-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Education
p-ISSN: 2162-9463 e-ISSN: 2162-8467
2014; 4(2): 35-40
doi:10.5923/j.edu.20140402.04
Validating the Effects of Inclusive Childcare with the Interaction Rating Scale
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAnme T.1, Tanaka E.1, Sugisawa Y.2, Matsumoto M.3, Watanabe T.4, Tomisaki E.5, Tokutake K.1, Miyazaki K.6, Edamoto S.6
1Faculty of Medicine, University of Tsukuba, Ibaragi, Japan
2UsyukuCity, Ibaragi, Japan
3Futaba Nursery, Tokyo, Japan
4Faculty of Nursing, Ashikaga University, Tochigi, Japan
5Sofia University, Tokyo, Japan
6Rokokan, Osaka, Japan
Correspondence to: Anme T., Faculty of Medicine, University of Tsukuba, Ibaragi, Japan.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
This study aimed to validate the effects of inclusion in center-based childcare, focusing on the inclusion of children with disabilities. One hundred thirty-eight 3 to 12-year-olds participated in this study. Participants were required to complete a 5-minute interaction session and were evaluated using the Interaction Rating Scale between Children (IRSC) as an evidence-based practical index of social skills. Significantly higher IRSC self-control scores were observed in interactions between typically developing children and children with disabilities than in normal children pairs. Additionally, behaviors reflecting the IRSC items, “explains his/her opinion logically” and “explains his/her opinion based on the level of competence/ability of the partner” were more frequently observed in interactions involving peers with disabilities than in those involving only typically developing peers. These results suggest that inclusive childcare may be effective in enhancing child social competence, especially self-control and flexibility/adaptability, depending on interaction partners’ needs for care.
Keywords: Inclusion, Interaction, Peer, Evaluation, Scale
Cite this paper: Anme T., Tanaka E., Sugisawa Y., Matsumoto M., Watanabe T., Tomisaki E., Tokutake K., Miyazaki K., Edamoto S., Validating the Effects of Inclusive Childcare with the Interaction Rating Scale, Education, Vol. 4 No. 2, 2014, pp. 35-40. doi: 10.5923/j.edu.20140402.04.
Article Outline
1. Introduction
- In early childhood education and care, “inclusive childcare” describes the practice of including children with disabilities in a childcare setting with typically developing children of similar ages, with specialized instruction and support when needed. Children with special needs and typically developing children can both benefit from sharing learning environments and enjoy the rich experiences and relationships that inclusive childcare centers offer growing hearts and minds.Many studies all over the world have demonstrated that inclusion, done well, can be a very positive experience for both young children with special needs and their typically developing peers [1-3]. For example, children with special needs can learn and acquire valuable opportunities to practice various social skills in real-world situations by observing and interacting with other children of similar ages. Meanwhile, typically developing children can benefit immensely from interacting with a child with special needs in their childcare program, as such interaction can help typically developing children develop an increased appreciation and acceptance of individual differences, as well as greater empathy for others.Studies have shown that children who continually interact with children with disabilities developed attitudes of acceptance and understanding not usually present in children who have not had such exposure [4-6]. Enhancing children’s social competence while they are young is both a tremendous responsibility and a privilege with potentially long-lasting effects. In fact, peer interactions provide opportunities for children to learn social skills from each other and understand rules for appropriate behaviors in different settings. Moreover, social relationships established through interactions are a major source of security and belonging [7]. Social competence is defined as the ability to understand others in the context of social interactions and engage in smooth communication with them. Thus, social competence must be evaluated according to the interactions an individual has with his/her social environment [8]. To enable practically effective, context-based evaluations of social competence throughout the lifespan, the Interaction Rating Scale between Children (IRSC) and Interaction Rating Scale Advanced (IRSA) were developed, with which an individual’s levels of “empathy/cooperation,” “self-control,” and “assertion” may be assessed [9]. Several studies assessing social competence have explored these three common aspects in considerable depth [10-12], finding that they were essentially stable from the ages of 1 to 6 in a longitudinal study of Japanese children [13].It is essential to evaluate the social skills relevant to fostering peer relationships among children when identifying the outcomes of inclusive childcare. The purpose of this study was to validate the effects of inclusion in center-based childcare, focusing on the inclusion of children with disabilities, utilizing the IRSC (see Appendix 1) as an evidence-based practical index of social competence.
