-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Diabetes Research
p-ISSN: 2163-1638 e-ISSN: 2163-1646
2020; 9(1): 5-11
doi:10.5923/j.diabetes.20200901.02

Evaluation of the Level of Knowledge and Practice of Hygieno-Dietary Measures in Diabetic Patients at the Medical-Surgical Clinic of the Sylvanus Olympio University Hospital in Lomé (Togo)
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbdou Razak Moukaila 1, 2, Edem Komi Mossi 1, 2, Komi Dzidzonu Nemi 1, Kossi Kodjo 1, Agbeko Kodjo Djagadou 1, Abago Balaka 1, Massan Agbanda 3, Emile Kou'santa Sabiba Amouzou 4, Awalou Mohaman Djibril 1
1Department of Internal Medicine, University of Lome, Lome, Togo
2Members of Diabetes Academic Afrique (D2A)
3Department of Pharmacy, University of Lome, Lome, Togo
4Department of Sciences and technologies, University of Kara, Kara, Togo
Correspondence to: Abdou Razak Moukaila , Department of Internal Medicine, University of Lome, Lome, Togo.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Diabetes care also requires therapeutic education to ensure that patients understand the hygieno-dietary measures necessary to achieve and maintain glycemic control. The objective of our study was to evaluate the level of knowledge and practice of hygieno-dietary measures (HDMs) in diabetic patients in Togo but also to evaluate their role in achieving glycemic control. This is a descriptive and cross-sectional prospective study that took place over a period of six months (August 1, 2018 - January 31, 2019) at the Medical-Surgical Clinic of the Sylvanus Olympio University Hospital. Included in our study were patients with diabetes all gender included, at least 18 years of age, diagnosed and followed for at least one year, with a glycated hemoglobin (HbA1C) measurement no more than three months old and who agreed to participate in the study. A total of 138 patients were registered. Females accounted for 51.4% with a M / F sex ratio of 0.9. The median glycated hemoglobin level was 7.90% (IQR: 6.90-8.20). Twelve point thirty percent of the patients had a notion about HbA1C. Our study allowed us to estimate that 72.5% of patients had an average level of knowledge about diabetes and its HDMs. Twenty-four point six percent of diabetic patients said they regularly use HDMs. The level of knowledge about diabetes and HDMs was not associated with adherence to HDMs. Snacking (p = 0.035) and patients' opinions about their glycemic control (p = 0.013) were the factors associated with glycemic control.
Keywords: Diabetes, Knowledge, Hygieno-dietary measures, Diet, Togo
Cite this paper: Abdou Razak Moukaila , Edem Komi Mossi , Komi Dzidzonu Nemi , Kossi Kodjo , Agbeko Kodjo Djagadou , Abago Balaka , Massan Agbanda , Emile Kou'santa Sabiba Amouzou , Awalou Mohaman Djibril , Evaluation of the Level of Knowledge and Practice of Hygieno-Dietary Measures in Diabetic Patients at the Medical-Surgical Clinic of the Sylvanus Olympio University Hospital in Lomé (Togo), International Journal of Diabetes Research, Vol. 9 No. 1, 2020, pp. 5-11. doi: 10.5923/j.diabetes.20200901.02.
Article Outline
1. Introduction
- In 2019, the International Diabetes Federation estimates that 463 million adults between the ages of 20 and 79 years have diabetes [1]. During the same period, diabetes and its complications are estimated to have caused 4.2 million deaths among adults aged 20 to 79 years [1]. With an estimated prevalence of 3.9% in 2019, Africa carries a heavy burden of diabetes with about 73.1% of diabetes-related deaths [1]. In Togo, diabetes is on the rise as a result of the population’s changing lifestyle and the associated nutritional transition [2]. The prevalence of diabetes in Togo is estimated at 2.6% according to the STEPS 2010 survey [2].Diabetes is the subject of numerous studies around the world in its diagnostic, therapeutic, but also preventive and educational aspects. Diabetes care beyond drug treatment must be based on a therapeutic education with the aim of making patients assimilate hygieno-dietary measures (HDMs) and therapeutic compliance with ultimately good glycemic control. When these rules are followed properly, they may improve the life expectancy of the diabetic patient [3]. Unfortunately, the socio-cultural and economic conditions specific to each region have a great deal of influence on the knowledge and compliance of these HDMs, which involve the choice of food, physical exercise and weight management.In order to understand the parameters influencing the perception and the implementation of HDMs by people living with diabetes in Togo, we set ourselves the objective of evaluating the level of knowledge of hygieno-dietary rules and identifying the factors associated with compliance with hygieno-dietetic measures.
2. Patients and Methods
2.1. Framework
- This was a prospective, descriptive and cross-sectional study which took place from August 1, 2018 to January 31, 2019 (06 months) at the Medical - Surgical Clinic (MSC) of the Sylvanus Olympio University Hospital, national reference center of the health system in Togo.
2.2. Study Population
- Diabetic patients were included in our study regardless of gender and type of diabetes:- diagnosed and followed for at least one (01) year, assuming that after one year of follow-up a person living with diabetes has had enough time to benefit from therapeutic education- at least 18 years of age- received in a medical consultation as part of a follow-up appointment or hospitalized in the department for a complication related to his or her diabetes and with a clear conscience at the time of the survey;- with a glycated hemoglobin level no older than three months.We excluded from our study any patient who did not meet the inclusion criteria and who expressed a refusal to participate in the study.
2.3. Sampling
- To calculate the minimum sample with good representativeness, we used Giezendanner’s expression [4]:
 n = sample sizez = confidence level according to the reduced centered normal law (for a confidence level of 95%, z = 1.96)p = estimated proportion of the population with the characteristic (prevalence of diabetes)d = tolerated margin of error (5%)Based on the prevalence of diabetes in Togo which is estimated at 2.6%, a minimum of 39 patients is representative. However, we targeted a minimum of one hundred patients for our study and had identified a total of 138 patients.
n = sample sizez = confidence level according to the reduced centered normal law (for a confidence level of 95%, z = 1.96)p = estimated proportion of the population with the characteristic (prevalence of diabetes)d = tolerated margin of error (5%)Based on the prevalence of diabetes in Togo which is estimated at 2.6%, a minimum of 39 patients is representative. However, we targeted a minimum of one hundred patients for our study and had identified a total of 138 patients.2.4. Study Variables
2.4.1. Socio-Demographic Characteristics and Diabetes History of Respondents.
- These variables included sex, age group, weight, height, Body Mass Index (BMI), level of education, socio-professional class, length of time with diabetes, how diabetes was of discovered.
2.4.2. Knowledge about Diabetes
- Patients were asked about the definition of diabetes, their type of diabetes, current treatment, their views on the concept of glycemic control and the severity of diabetes as a disease. The existence of complications due to diabetes, the modalities of diabetes care, the concept of glycated hemoglobin (HbA1c) and its usefulness, their recent HbA1c levels were also informed.
2.4.3. Evaluation of the Level of Knowledge of Hdms
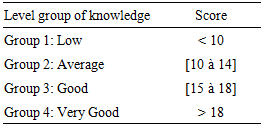
- To evaluate patients’ level of knowledge, we used a 20-point scale scoring system based on similar studies [5,6]. Based on each respondent’s answer to a question, we awarded 1 point for a correct answer or 0 point for a wrong answer.The questions that were scored were:1. the definition of diabetes2. the definition of glycated hemoglobin (HbA1c)3. the usefulness of weight loss4. the usefulness of physical exercises,5. the complementarity of the measures implemented for diabetes care6. Togolese context specific food classification tests. The patient had to be able to identify the food as being to be avoided, consumed in moderation or free of consumptionThe lowest score that could be obtained from the evaluation was 0 points, and the highest score that could be obtained was 20 points.Once the scores were obtained, patients were classified into four groups according to their score (Table 1).
|
2.4.4. Evaluation of HDMs Compliance
- Patients were evaluated on their compliance with daily dietary and hygienic recommendations: frequency of HDMs application, habitual snacking, physical activity (frequency and duration) and finally the identification of factors that limit HDMs application.
