-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Education
p-ISSN: 2162-9463 e-ISSN: 2162-8467
2019; 9(2): 23-29
doi:10.5923/j.edu.20190902.01

Utilization of Rehabilitation Programmes on Needy Inpatients in University of Maiduguri Teaching Hospital Borno State, Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAugusta Obum Okute1, Rufina Stephen Hamafyelto2
1Department of Continuing Education and Extension Service, Faculty of Education, University of Maiduguri, Borno State, Nigeria
2Department of Vocational Education, Faculty of Education, University of Maiduguri, Borno State, Nigeria
Correspondence to: Augusta Obum Okute, Department of Continuing Education and Extension Service, Faculty of Education, University of Maiduguri, Borno State, Nigeria.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

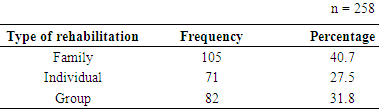
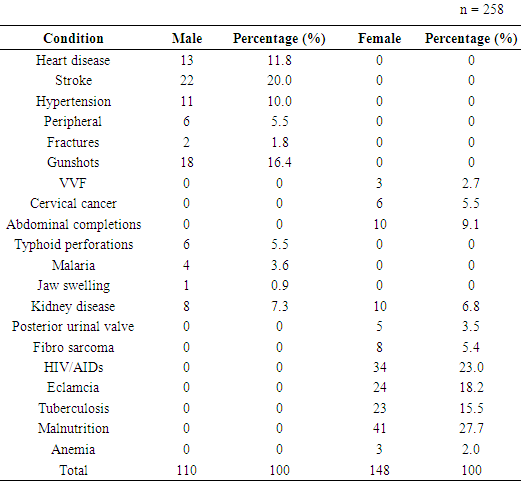
Rehabilitation is a known subject in both community development and vocational education literature especially aspects dealing with rehabilitation of disabled persons, leprosies, mental health and social and psychological wellbeing as well individuals who fail to measure up in certain educational tasks. However, this paper focused mainly on people who suffered varying degrees on ill-health in the hospital and required interventions in form of rehabilitation therapies. As both community development worker and vocational educationists, it is imperative to advance support to the needy patients in the hospital. This paper examined the utilization of rehabilitation programmes on needy inpatients in University of Maiduguri Teaching Hospital Borno state, Nigeria. The objective is to assess the rehabilitation of needy inpatients in University of Maiduguri Teaching Hospital in Nigeria. It was hypothesized in the study that there is no significant difference in rehabilitation programmes among needy in-patients across the wards in the hospital. There are two hundred and eight (258) in-patients in this study identified by the nurses in charge of each ward and staff of the social welfare unit in University of Maiduguri teaching hospital. Of this number, 110 were males and 148 female in-patients with a minimum age of 4 years and maximum of 63 years. A 31-item questionnaire divided into three section; namely, Group rehabilitation, Family rehabilitation and Individual rehabilitation was used to collect data from the respondents. The reliability index of the questionnaire was .79 Cronbach’s alpha. Results showed that 105 (40.7%) in-patients received family rehabilitation; 71 (27.5%) of the patients were given individual rehabilitation while 82 (31.8%) received group rehabilitation.
Keywords: Rehabilitation, Utilization, Needy in-patients
Cite this paper: Augusta Obum Okute, Rufina Stephen Hamafyelto, Utilization of Rehabilitation Programmes on Needy Inpatients in University of Maiduguri Teaching Hospital Borno State, Nigeria, Education, Vol. 9 No. 2, 2019, pp. 23-29. doi: 10.5923/j.edu.20190902.01.