2. Methods
2.1. Participants
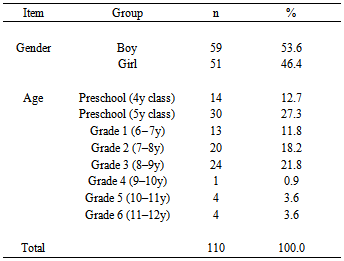
- Participants were children enrolled in an inclusive childcare center for preschool and school age children. Data were obtained from 138 children aged between 3 and 12 years old (59 boys, 51 girls) whose interactions could be measured (Table 1).
|
2.2. Measures
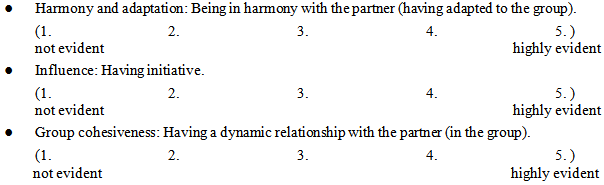
- The IRSC, which can be utilized to evaluate interactions occurring in ecologically valid everyday situations within a short period, was used to assess children’s social competence. The scale was developed as a peer relationship version of the Interaction Rating Scale (IRS) [13-15], which is used to evaluate child-caregiver interactions through observation and is typically used for children under the age of 8. The IRSC is used to measure social competence through a 5-minute observation of children’s interactions with their peers, and includes three subscales measuring cooperation (20 items), self-control (10 items), and assertion (13 items; see Appendix 1). The scoring system for all IRSC subscales was created from laboratory-based observations of the interactions of children. The IRSC items are based on items from the IRS (used for assessing mother–child interactions) [13-15]. We also referred to the IRSA (for adolescents over 15) [16]. In previous studies, social competence from infancy through adolescence has been classified into the three core dimensions: cooperation, self-control, and assertion [10-12]. As such, we based the subscales of the IRSC on these three dimensions. The IRSC has two different levels of scoring each item for each subscale. One is the “behavior score” in which each item reflects a given behavior (e.g., “Expresses his/her opinion well with words”), and evaluators assess whether that behavior is present (1 = “Yes,” 0 = “No”). The sum of all behavior scores in each subscale is the overall behavior score for that subscale. The other is the “impression score” for each subscale, rated on a 5-point scale, where 1 = “not evident at all,” 2 = “not clearly evident,” 3 = “neutral,” 4 = “evident,” and 5 = “highly evident.” The total IRSC score is calculated by summing the “behavior scores” of all three subscales. A higher score indicates a higher level of social competence.The IRSC's internal consistency, as measured by Cronbach’s alpha, was 0.87. The scale’s inter-observer reliability was 90%.
2.3. Procedure
- In the current study, interaction trials to evaluate social competence with the IRSC, each lasting approximately 5 minutes, took place in a child care center, where children’s interactions could be observed and evaluated as they occurred in a natural, realistic setting. We chose a candy distribution task, which has been validated as an interaction-rich context for children in previous inductive research on their social competence. An experimenter asked four participants to distribute fifteen candies among them in an ecologically valid environment. In some groups, a child with special needs, such as autism, Down syndrome, and ADHD participated, while in others, the child did not. The recording was carried out in a room with 2 video cameras. Participants were escorted into this room, which was furnished with a small table, and the instructor asked them to distribute the candies placed on the table.Two evaluators coded the participant’s behaviors during the interaction.
