-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Education
p-ISSN: 2162-9463 e-ISSN: 2162-8467
2014; 4(6): 160-166
doi:10.5923/j.edu.20140406.05
The Effect of Common Teaching Tools on Upper Extremity Muscle Activity
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLCarlos Zerpa, Natalie Lopez, Eryk Przysucha, Paolo Sanzo
Lakehead University, School of Kinesiology, City, Canada
Correspondence to: Carlos Zerpa, Lakehead University, School of Kinesiology, City, Canada.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Excessive muscle activation and repetitive movements of the upper extremities while using teaching tools in the classroom (e.g., whiteboard, PowerPoint, or both) may result in muscular fatigue and increased risk of injury. Based on these concerns, the aim of this study was to examine upper extremity muscle activation levels associated with classroom teaching tools and develop appropriate recommendations for teachers to minimize the risk of injury. Eighteen participants, 18 to 30 years of age were asked to teach a lesson using different teaching tools (e.g., whiteboard, PowerPoint, or both). Muscle activation was measured using surface electromyography on the upper and middle trapezius, infraspinatous, and anterior deltoid for each teaching tool. The data were analyzed using two way repeated measures ANOVA. Inferential statistics revealed an interaction effect between teaching method and muscle type, F (2, 15) =4.861, p<0.05,  =.247in relation to muscle activation. The interaction effect indicated that using the whiteboard as a teaching tool increased the level of muscle activity. On the contrary, when using PowerPoint as a teaching tool, all muscle groups converged producing a low level of muscle activity. When using both teaching methods combined (whiteboard and PowerPoint), however, a moderate effect on muscle activation levels was obtained. The outcome of this study can be used as an avenue to provide recommendations for teachers to minimize the risk of injuries in the upper extremities by using alternating teaching methods (whiteboard and PowerPoint combined). Future research should explore other teaching tools (e.g., smart boards) in relation to muscle activation levels. Future research should also explore preventative methods and the development of rehabilitation techniques to help teachers recover from overuse injuries caused by the various teaching and instructional tools.
=.247in relation to muscle activation. The interaction effect indicated that using the whiteboard as a teaching tool increased the level of muscle activity. On the contrary, when using PowerPoint as a teaching tool, all muscle groups converged producing a low level of muscle activity. When using both teaching methods combined (whiteboard and PowerPoint), however, a moderate effect on muscle activation levels was obtained. The outcome of this study can be used as an avenue to provide recommendations for teachers to minimize the risk of injuries in the upper extremities by using alternating teaching methods (whiteboard and PowerPoint combined). Future research should explore other teaching tools (e.g., smart boards) in relation to muscle activation levels. Future research should also explore preventative methods and the development of rehabilitation techniques to help teachers recover from overuse injuries caused by the various teaching and instructional tools.
Keywords: Teaching Tools, Muscle Activation, Upper Extremity, Shoulder and Back Pain
Cite this paper: Carlos Zerpa, Natalie Lopez, Eryk Przysucha, Paolo Sanzo, The Effect of Common Teaching Tools on Upper Extremity Muscle Activity, Education, Vol. 4 No. 6, 2014, pp. 160-166. doi: 10.5923/j.edu.20140406.05.