Article Outline
1. Introduction
- Rehabilitation is a special area of health care that aims to provide function and or prevent deterioration of function to bring about the highest possible level of independence, physically, psychologically, socially and economically to maximize quantity of life and minimize the long term health care need and community support of these people [1]. According to Canadian working group (http://www.hivandrehab.ca), rehabilitation is the development of a person to the fullest physical, psychological, social, vocational and educational potential consistent with his/her physiological or anatomic impairment and environmental limitation.These definitions captured the many life domains for any medical condition and environmental constraint that may affect a needy patient. The definition frame rehabilitation activities to include many activities directed at improving all aspect of life or well-being of those living with medical conditions. The definition include within the range of activities performed that can link rehabilitation activities and services directly to the body requirements, activity limitations and participation restriction in order to connect the function of rehabilitation to various service dimension.The word rehabilitation in French translation is “re insertion sociale” meaning social re- insertion (https://wikipedia.org/rehabilitation). The word social insertion captured a fundamental aspect of the rehabilitation process “return to active living and participation in the society”. The main purpose of rehabilitation is to regain and maintain the level of function possible to needy in-patients. Rehabilitation in this sense helps the needy patient to live a normal life and interact freely in his/her environment. The incidence of diseases calls for many to seek for hospital services. The incidence of pronounced high poverty index especially in the north east region of Nigeria in which Borno State is situated have caused many not to seek the hospital services. Those who are able to seek the hospital services may be unable to afford the hospital bills while still in the hospital. These groups of inpatients who along the line are unable to afford the hospital services are those this study refers to as needy in patients. In most cases they are being identified by the doctors and nurses in charge of the wards. The purpose of this study is to assess the utilization of rehabilitation on needy in-patients in University of Maiduguri Teaching Hospital, Borno state, Nigeria. The study therefore hypothesized that there is no significant difference in utilization of rehabilitation programmes among needy in-patients across the ward.
1.1. Rehabilitation Programmes
- Rehabilitation programmes are designed to equip people with severe and enduring mental illness with the skills they need to live more independently (Survey and Borders Partnership NHS Foundation Trust 2016). According to Healthcare.gov (http://www.healtcare.govblog), rehabilitation services are health care services that help keep, get back or improve skills and functioning for daily living of a patient that have lost or impaired due to sick, hurt or disabled. In other words the rehabilitation services are given to repair bring back to normal what must have been damaged by illness and injury.According to Barry, Matika and Jerry [2] rehabilitation includes a range of services, programmes and policies that intend to provide solutions to many issues such as:(1) Addressing impairment, activity limitation and participation restriction or side effect of medication(2) Managing treatment side effects, supporting, integration of often complex treatments regimens into daily activities and tolerating treatment without increasing toxicity(3) Staying at, or returning to employment or volunteer work(4) Improving health and participation in society(5) Improving self- esteem, maintaining interpersonal relationshipAccording to Rehabilitation Organization [3] rehabilitation programme varies based on the patients’ requirement. Each patient needs personal attention and rehabilitation is given based on his/her needs. For example, inpatient rehabilitation in requires utilizing interdisciplinary approach to help people regain function, become as independent as possible and return to community setting (Hopkins, 2015).
1.2. Utilization of Rehabilitation Programmes
- Discussing the importance of rehabilitation in cancer treatment, Japanese Journal of Clinical Oncology [4] stated that rehabilitation can be applied throughout the entire phase from the time of diagnosis to the terminal stage. The approach has been a means of supporting the hopes of needy patients and their families which help to maintain and improve the quality of life. According to Wadell and Burton [5] rehabilitation programme helps patients recovering from serious injury illness, psychological problem to regain their strength and or mobility and finding way of doing things ultimately functioning relearns skills with the highest possible level of independence in their community choice.To support the view that rehabilitation helps to improve quality of life of patients, Korstjens, Mesters, Gijien and Van [6] conducted a study on quality of life of cancer survivors after physical and psychological rehabilitation. A twelve weeks rehabilitation group programme for all types of patient was organized combining physical exercise and psycho education. These group was tested in a longitudinal cohort study (n=658). Before the rehabilitation programme, participant reported a low quality life measured by the European organization for research and treatment of cancer (EORTC). Questionnaire tagged quality of life questionnaire (QLQ) was used to collect the data for analysis. The patient while still receiving the therapy recorded a significant improvement in all area. At the end of the programme the result revealed that there was a significant improvement on all outcome variables. In global quality of life (from 63.0 to 71.9), emotional function (from 66.2 to74.4), cognitive functioning (from 70.5 to 74.4) and fatigue level (reduction from 49.8 to 41.8) while, non-breast cancer patient showed clinically relevant improvement in physical functioning (from 67.3 to 80.4) and social functioning (63.4 to 79.4) and no worker patient.Similarly, Victor, Nneoma and Franco [7] conducted a study on Knowledge and Opinion on Stroke Rehabilitation and outcome among patients in Bayelsa state, Nigeria. The study assessed the knowledge and opinion of nurses on stroke patients’ rehabilitation as well as rehabilitation outcome. The descriptive survey design was used to determine the knowledge and opinion of nurses on stroke patient’s rehabilitation. One hundred (100) nurses participated in the study. The study revealed that seventy-five percent (75%) of the nurses believed that they (nurses) have a role to play in stroke rehabilitation and seventy-eight percent (78%) of the nurses acknowledged to a great extent that rehabilitation is a key component of nursing management of stroke patients. In conclusion, adequate rehabilitation leads to better outcome.
1.3. Types of Rehabilitation
- There are various rehabilitation programmes. Each rehabilitation programme is given to patient based on the health condition. This is due to the fact that what works for one person may not be effective for another person. Some rehabilitation programmes utilize multiple approaches adjusting the balance and focus of these approaches as treatment progress. Though rehabilitation most of the time is typically thought in relation to drug and alcohol abuse, there are other areas that need rehabilitation such as court order rehabilitation for some type offenders, injuries, accident persons including those who may need assistance in reintegrating into society. The different types of rehabilitation includes.
1.3.1. Individual Rehabilitation Counselling
- Individual rehabilitation is the most common type of rehabilitation counselling treatment. The patient meets one on one with the counsellor. The purpose of counselling rehabilitation according to the (http://gooddrugguide.com 2016) is to explore the roots causes behind the health condition that required rehabilitation, to uncover the triggers or life stress that lead to the individual problem, to develop strategies that help Individual maintain sobriety, and to help the individual make better decision concerning his/her health.Literatures have revealed that when medication is combined with single therapy, it can help to improve the health status of a needy patient, a typical example is a report from Juvet, Elvasaas, Leivseth, Anker, Bertheussen, Falkmer, Fors et.al [8] on rehabilitation of breast cancer patient; an overview. The report explores literature to assess the effect of single treatment and combination of treatment with respect to improvement in physical functionality and psychological wellbeing. The study involved forty-six (46) randomized controlled trials. The investigated interventions were physiotherapy, different types of physical activity, different Psychosis interventions nutrition, complementary interviews and complex rehabilitation programme. The report indicated that physical activity after primary cancer treatment can increase quality of life and reduce fatigue. A study conducted by Beauchamp, Evans, Janaudis, Goldstein and Brooks [9] on systematic review of supervised programmes after pulmonary rehabilitation in individual with COPD. The aim of this systematic review was to determine the effect of supervised exercise programmes after primary PR on exercise capacity and health related quality of life (HROL) in individual with COPD. Randomized controlled trials of post rehabilitation supervised exercise programmes versus usual care for individuals with COPD were identified after searches of six data bases and reference lists of appropriate studies. Two reviewers independently assessed study quality standard mean differences (SMD) with 95% as were calculated using a fixed-effect model for measures of exercise capacity and HROL. Seven randomized controlled trials, with a total of 619 individuals with moderate to severe COPD were involved in the study. At 6-month follow up there was a significant difference in exercise capacity in favour of the post-rehabilitation interventions (SMD, -0.20: 95% Cl, -0.39 to -0.01).Similarly, Ory, Fabre, Gu, Pastorelli, Tardez, Marchat, Marque et.al [10] conducted a study on an individual rehabilitation programme evaluation by Parkinson patients and their physiotherapists. The purpose of the study was to evaluate the feasibility Parkinson disease (PD) rehabilitation programme based on each patient’s prevalent symptoms and to determine the effect of this program on patient’s quality of life as well as the level of patients and physiotherapist’s satisfaction with the program in collaboration with physiotherapist with expertise in PD, a physical medicine and rehabilitation physician. A physical therapy programme was elaborated based on the core area for physical therapy in PD: exercises were selected that tailored to each patient’s main impairments and proposed this selection to local physiotherapist for three months. Quality of life was evaluated with PDQ-39 at baseline and after three months of the individual physical therapy programme. Questionnaire was structured based on anonymous satisfaction and was filled by participant at the end of the programme. One hundred and three individuals with moderately advanced but clinically stable idiopathic PD were involved. At the end of the study, significant improvement was found for emotional well-being