2.4. Analysis
- T-tests were conducted to examine the relationship between peer type (with a child who has disabilities, or with a typically developing child) and social competence. Data analysis was performed with the Statistical Analysis System (Version 9.1).
3. Results
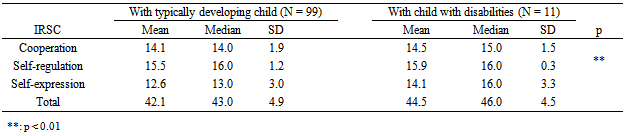
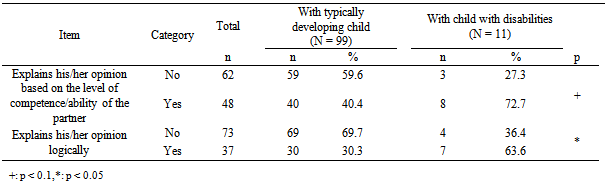
- We examined the relationship between peer type and children’s social competence in the candy distribution task. Table 2 shows the differences in total and subscale scores whereas Table 3 illustrates the differences in item scores in interactions between typically developing children and between a typically developing child and a child with special needs.
|
|
4. Discussion
- Evaluations of social competence using the IRSC in this study revealed that typically developing children showed significantly greater self-control when interacting with children who have disabilities than with typically developing children. Additionally, children tended to explain their opinions logically and in accordance with the level of competence/ability of their interaction partners in interactions with another child with disabilities. These results suggest that inclusive childcare may be effective in enhancing child social competence, especially self-control and flexibility/adaptability, depending on interaction partners’ needs for care. Inclusive childcare may affect children’s perceptions of disability-based exclusion in ways other than through contact or interpersonal experience [1]. The inclusion of children with disabilities requires that children be more flexible/adaptable in their social interactions than in childcare settings consisting entirely of typically developing children. More specifically, mainstreaming children with disabilities promotes high cognitive and social classroom diversity, which is best managed with educational strategies that place less emphasis on general instructions and more on child-centered, cooperative activities [17]. Child-centered care, or care that is sensitive to a child’s specific needs, positively contributes to the classroom norm or expectation that each child, independent of performance, ought to be respected and included [18]. Cooperative activities can further provide children with important interactional opportunities for developing vital social skills as they learn alongside children who have disabilities [19]. Even though previous studies have investigated children’s attitudes toward children with disabilities, these focused primarily on social acceptance [20]. Quite a few researchers have in fact observed that self-control skills acquired in preschool age have lifelong positive effects [21-23].As our findings imply, childcare providers can play a more central role in ensuring the success of inclusive childcare. Inclusive childcare can be beneficial, both for the child with special needs and for other children. Through inclusion, children with special needs gain valuable time and support to build relationships with other children, exposure to a wider variety of challenging activities, and opportunities to learn at their own paces in a supportive environment. Furthermore, typically developing children will be better prepared for adult life in a society that values inclusion, and have opportunities to master activities by practicing and teaching others with different levels of competence/ability.The present findings suggest that mutual interactions with children who have disabilities enhance the adaptive skills of typically developing children. Children learn more from naturally occurring, spontaneous learning situations than from ones that have been fully planned by adults. The same is true when a child with disabilities enrolls in a school and joins a class. Furthermore, children will shape their knowledge, beliefs, and attitudes regarding individuals with disabilities based largely on the attitudes, words, and actions they observe of grown-ups around them. When childcare professionals are purposeful about what attitudes and behaviors they are modeling for children, they can be more confident that they are making a positive impact. It is essential to create an environment, both physical and emotional, where everyone is invited to participate to the extent that they would like and is treated with respect and kindness. Environments like these help children feel comfortable with each other and develop friendships based on their shared interests.Additionally, childcare professionals need to bear in mind that creating a sense of community in the classroom is essential, where every child is valued as a unique individual who has something to contribute and where everyone is responsible for caring for one other. Doing this gives children the freedom to explore their ideas about disabilities through play and conversation, as they are guided to be more aware and respectful of the feelings and perspectives of children with special needs.While this study provides valuable insights, it is also important to acknowledge its limitations. First, our data were drawn from a sample of only 138 participants enrolled in a single childcare center, which might limit the generalizability of our results. Second, ours was a cross-sectional study, on which we plan to expand in the future to include the longitudinal effects of inclusion. Third, the IRSC subscales might not cover all the dimensions of social competence, even though it is structured after the most common framework illustrating social competence. Despite these limitations, our results can be considered valid evidence for the positive effects of inclusive childcare on children’s social competence. These outcomes contribute toward our understanding of the benefits and potential of inclusion in childcare and education.
