IVACG). 1997. Maternal night blindness: extent and associated risk factors. International Life Sciences Institute, Washington, DC. |
| [2] | Stephenson C.B. 2001. Vitamin A, infection and immune function. Annual Review of Nutrition, 21: 167–192. |
| [3] | World Health Organization (WHO), 2009. Global prevalence of vitamin A deficiency in populations at risk 1995 – 2005: WHO global database on vitamin A deficiency. Geneva, Switzerland: WHO Press. |
| [4] | Micronutrient Initiative, 2009. Investing in the Future: A united call to action on vitamin and mineral deficiencies. Micronutrient Initiative, Flour Fortification Initiative, USAID, GAIN, WHO, the World Bank, and UNICEF: Ontario Canada. |
| [5] | UNICEF/WHO/World Bank. 2012. Levels and trends in child malnutrition. Joint child malnutrition estimates. New York, NY: United Nations International Children’s Fund; Geneva: World Health Organization; Washington, DC: World Bank. |
| [6] | Central Statistical Agency. 2012. Ethiopia Demographic and Health Survey, Addis Ababa, Ethiopia and ICF International Calverton, Maryland, USA. |
| [7] | Haidar Jemal. 2011. Common micronutrient deficiencies among food aid beneficiaries: Evidence from refugees in Ethiopia. Review article. Ethiopian Journal of Health Development, 25(3): 222-229. |
| [8] | Tsegaye Demissie, Ahmed Ali and Dilnesaw Zerfu, 2009. Availability and consumption of fruits and vegetables in nine regions of Ethiopia with special emphasis to vitamin A deficiency. Ethiop. J. Health Dev. 23(3): 216-222. |
| [9] | World Health Organization. 2001. Complementary feeding report of the global consultation: Summary of guiding principles, Geneva. PP 10-13. |
| [10] | Brown K.H., Rivera J.A., Bhutta Z., Gibson R.S., King J.C., Lonnerdal B., Ruel M.T., Sandtrom B., Wasantwisut E. and Hotz C. 2004. Assessment of the risk of zinc deficiency in populations and options for its control. International Zinc Nutrition Consultative Group (IZiNCG). Food Nutrition Bulletin, 25 (1 suppl 2):S99–203. |
| [11] | Khush G.S. 2002. The Promise of Biotechnology in Addressing Current Nutritional Problems in Developing Countries. Food Nutrition Bulletin, 23: 354–357. |
| [12] | Ruel M.T. and Levin C.E. 2006. Assessing the Potential for Food-Based Strategies to Reduce Vitamin A and Iron Deficiencies: A Review of Recent Evidence Food Consumption and Nutrition Division. International Food Policy Research Institute 2033 K Street, N.W. Washington, D.C. U.S.A. |
| [13] | Debebe Moges, Yewelsew A., Rosalind S. Gibson. 2009. Assessing the nutritional adequacy of complementary foods and infant and young child feeding practices in Sodo Zuria Woreda, Wolayta Zone, Southern Ethiopia: Masters Degree Thesis. Hawassa University, Hawassa, Ethiopia, P1-49. |
| [14] | Ethiopian Health and Nutrition Research Institute (EHNRI). 2009/10. Nutrition baseline survey report for the national nutrition program of Ethiopia. Addis Ababa, Ethiopia. |
| [15] | Oumer Seid Ahmed, Singh P. and Getenesh Berihanu, 2012. Assessment of Dietary Consumption of Vitamin A by Preschool Children in Southern Ethiopia- A Cross Sectional Study. International Journal of Environmental Sciences. 1(4): 279-284. |
| [16] | Kana S.MM., Kikafunda J.K., Meli F.C., Gouado I., Zollo P.H.A., Oberleas D. and Tetanye E. 2012.Young Children Feeding and Zinc Levels of Complementary Foods In Western Cameroon. African Journal of Food, Agriculture, Nutrition and Development. 11 (4): ISSN 1684-5374. |
| [17] | Ruel M.T., Minot N. and Smith L. 2005. Patterns and determinants of fruit and vegetable consumption in sub-Saharan Africa: a multi-country comparison, IFPRI (International Food Policy Research Institute), Washington DC. |
| [18] | Deepa K.S., Bharati P. and Naik R.K. 2004. Seasonal variations in nutritional status of adolescent girls. J. Hum. Ecol., 15: 147-151. |
| [19] | Samson Gebremedihin, Eskinder Loha, Yewelsew Abebe and Gulelat Dessie. 2009. Assessment of vitamin A supplementation coverage and its association with childhood illness in Boloso Sore Woreda, Wolayta Zone, SNNP Region, Ethiopia: Ethiop. J. Health Dev. 23(3): 223-228. |
| [20] | Malde M.K., Zerihun L., Bjorvatn K. and Julshamn K. 2010. Intake of iron, zinc and iodine in 28 Ethiopian children living in Wonji Shoa Sugar Estate, assessed by duplicate portion technique. Academic Journals, 5(8): 730-736, ISSN 1992-2248. |
| [21] | World Health Organization. 1996. Indicators for assessing vitamin A deficiency and their application in monitoring and evaluating intervention programmes. Geneva, WHO, 1996 (WHO/NUT/96.10;http://whqlibdoc.who.int/hq/1996/WHO_NUT_96.10.pdf, accessed on 24 June 2004. |
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML