-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Economics
p-ISSN: 2166-4951 e-ISSN: 2166-496X
2013; 3(6): 243-251
doi:10.5923/j.economics.20130306.01
Health Campaigns and Use of Reproductive Health Care Services by Women in Ghana
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLEmmanuel E. Asmah1, Daniel K. Twerefou2, Jessica E. Smith3
1Department of Economics, University of Cape Coast, Cape Coast, Ghana
2Department of Economics, University of Ghana, P. O. Box LG 57, Accra, Ghana
3Africa Growth Initiative, Brookings Institution, 1775 Massachusetts Avenue, NW, Washington DC, USA
Correspondence to: Emmanuel E. Asmah, Department of Economics, University of Cape Coast, Cape Coast, Ghana.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
The availability of health information and knowledge to women is important in efforts to raise women’s awareness about health practices needed to promote good health outcomes. Policy makers can use different forms of knowledge infrastructure to for example, induce faster diffusion of health information among women. In this study, we have used the Ghana Demographic and Health Survey for 2008 to evaluate differentials in health campaigns (transmitted through television, radio and newspapers) on the use of reproductive health care services by women. This objective is motivated by the fact that Ghana is still off-track in achieving the 2015 maternal health targets, despite the modest gains in other areas. After controlling for other variables in the model, a series of logit regressions showed that health information delivered via television is a significant predictor of the likelihood that a woman would choose skilled delivery care and utilize antenatal care services. Besides health campaign variables, the findings also confirm the importance of wealth, education and location in driving information asymmetry as well as the promotion of good maternal health. These findings imply that family planning campaigns through the mediums of TV and radio need to be intensified and extended to all women, including those in rural areas. Health policy should also encourage investments in education and wealth creation.
Keywords: Reproductive Health Care, Women, Health Campaigns, Logit Regression
Cite this paper: Emmanuel E. Asmah, Daniel K. Twerefou, Jessica E. Smith, Health Campaigns and Use of Reproductive Health Care Services by Women in Ghana, American Journal of Economics, Vol. 3 No. 6, 2013, pp. 243-251. doi: 10.5923/j.economics.20130306.01.
Article Outline
1. Introduction
- Globally, the health of women has engaged the attention of many governments, as has been demonstrated by the mainstreaming of maternal health improvement as the fifth goal in the internationally agreed Millennium Development Goals (MDGs). Despite its fundamental importance to the country’s wellbeing, the statistics on maternal health especially in Africa leave so much to be desired. The 2008 maternal mortality ratio (MMR) of maternal deaths per 100,000 live births was 640 in sub-Saharan Africa, compared with an average of only 14 for developed regions and 290 for developing regions[1]. However, the phenomenon of high maternal death in sub-Saharan Africa is preventable and health solutions are readily available. Ghana, like other developing countries has a high maternal mortality rate. The WHO report estimates a maternal mortality ratio of 350 per 100,000 live births; while in-country reports quote a higher figure of 450. However, as figure 1 show, the maternal mortality ratio since 1990 has been reducing. Despite the modest gains made in achieving other MDGs and an improvement in maternal health, Ghana still lags behind other countries in achieving the 2015 maternal health targets.Given the above statistics and the role women play in the process of human capital formation, it is important for policy makers and health workers to make an effort to promote safe motherhood. Reproductive health services, in particular family planning and maternal health services, can help women avoid unplanned births, unsafe abortions, and pregnancy-related disabilities[2]. One way to make this happen is to provide mothers with information on best maternal health care practices. For example, information and services made available to women through sex education and reproductive health services can help them understand their sexuality and protect them from unwanted pregnancies, sexually transmitted diseases and subsequent risk of infertility[3].