Article Outline
1. Introduction
- In the teaching profession, the majority of research studies related to upper extremity injuries have focused primarily on cross-sectional surveys to gain insight on teacher perception of upper extremity risk factors related to teaching [6, 10]. Korkmaz, Cavlak, and Telci (2011) conducted a cross-sectional survey on 900 full-time teachers in Turkey. The researchers found that 463 teachers had musculoskeletal pain and that 59.4% of the sample was female. In addition, from the sample of 463 teachers who reported musculoskeletal pain, 42.5% had neck pain and 36.9% had upper back pain. The researchers also found that 71.1% of the teachers reported that standing for long periods of time increased or caused upper extremity pain. da Silva and Almedia (2012) also used a cross-sectional survey to report on teacher upper limb discomfort associated with repetitive overhead movements such as when writing on a whiteboard and found that 14.1% of females and 6.2% of males reported having discomfort. While researchers used cross-sectional surveys to gain a better understanding of teacher upper extremity discomfort and pain in the teaching profession, the effect of teaching tools (e.g., whiteboard, PowerPoint, or both) on shoulder muscle activation levels has not been extensively investigated. Consequently, teachers lack information on the appropriate use of teaching tools in the classroom to minimize the risk of upper extremity overuse injuries when delivering a teaching lesson [6, 10]. As Antony and Keir (2010) stated, when writing on a whiteboard, the teacher needs to maintain a gripping action with the shoulder flexed to greater than 90 degrees, which results in an increased shoulder moment. The increased shoulder moment causes the activation levels of the trapezius and deltoid muscles to be redistributed to the infraspinatous and supraspinatus muscles to stabilize the glenohumeral joint throughout the hand movement [2, 4]. Since the infraspinatous and supraspinatus are smaller rotator cuff muscles, they generate high intramuscular pressure and manifest early signs of fatigue in comparison to the larger shoulder muscles (i.e., trapezius, deltoid) [8]. Subsequently, the muscular fatigue may result in harmful loading of the glenohumeral joint increasing the chance of rotator cuff injury [2, 12]. In the teaching profession, however, shoulder pain has been attributed mostly to sustained arm elevation when writing on the board, which over time has the potential to cause rotator cuff injury [2, 12, 14]. That is, prolonged arm elevation can cause mechanical impingement of the subacromial tendons and bursa, reduce blood flow to the rotator cuff region, and result in secondary upper extremity injuries due to compression of other vessels and nerves in the cervical and brachial plexus regions [11, 15].Shoulder pain and rotator cuff injuries can also originate from excessive activation of larger shoulder muscles (e.g., trapezius, deltoid, pectorals) when performing prolonged arm elevation movements such as writing on the board. These muscles may then be required to function in an alternate capacity altering the normal force couple in the scapular region, changing the normal patterning, and completion of the motion. In the case of trapezius muscle activation levels, for example, all three muscular divisions (i.e., upper, middle, and lower) responsible for shoulder and thoracic spine movements must work in coordination and time sequentially to elevate and control scapular motion at varying degrees when writing on the board [7]. That is, the upper trapezius muscle elevates the lateral clavicle to contribute to scapular external rotation and upward rotation, while the middle trapezius controls the axis of rotation for the shoulder as the person writes on the board [7]. The lower fibers of trapezius, however, maintains a constant length to control the axis of rotation, upward scapular rotation, and assists in preventing unwanted protraction of the scapula [7]. The coordination and timing of all three divisions of the trapezius muscle are necessary for optimal and painfree shoulder elevation and scapular control when writing on the board. If muscle over activation is induced in the trapezius for prolonged periods of time, however, it may lead to an altered force couple, muscular fatigue, and possible impingement resulting in shoulder pain and injury [7].There are also upper extremity injuries that can be associated with prolonged use of PowerPoint as a teaching tool. Some of these injuries can be linked to teachers' poor postural habits such as forward head positioning [5, 9, 10, 13, 18, 19]. According to Weon et al., (2010), a forward head posture in a standing position increases the muscle activation of the upper and lower trapezius, resulting in neck and shoulder pain, due to over muscle activation and changes in cervical and scapular kinematics. Zakharova-Luneva, Jull, Johnston, and O’ Leary (2012) found that upper limb pain correlated to muscle activation changes in the upper, middle and lower fibers of trapezius when performing repetitive movements of the arms, while in a standing position. Other researchers also found that when the trapezius muscles were exposed to daily, repetitive, and sustained low-level activity, it resulted in an overload of muscle fibres of low-threshold motor units, potentially causing trapezius myalgia, which is a chronic pain in the upper trapezius [1]. One approach to minimize potential risks resulting from excessive activation of the upper extremity musculature in the teaching occupation may be to implement activities in the classroom that require the use of teaching tools intermittently (e.g., whiteboard and PowerPoint). As stated by Balasubramanian, Adalarasu, and Regulapati (2009), stationary standing for extended periods of time results in decreased blood flow to the muscles, accelerated onset of muscle fatigue, and pain in the cervical and lumbar muscles. The pain usually worsens when the person assumes a poor posture [18]. This finding seems to indicate that the use of just one tool (either a whiteboard or PowerPoint) to deliver a teaching lesson may potentially result in injury over time due to the repetitive sequential movements and continued muscle contractions.Based on the concerns stated in the literature, the purpose of this study was to examine the levels of muscle activation in the upper extremity associated with different teaching tools to gain a better understanding of which tools may potentially have an adverse effect on teacher upper extremity muscles. The question driving this study was:What effect do teaching tools (e.g., whiteboard, PowerPoint or both) have on the upper extremity muscle activity (i.e., upper and middle trapezius, infraspinatous, and anterior deltoid muscles) when delivering a teaching lesson?