bodily discomfort and stigmas domain (p≤ 0.05). Most of the patients felt improved by the physiotherapy program.Furthermore, Alda, Cristina, Joana, Raquel, Dina and Daniela [11] conducted a study of family based psychosocial support and education as part of pulmonary rehabilitation in COPD: a randomized controlled trial. The aim of the study was to investigate the impact of a family based pulmonary rehabilitation (PR) programme on patients and family members’ coping strategies to manage COPD. Patient and family members were randomly assigned to family based (experimental) or conventional (control) PR. Exercise training were given to patients from both groups three times a week and psychosocial support and education once a week for twelve weeks. Both the patients and their family members attended the psychosocial support and education sessions. However in the conventional PR, family members were not allowed to participate. Patients and family members of both groups were assessed on how they are coping and their psychosocial adjustment to illness. Patients’ exercise tolerance, functional balance, muscle strength and health related quality of life was also measured. All measures were collected before and after the rehabilitation programme. The result revealed that forty two dyads participated (patients: FEV, 70.4%± 22.1% predicted) patients (p=0.48) and family members (p=.004). The result revealed that family based PR had significantly greater improvements in family coping than the control group.According to Bach [12] lives of many individual with severe disability and paralytic/restrictive conditions can be significantly prolonged and quality of life greatly enhanced through noninvasive or conservative rehabilitation interventions. These interventions are devised to maintain or improve individual’s orthopedic, pulmonary and functional status. The combination of orthopedic surgery and rehabilitation can reverse musculotendinous contractures and scoliosis. Thus, maintain optimal patient comfort and function. To achieve individual rehabilitation goals, Smith, Cardillo, Joseph Smith and Amezaga [13] also conducted a study on improvement scaling (Rehabilitation version): a new approach to measuring progress of patients in achieving their individual rehabilitation goals. The objective of the study was to accurate measurement of clinically relevant change in individual patients undergoing rehabilitation research and clinical. Rehabilitation should go hand in hand with medication in order to obtain the right result.
1.3.2. Family Rehabilitation Counselling
- When any member of a family is down with health condition, the immediate family members bear a great deal of the brunt. Family rehabilitation counselling becomes necessary for the members of his/her family to know about the health condition to learn how to deal more efficiently with the recovery of the patient and thus aid healing (http://gooddrugguide.com 2016). Michelle and Anita (2015) conducted a study on the needs of family members of stroke patients at the bedside during inpatient rehabilitation. The study involved twelve family members of stroke patients at a rehabilitation centre in Northern California healthcare delivery system. The study explored the needs of family members of stroke patients admitted to an acute inpatient rehabilitation hospital. Family members’ needs were determined through the use of the Family Needs Inventory (FIN) and qualitative semi structured interview. The data collected was analyzed using descriptive statistical analysis of the (FIN). The result revealed five unmet needs such as knowing what to expect at home, knowing what symptoms that can occur, knowing when to expect symptoms, having someone care about the health of the family member being informed about changes in treatment. The qualitative analysis of the semi-structured interviews also revealed five main thematic need categories: preparedness for discharge, a family-centre environment, caring for the family members, communication, trust and respect.In the same vein Janesks and Joyce (2009) also conducted a study on family involvement in the rehabilitation of a stroke patient (a case report) on a 72 year old female patient with right hemiplegia. The barthel index (BI) was used to evaluate the patient functional abilities. An inpatient rehabilitation programme was designed for the patient with contribution from the multi-disciplinary team including the family. The patient followed a routine daily programme receiving physiotherapy in