2.5. Data Collection
- Data collection was carried out using standardized anonymous questionnaires developed from similar studies [5,6] that we have readapted by taking into account the different food recipes in Togo. The said questionnaire was pre-tested on a small sample of patients in order to readjust the items if necessary before the actual investigation.
2.6. Data Entry and Analysis
- All data was entered into a data entry mask developed in Epidata version 3.1 software and then analyzed using IBM SPSS Statistics version 20 statistical software.Descriptive analysis included means and standard deviations for quantitative data with a normal distribution, medians and interquartile ranges for quantitative variables that did not conform to a normal distribution. The percentages were used to describe the qualitative variables.The percentages were compared using the chi-square test or Fisher's exact test when the theoretical numbers were less than n = 5.The test results were considered statistically significant at the 5% threshold.
2.7. Ethical Consideration
- We obtained the favorable opinion of the Director of the MSC to conduct our study. Each patient who participated in the survey gave informed consent. Anonymity was respected as well as the confidentiality of their answers.
3. Results
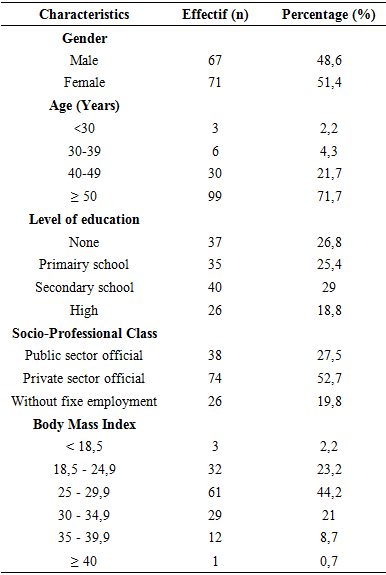
- During our study, we identified a total of 138 patients who met the inclusion criteria.The female sex was predominant with a frequency of 51.4%. The M / F sex ratio was 0.9. Patients over 50 years of age were most represented in 71.7% of cases.Nearly three-quarters (74.60%) of the patients had a Body Mass Index (BMI) greater than 25Kg / m2. Of these patients, patients classified as overweight accounted for 44.2%. The rest of characteristics of the respondents are presented in Table 2.
|
3.1. Knowledge about Diabetes
- While 71.70% of patients said they had a notion about diabetes, barely half (44.90%) of patients were able to give a satisfactory definition of diabetes.More than three-quarters (84.1%) of patients felt they had type 2 diabetes. Nine point four percent (9.4%) considered themselves to have type 1 diabetes. The distribution of patients' opinions on the type of diabetes they were suffering from with their current treatment showed that 53.85% of the patients who claimed to have type 1 diabetes were taking oral antidiabetic treatment.About half (47.8%) of our patients reported that their diabetes was poorly controlled. Twelve point thirty percent of patients were able to satisfactorily explain the role of glycated hemoglobin in the follow-up of their condition. The median glycated hemoglobin level was 7.90% (IQR: 6.90 - 8.20). The distribution of patients according to their glycated hemoglobin showed that 26.8% of the patients in our series had an HbA1c level less than 7%.The majority of patients, 87% believed that diabetes was a serious disease.Regarding the means useful for the care of diabetes, 81.20% of patients declared that diabetes care should take into account a complementarity between drugs, physical exercise and dietary measures (Figure 1).