2. Method
2.1. Participants
- This study recruited 18 healthy participants, 9 males and 9 females. The participants were students enrolled in either the Concurrent Education program or professional year of Teachers’ College at Lakehead University due to their experience with teaching a lesson. The participants were between 20 to 30 years of age, and did not have any previous upper extremity injuries or pain. The participants filled out a Physical Activity Readiness Questionnaire (PAR-Q) to determine their health status. The participants also completed three additional eligibility forms to further determine any pain, discomfort, or injuries on the muscles being examined. If any of these symptoms were present, participants were excluded from the study.
2.2. Instruments
- A Delsys dipole electromyography (EMG) instrument with eight input channels was used to measure the muscle activities for the upper and middle trapezius, infraspinatous, and anterior deltoid muscles. The Delsys EMG instrument was interfaced with an ADinstrument Technologies Power Lab unit and software to read the raw EMG signal for each muscle. Adhesive bipolar surface EMG electrodes sensors were connected to each participant muscle group and the signal was fed into the Delsys EMG amplifiers that were linked to the ADinstrument Power Lab Unit. There were a total of two amplifiers, four electrodes, and two grounds used on each participant. The two amplifiers were hooked to a belt that the participant attached to his/her waist. A lesson plan on the solar system was provided to each participant. The participant was asked to deliver the lesson plan for each teaching trial using either a whiteboard, PowerPoint, or both as teaching tools. The solar system lesson was selected because participants reported to be more familiar with this topic. The lesson plan was provided as a hard copy for the trials involving the use of the whiteboard and in digital format for the trials involving the use of PowerPoint. A 54 inch Panasonic television set was used to display the PowerPoint slides.
2.3. Procedure
- Participants were asked to come to the Multipurpose Research Laboratory at Lakehead University during the day of the testing. Before administering the testing protocol, participants filled out and signed a consent form, eligibility questionnaire, and PAR-Q. After completing and signing the required information, participants were asked to identify their dominant hand. The researchers administering the testing protocol began preparing the participants’ dominant hand by cleaning the skin with alcohol wipes on the areas where the electrodes would be placed. The Surface ElectroMyoGraphy for the Non-Invasive Assessment of Muscle (SENIAM) technique (1999) was used as a reference for location of the surface electrodes on the participant trapezius (upper and middle fibers) and anterior deltoid muscles. To identify the location for the upper trapezius, the surface EMG electrode was oriented in line with the acromion and C7 spinous process and then positioned in the middle of these two locations. For the middle trapezius, the surface EMG electrode was placed between the medial border of the scapula and spinous process of T3 in the direction of a line between the T5 spinous process and the acromion. For the anterior deltoid, the surface EMG electrode was positioned, one finger width distal to the acromion. For the infraspinatous, however, the surface EMG electrode was positioned over the infrascapular fossa, 4 cm parallel to the spine of the scapula based on the research work of Waite, Brookham, and Dickerson (2010). The researchers also identified the locations to place the Delsys EMG instrument grounds on the participant upper extremity. The researchers insured that the grounds remained in complete contact with the participant skin to reduce the chance of open ground noise. Two locations were identified on the participant to place the ground electrodes for each Delsys EMG instrument. The first ground electrode was positioned on the participant’s C7 spinous process and the second ground electrode was placed on the non-dominant pisiform bone of the wrist. After the surface EMG electrodes and grounds were positioned on the appropriate locations, the participants were asked to put a belt around his/her waist and the two Delsys EMG instruments were attached to the belt. The participants were asked to perform a variety of exercises to ensure that surface EMG electrode sensors were reading information from the correct muscles before commencing the testing protocol. These exercises included a standing row with arms raised forward and laterally, external rotation of the arm, and shoulder shrugs. To maintain consistency across EMG electrode placement for each subject, the electrodes were labeled from numbers 1 to 4 and placed on the same muscles for each participant. That is, middle trapezius muscle activity was always read from electrode 1, infraspinatous from electrode 2, upper trapezius from electrode 3, and anterior deltoid from electrode 4. Once the muscle activity was detected for each muscle, the participants performed three trials to deliver a teaching lesson. For the first trial, the participants were provided with a hard copy of the lesson plan and were asked to write a few lines from the lesson plan on a whiteboard. Participants were given the option to either hold the hard copy of the lesson plan with his/her non-dominant hand or lean the hard copy on the ledge of the whiteboard. Once the participants felt comfortable with the marker in his/her hand, he/she was instructed to begin writing on the whiteboard and stay within the length of the whiteboard, as depicted in Figure 1. EMG muscle activation data were collected for one minute, via the Delsys EMG system. After completing the trial, participants were provided with a one minute rest. For the second trial, participants were instructed to stand from a set location, perpendicular to a television monitor, which was displaying the PowerPoint teaching lesson as depicted in Figure 2. Participants were encouraged to use his/her hands and arms in a similar fashion as he/she would in the classroom settings when delivering a PowerPoint lesson using PowerPoint. The number of slides completed when delivering the PowerPoint lesson depended on the speed of participants’ speech. EMG muscle activation data were collected for one minute. After the data collection was completed, participants were provided with a subsequent one minute rest break.