the morning and repeating the same in the afternoon with family assisting her. The result revealed that her BI scores improved from 15 to 65 points and the self-expressed short term goals were achieved by the end of her rehabilitation.Similarly Elisabetta, Andre and Massimo [14] conducted a study on measuring family satisfaction with inpatient rehabilitation care. The purpose of the study was to investigate the psychometric characteristics of the questionnaire of the family members. Satisfaction about the rehabilitation (QFSR), a new questionnaire assessing the satisfaction of patient families with the in-hospital rehabilitation services that is the organizational procedure, medical treatment, relationship with nurses/other health workers and outcome. The QFSR of 13 items was administered to 1,2.26/F-60.4 percent, mean age = 57.4, SD 15 years family members of patients admitted to two units for inpatient rehabilitation, that is cardiovascular and neuromotor. The result revealed that confirmation factor analysis (CFA) confirmed the theoretical four-factor structure of questionnaire in a subsample of 308 respondent randomly selected from the sample SBX2 (61) = 57.4; p=0.61; RMSEA = 0.0; 90 percent Cl [0.0, 0.031], CFI=1.00). The remaining 708 respondent (393 relatives of cardiovascular unit inpatients and 315 relatives of neuromotor unit inpatient) were used to test measurement invariance between the groups of family members with patients in the two units. The configurable, scalar and strict factorial invariance provided a good fit to the data.Meanwhile Loupis and Faux [15] conducted a study on family conferences in hospital settings. A literature review was conducted with 23 articles highlighting problem areas within current practice and discussing the merits of existing approaches. The review provides insight into the ideal method of communicating and planning and identifies better uses of these opportunities.
1.3.3. Group Rehabilitation Counselling
- Group rehabilitation counselling is an opportunity for patients with a common health condition to meet. The group itself becomes a kind of support structure, offering care and love to the patients who are willing to share their own experiences. The meeting serves as an avenue to realize that they are not alone in their struggle against their health condition (http://gooddrugguide.com 2016, psychosocial counselling and social work 2009).Apart from single therapy, group rehabilitation has also been used to prove the effect of patient to patient contact in rehabilitation, Lemu [16] conducted a study on group rehabilitation. The aim was to investigate how cancer patients perceive satisfaction with a group rehabilitation (GR) intervention to evaluate its effect and to explore the extent which patients copy style (monitoring, blunting) modulate the effect of GR. The additional aim of the study is to investigate to what extent some aspect of health related quality of life (HRQOL) physical functioning (QOL). One year after diagnosis was predicted on the basis of medical, socio demographic and psychological data collected at diagnosis. The study involved patient (n=481) diagnosed with breast gastrointestinal or prostate cancer. They were randomly assigned to one of four alternatives.1. Individual support (IS).2. Group rehabilitation (GR)3. Combination of (IS) TO (GR)4. Standard care (SC)The entire patients were monitored for two years. The rehabilitation programme comprised eight weekly session and one boaster session after two months. The session dealt with information about cancer, treatment, nutrition, cognitive behavior therapy (CBT) light physical training and relaxation. The result revealed that physical and informative component were rated more beneficial by the patients. The result also proves that patient meeting with other patients with same/similar problem is also beneficial to the needy patients as they are not alone that there are others having the same problem like theirs.Similarly, Korstjens, Mesters, Gijien and Van [17]) conducted a study on quality of life of cancer survivors after physical and psychological rehabilitation. A twelve weeks rehabilitation group programme for all types of patient was organized combining physical exercise and psycho education. These group was tested in a longitudinal cohort study (n=658). Before the rehabilitation programme, participant reported a low quality life measured by the European organization for research and treatment of cancer (EORTC). Questionnaire tagged quality of life