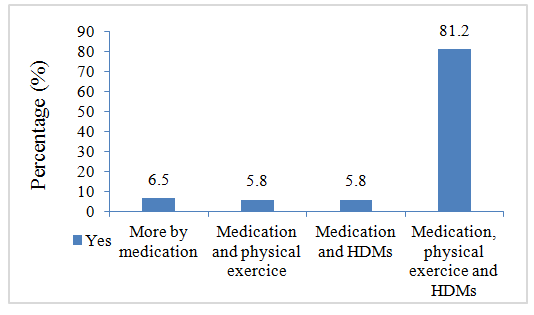 | Figure 1. Patients' opinions on useful diabetes management solutions |
3.2. Evaluation of the Level Of Knowledge and Adherence of Hygieno-Dietary Measures
- More than three - quarters of the patients (79%) said they were aware of the main components of hygieno-dietary measures, namely an education on diet, physical exercise and weight management.Diabetic physicians and internists were the most cited as a source of information on HDMs for patients in 56.5% followed by the general practitioner cited by 47.2% of patients.About three - quarters (73.2%) of patients found it useful to receive information about HDMs.The majority of patients had good abilities to categorize foods as avoidance, moderation or free choice.The median score for evaluating knowledge on a 20-point scale was 14 (IQR: 13 - 16).Seventy-two point five percent of the patients evaluated had an average level of knowledge about diabetes and hygieno-dietary measures (Figure 2).
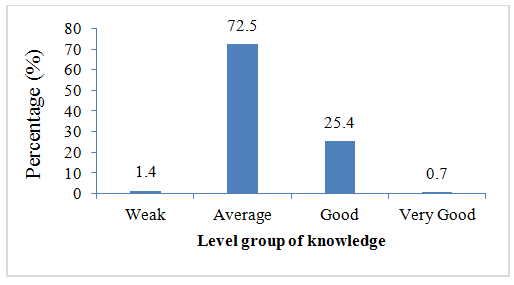 | Figure 2. Distribution of patients according to their level of knowledge on diabetes and HDMs |
|
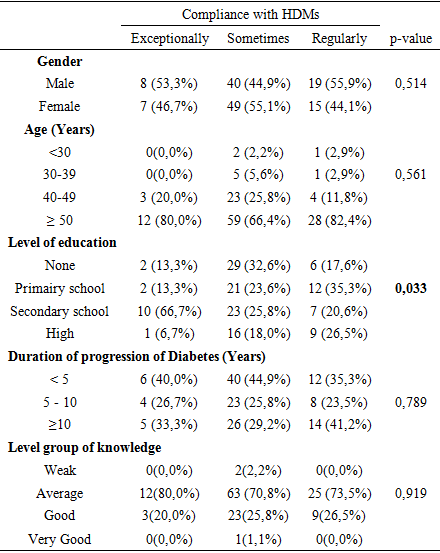
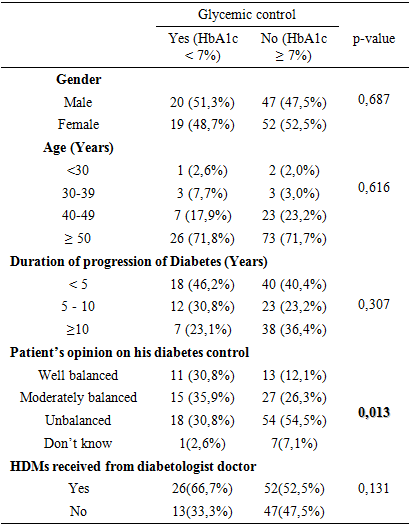
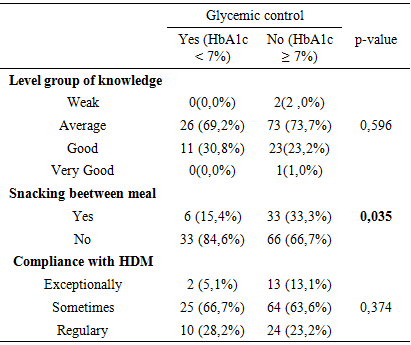
3.3. Factors Associated with Glycemic Control
- Glycemic control was associated with snacking between meals (p = 0.035), and patients' opinions about their diabetic control (p = 0.013) (Table 4).