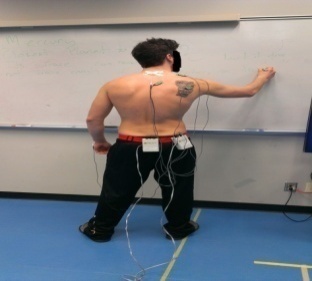 | Figure 1. Whiteboard trial |
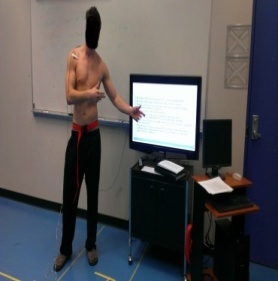 | Figure 2. PowerPoint trial |
2.4. Data Analysis
2.4.1. Signal Processing
- A power spectrum analysis was conducted to determine the cutoff frequency of the signals. The cutoff frequency of the EMG signals ranged from 6 to 7 Hz. After each signal cutoff frequency was determined, the raw EMG signal was rectified using a mathematics absolute value function. A 10 Hz low pass filter was applied to the rectified signal to eliminate any high frequency noise that could potentially interfere with the EMG readings. The average EMG from each rectified signal was computed.
2.4.2. Statistical Analysis
- Descriptive statistics were used to compare means and standard deviations of the rectified average EMG signals for each teaching tool and muscle group. Two independent variables were examined (muscle type and teaching methods) and one dependent variable (EMG muscle activity). To answer the research questions, a two way repeated measures ANOVA was conducted to examine the interaction effect between muscle groups and teaching tools in relation to EMG muscle activity. Bonferroni pair mean comparisons were conducted to determine differences between muscle group activation levels, as well as, differences between teaching methods in relation to muscle activity levels.
3. Results
- Descriptive statistics as depicted in Figure 3 and Figure 4 revealed that for the whiteboard teaching method, the deltoid (M = .096, SD = .014), upper trapezius (M = .044, SD = .035), middle trapezius (M = .018, SD = .014) and infraspinatous (M = .016, SD = .012) exhibited higher EMG muscle activation levels than the muscle activation levels produced by the deltoid (M = .008, SD = .003), upper trapezius (M = .011, SD = .004), middle trapezius (M = .005, SD = .003), and infraspinatous (M = .003, SD = .001) when using PowerPoint as a teaching method. Similarly, as depicted in Figure 3 and Figure 5, the whiteboard teaching method exhibited higher EMG muscle activation levels than the muscle activation levels produced by the deltoid (M = .037, SD = .019), upper trapezius (M= .026, SD= .013), middle trapezius (M= .008, SD= .004), and infraspinatous (M=.008, SD=.004) when using both teaching methods combined.