questionnaire (QLQ) was used to collect the data for analysis. The patient while still receiving the therapy recorded a significant improvement in all area. At the end of the programme the result revealed that there was a significant improvement on all outcome variables. In global quality of life (from 63.0 to 71.9), emotional function (from 66.2 to74.4), cognitive functioning (from 70.5 to 74.4) and fatigue level (reduction from 49.8 to 41.8) while, non breast cancer patient showed clinically relevant improvement in physical functioning (from 67.3 to 80.4) and social functioning (63.4 to 79.4) and no worker patient showed a clinically relevant improvement in role functioning (57 to 69.6). Kortjens, Mesters, Gijisen and Van [17] also conducted a study on cancer patient’s view on rehabilitation and quality of life: a programme audit. The objective of the study was to explore patients’ perspective on how and to what extent the rehabilitation programme met their need in order to optimize the programme. Patients that have participated in the similar programme five (5) years ago were interviewed in the three focused groups (n-23). Participant who received rehabilitation previously saw it as a stepping stone in their ongoing recovering process and identified the integrated physical training, psycho social sessions and patient to patient contact as a powerful and supportive combination. Patient that participated in the group based multi-modal cancer agreed and show that the rehabilitation programme has help in improving their health condition.Furthermore, Kalra, Dale, Crome [18] conducted a study on improving stroke rehabilitation; a controlled study. The study involved a prospective controlled study of two hundred and forty five (245) stroke patients that were divided into three (3) groups according to prognosis and managed on stroke rehabilitation unit (n=124) or general medical wards (n=121). These patients were randomly allocated to either setting two (2) weeks after stroke and were comparable for baseline characteristic. More physiotherapy was given to patients on general medical wards. Similar amount physiotherapy was also given to patients with stroke. More time was spent on individual rehabilitation on those in stroke unit than those in general ward. In both setting, functional abilities at discharge, destination of discharge and length of hospital stay in patients with good prognosis were compared. The result revealed that patients grouped with intermediate prognosis had significantly better outcome on the stroke unit, as more patients were discharged.Mbada, Ayanni, Ogunlade, Orimolade, Oladiran and Ogundele [19] conducted a study on Rehabilitation of Back Extensor muscles’ inhibition in patients with long-term mechanical low-back pain. The study investigated the effect of static or dynamic back extensors endurance exercise in combination with McKenzie Protocol (MP) in patients with long term mechanical low-back pain (LMLBP). This randomized controlled trial involved eighty four (84) patients who were assigned into MP Group (MPG), MP plus Static Back Extensor’s Endurance (SBEE), Exercise Group (MPSBEEG) or MP plus Dynamic Back Extensor’s Endurance (DBEE) and Exercise Group (MPDEEG). Twenty five (25), twenty two (22) and twenty (20) participants in MPG, (MPSBEEG) and (MPDBEEG) respectively completed the trice weekly eight week study. The result revealed that MP alone, or in combination with SBEE or DBEE exercise was effective in the rehabilitation of back extensor’s endurance and fatigability in patients with LMLBP. However, the addiction of SBEE to MP led to higher significant positive effects.Meanwhile Nor, Noor, Aznida, Devinder, Nor, Saperi and Syed [20] conducted a study exploring views on long term rehabilitation for people with stroke in a developing country; findings from focus group, discussion. The study explored the perception of rehabilitation professionals with stroke towards long term stroke rehabilitation services and potentials approaches to enable provision of these services, views from providers and users are important in ensuring whatever strategies developed for long term stroke rehabilitations are feasible and acceptable. Focus group discussions were conducted. The group discussion involved 15 rehabilitation professionals and eight long term stroke survivors. Family-assisted home therapy was viewed as a potential approach to continued rehabilitation for long term stroke survivors, given careful planning to overcome several family-related issues.