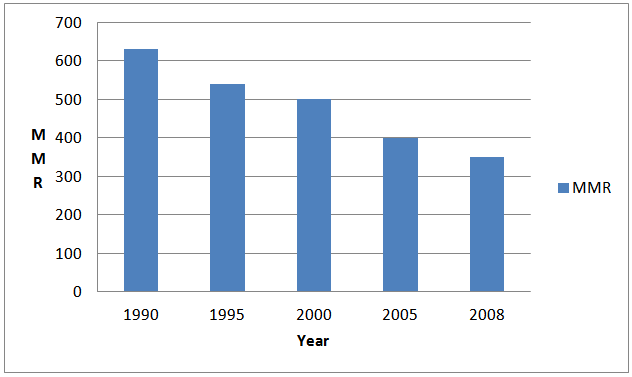 | Figure 1. Trends in marternal mortality ratio in Ghana:1990-2008 |
2. Overview of the Literature
- Reproductive Health, as defined by the World Health Organization (WHO) refers to a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity, in all matters relating to the reproductive system and to its functions and processes. In line with the above definition, reproductive health care is also defined as the constellation of methods, techniques and services that contribute to reproductive health and well-being by preventing and solving reproductive health problems. Reproductive health care includes a variety of prevention, wellness and family planning services as well as diagnosis and treatment of reproductive health concerns[2]. The International Conference on Population and Development (ICPD), held in Cairo in 1994, was noteworthy for achieving a global consensus that all people – regardless of age, parity, marital status, ethnicity, or sexual orientation – are entitled to reproductive health and rights. Reproductive health is a critical component of women’s general health. When women lack access to safe, comprehensive reproductive health care, the consequences can be damaging. Sexual and reproductive ill health accounts for almost twenty per cent of the global burden of disease for women and fourteen per cent for men[12]. Positive reproductive health means that individuals can manage their own sexuality and have unrestricted access to the full range of reproductive health care options. The choice of reproductive health care services by women, as with other areas of health care options, is influenced by a complex interplay of economic and social determinants ([2],[13],[14] and[15]). The United Nations sixty-seventh session of the General Assembly resolutions on Global Health and Foreign Policy acknowledges “that many of the underlying determinants of health and risk factors of both non-communicable and communicable diseases, in particular tuberculosis, malaria and HIV and AIDS, as well as the causes of maternal and infant mortality, are associated with social and economic conditions, the improvement of which is a social and economic policy issue”[16].An extension of the social determinants to cover media exposure is gradually becoming an important consideration. Exposure to television, radio, newspapers or magazines are important sources from which women obtain information that can help them understand their sexuality and protect them from unwanted pregnancies, sexually transmitted diseases and subsequent risk of infertility[2]. Quite a number of empirical studies exist on the effects of media exposure on different reproductive health indicators. For example, in Nigeria, use of modern contraception, intent to use, and desire for fewer children were found to be associated with exposure to media messages on family planning[17]. A similar study in Tanzania found that women exposed to a mix of media promoting family planning were more likely to use family planning[18]. According to a study in Nepal, exposure to mass media had an indirect effect on contraceptive use through increases in interpersonal communication, as well as positive changes in attitudes and perceived social norms regarding family planning[19]. In Mali, exposure to a campaign was linked to more favorable attitudes towards family planning and a decline in the proportion of men and women who believed that Islam opposes family planning[20]. Gupta et al[21] examined the influences of multi-media Behavior change communication campaigns (BCC) on women's and men's use of and intentions to use contraception in target areas of Uganda. Results indicated that exposure to BCC messages was associated with higher contraceptive intentions and use. A few related studies based on Ghana include the work by[22],[23],[24],[25],[26],[27] and[28]. A comprehensive review of the literature by Women’s Health West[2] cites many other country instances where mass media campaigns have proved successful in promoting family planning. Another WHO study found that whiles factors such as media exposure, migration, connectedness to school and family among others were identified as important in industrialized countries; research on these factors in developing countries is too scanty[29]. The study found that many of the research focused on individual socio-demographic factors, such as age, sex, socioeconomic status, and geographic location, many of which are not amenable to programmatic interventions. An earlier synthesis of the research evidence on reproductive health in Ghana aimed at identifying research gaps by Awusabo-Asare et al[3] found that much of the existing studies on Ghana shows the levels and patterns in risky sexual and health behaviors, but provide very little evidence to explain why. The current research is similar in spirit and conception to most of the above cited studies, especially the one by Kwankye and Augustt[26]. Instead of the focus on sexual and reproductive risk factors, this present study investigates the extent to which media exposure affects the use of contraceptives, antenatal care and skilled delivery based on new data for Ghana.