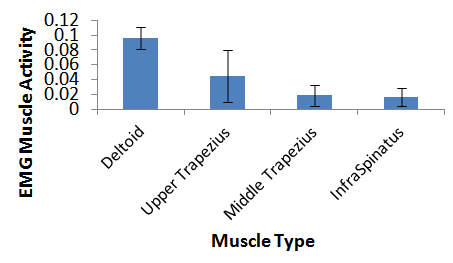 | Figure 3. Muscle activity level for the whiteboard teaching method |
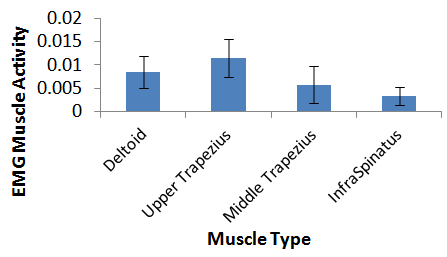 | Figure 4. Muscle activity level for PowerPoint teaching method |
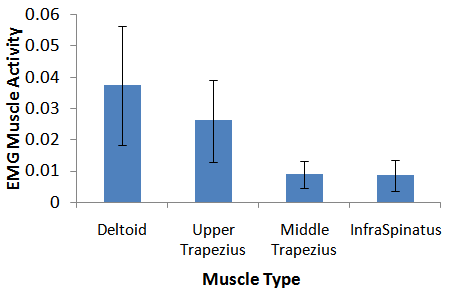 | Figure 5. Muscle activity level for both teaching methods combined |
 =.247. To provide evidence of the statistical reliability of the sample size in representing the population, a power of analysis was conducted to compute with how much power the null hypothesis was rejected. The observed power of rejection was found to be .97. Since the power level is higher than .80 and the interaction effect size is large, the sample has evidence of statistical reliability in representing the population to identify the effect of teaching tools on muscle type EMG levels. As depicted in Figure 6, there was a higher effect on muscle type EMG levels when using the whiteboard. Muscle type EMG levels, however, seemed to converge with a low level of muscle activity when using PowerPoint as a teaching tool. When using both teaching tools combined (whiteboard and PowerPoint), a moderate muscle EMG activation level was obtained for each muscle type. The Bonferroni mean comparisons revealed that the deltoid and upper trapezius muscle activity levels were significantly higher than the middle trapezius and infraspinatous activation levels for all teaching methods. The Bonferroni mean comparisons also revealed that the teaching methods were significantly different from one another in terms of muscle activation levels.
=.247. To provide evidence of the statistical reliability of the sample size in representing the population, a power of analysis was conducted to compute with how much power the null hypothesis was rejected. The observed power of rejection was found to be .97. Since the power level is higher than .80 and the interaction effect size is large, the sample has evidence of statistical reliability in representing the population to identify the effect of teaching tools on muscle type EMG levels. As depicted in Figure 6, there was a higher effect on muscle type EMG levels when using the whiteboard. Muscle type EMG levels, however, seemed to converge with a low level of muscle activity when using PowerPoint as a teaching tool. When using both teaching tools combined (whiteboard and PowerPoint), a moderate muscle EMG activation level was obtained for each muscle type. The Bonferroni mean comparisons revealed that the deltoid and upper trapezius muscle activity levels were significantly higher than the middle trapezius and infraspinatous activation levels for all teaching methods. The Bonferroni mean comparisons also revealed that the teaching methods were significantly different from one another in terms of muscle activation levels. 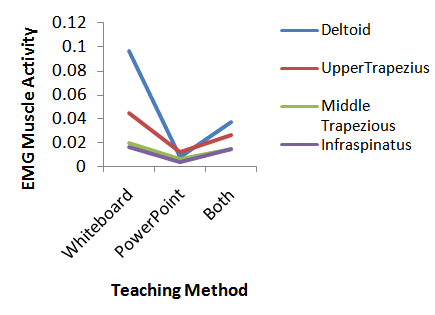 | Figure 6. Interaction effect of teaching tools and muscle type in relation to muscle activity |
4. Discussion
- The outcome of this study revealed a significant interaction effect between teaching methods and upper extremity muscle type in relation to EMG muscle activity. The use of the whiteboard, for example, produced the highest muscle activation levels for the deltoid and upper trapezius muscles. This finding supports the research work of Antony and Kleir (2010), which stated that when writing on the board, there is an increased shoulder moment causing higher muscle activation levels in larger shoulder muscles (i.e., deltoid and trapezius). The issue, however, is that if this action is performed for long periods of time, it has the potential to produce adverse effects in the upper extremity related to possible abnormal coupling, scapular malpositioning, superior and/or anterior migration of the humerus, resulting in possible rotator cuff injury and shoulder pain. As stated by Falla et al., (2007) in the teaching profession, shoulder pain and rotator cuff injury can potentially originate from excess activation of larger shoulder muscles (e.g., trapezius, deltoid, pectorals) when performing prolonged shoulder elevation movements such as writing on the board. The results of the current study also revealed that the middle trapezius and infraspinatous muscles produced the lowest muscle activation levels when writing on the whiteboard. Although this movement was only performed for one minute, the concern is that writing on a whiteboard for long periods of time may cause smaller rotator cuff muscles (i.e., infraspinatous) to develop early signs of fatigue, increasing the chance of teacher upper extremity injury. As stated in the literature, upper extremity muscle fatigue can result in a harmful loading of the glenohumeral joint increasing the possibility of a rotator cuff injury [2, 12]. In addition, sustained arm elevation for long periods of time has been found to cause mechanical impingement of the subacromial tendons, a reduction in blood flow to the rotator