2. Methodology
- The descriptive survey design was used in this study to assess the utilization of rehabilitation programme on needy in-patients in University of Maiduguri Teaching Hospital Borno State. The populations for this study included those patients hospitilised in the University Teaching Hospital in Maiduguri who did not have means of paying their hospital bills hospital due to poverty. Two hundred and fifty eight (258) such patients were identified by the hospital management. Eight (8) hospital departments/wards were involved in the study, they are pediatrics, male medical, male surgical, female surgical, gynecology and obstetrics, accident and emergency (A&E) ear, nose, and throat, (ENT) and the orthopedic wards.A 31-item Questionnaire was used to collect the data. The data collected was analyzed using frequency and percentage score while the hypothesis was tested using chi-square at the confidence level of 0.05. According to Kerlinga and Lee (2002) chi square is suitable for analyzing data that is nominal which seek to establish the observed and obtained scores and variables.
3. Data Analysis, Results and Discussion
|
|
|
4. Discussion
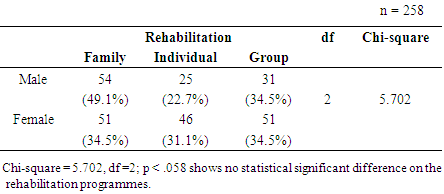
- The study examined the rehabilitation programmes employed by the University Teaching Hospital Maiduguri, Borno State, Nigeria in rehabilitating patients with diverse health conditions. The hospital has rehabilitation programmes meant to care for the patients whose conditions are critical and could not foot their hospital bills unassisted. Most times such patients are usually abandoned by the relations who bring them into the hospital due to lack of money to pay for the hospital bills. Although many spirited individuals, non-governmental organisations and religious bodies often come to the help of such patients, their prolong hospitalization requires that the hospital through its units of social welfare assist them to get treatment and feeding while they are on admission.In this regard, different rehabilitation methods are employed to ameliorate the suffering of the patients. For example, in this study, 105 inpatients received family rehabilitation; this number represents 40.7 percent of the patients. This rehabilitation seemed to be most favoured by both the hospital management and patients. According to Kortjens, Mesters, Gijisen and Van [17] rehabilitation help patients to improve on their emotion, function, cognitive functioning and level of fatigue. Waddell and Burton [5] posited that rehabilitation helped patients to regain their strength with possible independence without being a liability to their families and society at large. This in fact, reveals why the hospital consistently employs the family rehabilitation programme for the patients. It appears that the individual rehabilitation was not given to patients most often. Perhaps that explains why only 71 patients representing 27.5% were given individual rehabilitation. In Africa the family values and support remains major concern as such what affects an individual affects the whole family. Furthermore, the study revealed that 31.8% of the patients received Group rehabilitation in the hospital. It appears too that the hospital employed this method to handle large number of patients who have similar conditions for example the HIV/AIDs group counselling and rehabilitation. In the recent past, literature regarding cost effectiveness analysis has dominated public discourse by rehabilitation scientists. For example, Aprille, Rizzo, Romanini De Santis, Marsan, Rinaldi and Padau [21] compared the effectiveness of group and individual rehabilitation and reported that group rehabilitation is efficient as individual rehabilitation for certain inpatients.Examining the types of rehabilitation used by the hospital, the study revealed that no statistical significant difference was shown among the three rehabilitation programmes; family, individual and group rehabilitations. The prevailing condition of the patients may have made this observation possible. Because of the concern of every patient is to get well and leave the hospital bed as soon as the rehabilitation programme can afford him or her. However, the data on family and group rehabilitation attest to the fact that the two programmes are favoured by the management due to cost effectiveness and man-effort required.
5. Conclusions/ Recommendations
- On the basis of the findings of this study it is therefore concluded that family and group rehabilitation programmes were favoured by the hospital rehabilitation staff. The inpatients on the other hand showed that both rehabilitation programmes are convenient for them. However, the individual rehabilitation programme also received attention by the hospital staff where populations of patients needing rehabilitation are few.Owing to the inherent benefits of individual rehabilitation programme, this paper suggests that the hospital management should maximize its use. The hospital should as a matter of necessity provide the appropriate facilities for hospital rehabilitation programmes because most patients do not have the satisfaction of being clumped with others while receiving the counselling.