3. Theoretical Framework
- To provide a theoretical frame of reference for analyzing the relationship between the use of reproductive health care services by women and health campaigns, this study draws from Gary Becker’s[30] household production theory, which was also extended by Grossman[31]. The analysis is also similar in spirit and conception to the studies by[32] and Mwabu[33]. In these models, health, defined as a state of physical, mental and social well-being of the individual is viewed as a consumer good as well as a durable capital good. As a consumer good, individuals derive satisfaction and have a high preference for a good health status. Given an initial stock of health capital that tends to deteriorate overtime, individuals invest in their health status in order to earn some economic return (normally in the form of healthy time for the capability to function). A mother’s health is a scarce commodity relative to the capabilities it can yield in terms of functioning. Thus, individual women within their households need to allocate resources in an optimal way to derive the maximum benefits from the consumption and production of health. The standard neoclassical approach to utility maximization serves as a good framework for understanding individual behavior in this context. Following[33], the approach considers a woman whose utility (U) is assumed to depend on a health-neutral (X), a health-related good or behavior (Y) and home produced maternal health, H. It is also assumed that the maternal health production function is given by:
 | (1) |
 captures the component of the mother’s health due to genetic endowments, environmental factors and other components not influenced by preferences. Thus, the objective function becomes:
captures the component of the mother’s health due to genetic endowments, environmental factors and other components not influenced by preferences. Thus, the objective function becomes: | (2) |
 | (3) |
 the number of hours worked and
the number of hours worked and  are prices of health neutral good, health related consumer goods and maternal health services.The time constraint is also given as:
are prices of health neutral good, health related consumer goods and maternal health services.The time constraint is also given as:  | (4) |
 is leisure. Substituting (4) into (3) yields;
is leisure. Substituting (4) into (3) yields; | (5) |
 | (6) |
 | (7) |
 | (8) |
 | (9) |
4. Estimation Methods and Empirical Strategy
- In order to assess the influence of health campaigns on the use of reproductive health care services by women in Ghana, we follow a general specification of the form:
 | (10) |
 the dependent is a variable representing selected reproductive health care services,
the dependent is a variable representing selected reproductive health care services,  is a vector of individual characteristics of the woman (age, education, religion, ethnicity, etc.) that also includes variables on access to health campaigns.
is a vector of individual characteristics of the woman (age, education, religion, ethnicity, etc.) that also includes variables on access to health campaigns.  is a vector of parameters to be estimated and
is a vector of parameters to be estimated and  is the disturbance term which includes all the unobserved factors that affect the woman’s use of reproductive health care services. The dependent variable in equation (10) is defined as a discrete dichotomous variable. In that regard, the appropriate empirical technique for empirical estimation is a linear probability model, i.e. logit, probit, nested logit, or some variation. The particular choice of probability model between logit or probit depends largely on preference as there are no compelling statistical reasons for using one or the other[34]. The major differences between the two models are the distributional assumptions of the disturbance term,
is the disturbance term which includes all the unobserved factors that affect the woman’s use of reproductive health care services. The dependent variable in equation (10) is defined as a discrete dichotomous variable. In that regard, the appropriate empirical technique for empirical estimation is a linear probability model, i.e. logit, probit, nested logit, or some variation. The particular choice of probability model between logit or probit depends largely on preference as there are no compelling statistical reasons for using one or the other[34]. The major differences between the two models are the distributional assumptions of the disturbance term,  In the logit model the distribution of the error term is assumed to be logistically distributed; while the in the probit model a normal distribution N (0, 1) is assumed. For ease of interpretation of the sign and significance of the coefficients, this study adopts the logit model[35]. The general logit model takes the following form:
In the logit model the distribution of the error term is assumed to be logistically distributed; while the in the probit model a normal distribution N (0, 1) is assumed. For ease of interpretation of the sign and significance of the coefficients, this study adopts the logit model[35]. The general logit model takes the following form: | (11) |
5. Discussion and Results
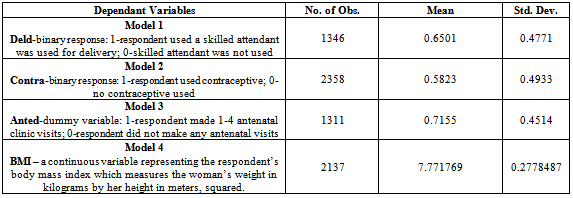
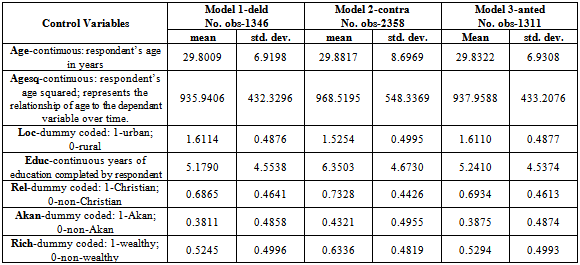
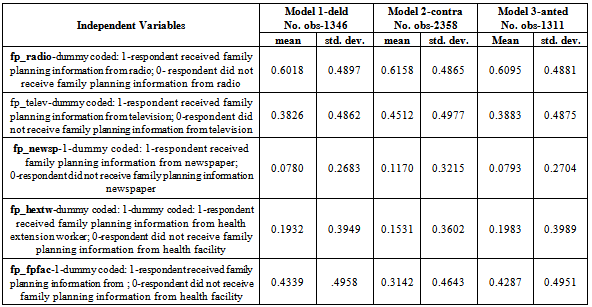
- The Data used in the study were drawn from the 2008 nationally representative Ghana Demographic and Health Survey (GDHS). Table 1 describes the dependant variables and their dichotomous responses. The number observations used in the three logit models vary from 1,311-2,358. Variation in observations is due to the fact that if a survey response is not recorded, the entire observation is dropped from the model in STATA. Table 2 presents the summary statistics of the control variables for each of the logit models. The mean education levels are 5.24, 6.35, and 5.18, respectively, and education levels range from 1 to 19 years of schooling. Ages of the survey respondents vary from 15-49, and the mean age is approximately 29.8 years for each of the three models. Table 3 provides the mean and standard deviation for the independent variables that represent a survey respondent’s access to health campaigns. As reported, each of these variables is a dummy for having received family planning information from various media or health resources. These variables along with the controls were entered into the three logit models to estimate whether they have any impact on a woman’s reproductive health decisions. Thus, there are three panels representing each of the logit models. Model 1 represents the skilled delivery, model 2 contraceptive use, and model 3 antenatal visit responses.
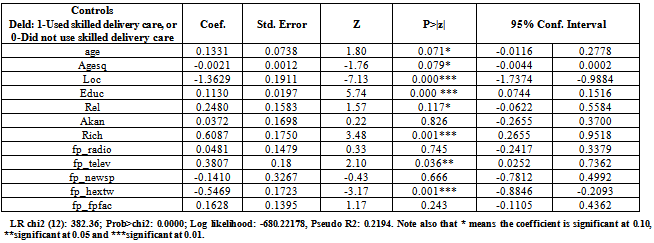
5.1. Model 1 – Health Campaigns and Skilled Delivery Care
- The first logit model, as shown in table 4, determines the likelihood that the average survey respondent will use a skilled delivery, in the event of pregnancy, deld. The predictor variables are a vector of control variables and a series of dummies relating whether the respondent has received family planning knowledge from the following sources: radio, television, health extension and/or a health facility. The dummy is always 1 - has received family planning information (for each information channel) or 0 - has not received family planning information. In the first model there are 1,346 observations and the likelihood ratio chi square 382.46 (12 degrees of freedom) with a small p value can be interpreted as the logit model has a good fit as compared to a model without predictors. For all models age squared is negative and significant. The variable age squared is included in the model to show that the relationship between age and the dependant value deteriorates over time, i.e. as women age they no longer make these maternal health decisions. An increase in a respondent’s age, education level, and level of wealth are all significant predictors that she will use a skilled delivery. If the respondent belongs to a Christian religion then she is more likely to use a skilled delivery than respondents belonging to non-Christian religions, as designated by the positive significant coefficient for religion. Respondents from rural areas are less likely to use a skilled delivery as the variable loc is negative and significant. Ethnicity, akan, of the survey respondent is not a significant predictor of whether or not she will use a skilled delivery. Looking at the health campaign variables as predictors, receiving health messages through television and health extension significantly predicts deld. Thus, viewing family planning information on television increases the probability that a respondent will use a skilled delivery. Unexpectedly, if a respondent has received family planning information from a health extension agent she is less likely to use a skilled delivery. Perhaps this is because respondents who are served by health extension agents are in more remote locations with less access to skilled delivery services. The remaining health information channels were not statistically significant.