cuff muscles, and an increased chance of upper extremity injury including full thickness tearing of the rotator cuff musculature or tears of the glenoid labrum [11, 15].Similarly, when using PowerPoint as a teaching tool in the current study, the upper trapezius and deltoid muscles produced the highest level of muscle activation when compared to the other muscles (i.e., middle trapezius and infraspinatous). When compared to the other teaching tools (i.e., whiteboard and combined teaching methods), however, the upper trapezius and deltoid muscles produced a significant lower level of muscle activation. Some of the high muscle activation levels for the deltoid and upper trapezius muscles when using PowerPoint may be attributed to sustained shoulder flexion movements and forward head positioning due to participant’s posture. While the levels of muscle activity were lower for all muscles when using PowerPoint as compared to other teaching tools (i.e., whiteboard or both), the risk of using just one single teaching tool for long periods of time (e.g., PowerPoint) is that teachers may develop poor postures, which consequently can lead to upper extremity neck and shoulder pain. As stated by Weon et al., (2010), a forward head posture in a standing position increases the muscle activation of the upper and lower trapezius, resulting in neck and shoulder pain, due to over muscle activation and changes in scapular kinematics. In the current study, the use of both teaching methods in combination produced a significant moderate level of muscle activation for all muscle groups. The muscle activation levels for the use of both teaching methods in combination were significantly higher than the use of PowerPoint alone and significantly lower than the use of the whiteboard alone. The use of both teaching methods in combination seems to provide an avenue for teachers to minimize the risk of upper extremity injuries related to muscle overexertion.
5. Conclusions
- The purpose of this study was to examine the levels of muscle activation in the upper extremity associated with different teaching tools to gain a better understanding of which tools could potentially have an adverse effect on teachers resulting in possible upper extremity dysfunction, pain, and/or injury. The outcome of this study revealed that the use of teaching tools intermittently seems to offer an avenue to help teachers prevent poor sustained static postures that may result in high levels of muscle activation in the shoulder region, which can potentially lead to neck and shoulder dysfunction and pain. As stated by Balasubramanian, Adalarasu, and Regulapati (2009), sustained standing positions may decrease blood flow to the muscles, accelerate the onset of muscle fatigue, and cause neck and low back pain. In addition, it is also stated in the literature that in the teaching occupation, shoulder pain and rotator cuff injuries can potentially originate from excess activation of larger shoulder muscles (e.g., trapezius, deltoid, pectorals) when performing prolonged shoulder elevation movements such as writing on the board [7]. In summary, the outcome of this study supports the literature and provides an alternative approach to minimize the risk of upper extermity injuries in the teaching occupation.Some of the limitations of this study, however, relate to sample size. With a larger sample size, it may be possible to make stronger generalizations to the population of teachers in regard to the intermittent use of teaching tools to minimize the risk of upper extremity injuries. Another limitation is the effect of cross talk on the surface EMG readings. That is, the effect of muscle activity from adjacent muscles on the intended EMG readings, which poses a validity concern when assessing the muscle activation levels for specific muscle groups (i.e., deltoid, upper and middle trapezius, and infraspinatous). In the current study, however, the effect of cross talk on the comparison of teaching methods was factored in by keeping the same electrode placements on the participant shoulder muscles when measuring the EMG activity across teaching methods.Future research studies should focus on the use of indwelling electrodes to more accurately measure the level of muscle activity for deep rotator cuff muscles (i.e., supraspinatus, infraspinatous) and minimize the effect of crosstalk. Future research studies should also include the use of wireless EMG electrodes to assess in service teachers’ level of muscle activity while teaching in the classroom to provide recommendations to teachers for the use of teaching tools intermitently. More specifically, future research should aim at developing appropriate prevention strategies and muscle rehabilitation protocols to help teachers recover from muscle injuries caused by the overuse of teaching methods.
ACKNOWLEDGEMENTS
- The researchers would like to thank the participants who partook in the study.