5. Conclusions
- This study provides evidence that typically developing children’s peer relationships with children who have disabilities can be improved by the experience of inclusive childcare. Further research on inclusion may potentially uncover additional features or factors contributing to the development of children’s social competence. Such information should enhance knowledge of implications for not only research, but also practitioners and caregivers.
ACKNOWLEDGEMENTS
- This research was supported by a Grant-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology (23330174, 24653134) and Nissei financial group.
Appendix 1 Interaction Rating Scale for School Children (IRSC)
- 1. Cooperation: children’s cooperative and empathetic behaviors1) Does not vocalize, make a facial expression, or move in response to the partner’s gestures after the partner’s utterance. 2) Babbles, makes a facial expression, or moves in response to the partner’s behavior or nonverbal cues. 3) Does not vocalize, make a facial expression, or move in response to the partner’s behavior or nonverbal cues. 4) Smiles in response to the partner’s smile. 5) Smiles, claps hands, or shows he/she is glad when the partner is feeling happy. 6) Shares intentions and attitudes with the partner through eye contact. 7) Praises the partner’s efforts, success, and behavior. 8) Smiles and/or nods at the partner during the conversation. 9) Talks to the partner positively or encouragingly during the assignment. 10) Does not vocalize or interrupt the partner while he/she is speaking.11) Accepts the partner’s opinion partially or totally by saying, “let’s do it” or by acting in a manner consistent with the partner’s suggestion. 12) Vocalizes and/or moves in response to the partner’s appearance after the partner’s utterance. 13) Says a word of thanks, such as “thank you” to the partner. 14) Says a word of apology such as “I am sorry” to the partner. 15) Gives a soothing non-verbal response (i.e., pat, touch, or rock). 16) Shows empathy with a verbal or non-verbal response when the partner is in a bad mood. 17) Vocalizes and/or moves in a humorous manner to brighten the atmosphere. 18) Does not criticize the partner. 19) Tries to respond appropriately during confrontation with the partner. 20) Tries to respond calmly when the partner becomes angry or agitated.2. Self-Control: children’s behaviors that emerge in conflict situations 21) Is not rude to the partner and not destructive/rough with the materials. 22) Does not disturb the partner. 23) Concentrates on the task and is gentle with the materials. 24) Does not lose his/her temper. 25) Attempts to elicit help or consolation from the partner. 26) Does not display distress cues even when the task does not go well. 27) Does not tell a lie and does not cheat. 28) Does not speak negatively of others and the materials. 29) Follows the rules of the tasks. 30) Behaves in accordance with the expectations of others. 3. Assertion: children’s initiating behaviors 31) Expresses his/her opinion well with words. 32) Shows his/her feelings well through gestures and behavior. 33) Smiles or laughs. 34) Looks at the partner’s face to get information/clarification. 35) Turns his/her gaze to the partner when trying to get sympathy. 36) Shows his/her feelings well with his/her facial expressions. 37) Speaks up to the partner about what he/she thinks. 38) The partner responds to his/her proposal or decision. 39) Exhibits a differing opinion with his/her expression and gestures. 40) Verbalizes a differing opinion or position. 41) Provides guidance through explanation and not through order. 42) Explains his/her opinion based on the level of competence/ability of the partner. 43) Explains his/her opinion logically.