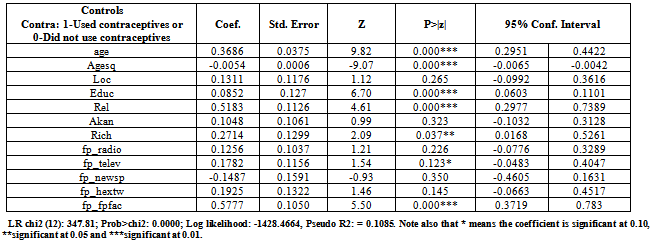
5.2. Model 2 – Health Campaigns and Contraceptive Use by Women
- The second logit model estimates the likelihood that a survey respondent will use contraceptives, contra, using 2,358 observations. Table 5 shows that the predictor variables remain the same as the previous logit model for skilled delivery, and that the model also has a small p value. In model 2, the age, education, wealth, and Christian religion are significant predictors that a respondent will use contraceptives. That is the older, more educated, wealthier, and if a woman is Christian, the more likely she is to use some form of contraceptive. According to the Ghana Maternal Health survey, location and ethnicity of the respondent are not significant predictors of her decision to use birth control. The health campaign variable, fp_fpfac, was positive and significant, thus women who receive family planning information from a health facility are more likely to use contraceptives in this sample. Additionally, family planning information viewed on television, fp_telev, is slightly significant at the 0.10 level. The other health information channels were not significant for contraceptive use.
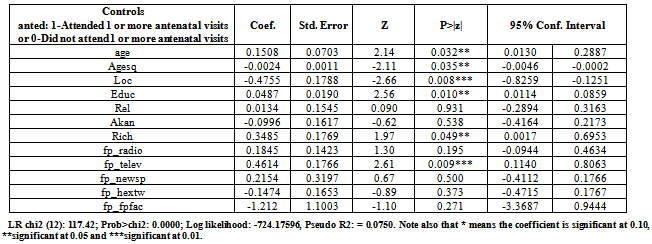
5.3. Model 3 - Health Campaigns and Antenatal Care Visits by Women
- The third logit model in the logit series, represented in table 6, estimates the likelihood that a survey respondent will have one or more antenatal visits, anted. This model used 1,311 observations, and the same predictor variables as the contra and deld logit models with a small p value. When estimating the likelihood that a survey respondent will have one or more antenatal visits, model 3 finds that age, education, and wealth are significant and positive. This suggests that wealthier, older, and more educated women are more likely to attend antenatal visits. As expected, location is negative and significant showing that women in rural areas are less likely to go to antenatal care; probably due to access issues. Religion and ethnicity are not significant predictors of a woman’s tendency toward antenatal visits. The variable fp_telev, the proxy for family planning information received via television is positive and significant. Thus, women who receive family planning information via television are more likely to attend one or more antenatal visits.
6. Conclusions
- The availability of health information and knowledge to women is important when considering efforts to raise awareness of health practices and positively influence maternal health behaviors. In this study, we have used the Ghana Demographic and Health Survey for 2008 to investigate whether access to family planning messages transmitted through different forms of knowledge infrastructure affect maternal reproductive health decisions. After controlling for some individual characteristics in the model, the logit regressions revealed that, women who received health messages conveyed through television have a higher likelihood to use skilled delivery care and utilize antenatal services. Besides showing the significance of information access, the logit model confirms most of previous theoretical and empirical expectations about the positive influence of education, wealth and health endowments on maternal reproductive health decisions. In addition, households who live in urban communities were predicted to have a higher probability of exposure to health campaigns and utilize reproductive health services. Various post estimation tests for the models were conducted. Most of the tests passed as required except for the heteroskedasticity test which was corrected by reporting the robust estimates. The results from the control variables imply that health policy should encourage investments in education and wealth creation. In addition, health campaigns need to be intensified and extended to all women, including those in rural areas, through the medium of TV and radio.
Appendix – Summary Statistics and Table of Results
|
|
|
|
|
|
Notes
- 1.The MMR is simply the total number of maternal deaths occurring for a given number of births (typically 100,000).2. See[3][5];[6];[7];[8],[9];[10].