|
|
4. Discussion
- The originality of our study lies, on the one hand, in the evaluation of the knowledge of diabetic patients in relation to their disease, their level of adherence with hygiene -dietary measures and, on the other hand, in the identification of the difficulties they face in the management of their disease. As with any cross-sectional study, selection bias cannot be ruled out, especially given the mode, site of recruitment and the inclusion criteria. We were unable to address certain variables such as comorbidities associated with diabetes (hypertension, dyslipidemia), and adherence to therapy. We have shown that just over half of the diabetic patients recruited (50.70%) were still professionally active. This result contrasts with what has been observed in France [5,12] where most of the subjects were pensioners. This difference could be explained by the age pyramid, which in Western countries corresponds to a widened top reflecting a low birth rate and an aging population, whereas in Africa the age pyramid corresponds to a wider base predominated by young and therefore active subjects. The duration of diabetes progression was less than 5 years in 42% of the cases in our study. This percentage is close to those reported in Mali by Coulibaly et al. [6] and Keita et al. [9], who reported 40 and 42.85%, respectively. On the other hand, in industrialized countries, the duration of evolution was more than 10 years, as reported by Donnio-Cordola et al. [13] and Royal et al. [5]. In Africa, the lack of financial resources limits spontaneous consultations and the completion of health check-ups for early detection of diabetes. The diagnosis is usually made late, which explains why patients are followed for a short time in the majority of cases. On the other hand, in developed countries, the existence of mutual health insurance encourages screening and the early start of diabetes monitoring.Approximately 45% of the patients surveyed were able to provide a satisfactory definition of diabetes. This observation corroborates the low literacy rate achieved in our study population. Indeed, our study showed a statistically significant association between the level of education and the ability to define diabetes (p = 0.047). However, more than 50% of our study population had not progressed beyond the primary level.Eighty-four point ten percent of patients estimated they had type 2 diabetes. Seven of the thirteen patients who reported having type 1 diabetes were on oral antidiabetic treatment. These patients may not have a clue about the difference between type 1 and type 2 diabetes. This lack of knowledge regarding the type of diabetes on the part of patients has been reported in the literature [14].The majority of patients (87%) stated that diabetes is a serious disease, which reflects the common thinking of diabetic subjects about the risks of uncontrolled diabetes. Unfortunately, our study revealed a high rate of non-adherence as only 1/3 of the patients in our study (26.8%) could be considered to have glycemic control. More than 80% of patients had no idea about glycated hemoglobin and its importance in the care and monitoring of diabetes. This result confirms the results of a study that reported that only 30% of patients were able to give an accurate definition of HbA1c [15].The French study DIABASIS also reported that « the most reliable measure of diabetes control (glycated hemoglobin) remains unknown to 79% of respondents [16].About three-quarters of the patients (73.2%) in our series had glycated hemoglobin greater than or equal to 7%. This result corroborates the low rate of compliance with hygieno - dietary measures, but also certainly with medication. Coulibaly et al. [6], obtained in their series a proportion of 67% of patients who also had glycated hemoglobin greater than or equal to 7%. In terms of nutritional education, we found in our study that 79% of the patients included in our study admitted having received information about diet, the importance of physical effort and weight loss. This result is in line with the results of a Tunisian study carried out in Sousse [17] which reports that about 90% of the patients had knowledge about physical activity and dietary measures, including changes in eating behavior and the need for balanced meals under oral antidiabetic treatment.Almost 3/4 of the patients in our sample (72.5%) had a level of knowledge about diabetes and HDMs that we estimated to be average. Our result is consistent with two studies that reported a low level of knowledge of diabetic patients on dietetics. It’s about a Norman [18] and Nigerian study that used the Michigan Diabetes Knowledge Test (MDKT) to assess the knowledge of the Nigerian diabetic population [15]. In contrast, patients in the study by Royal et al., [5] had a good level of knowledge and application of HDMs. An exercise thesis carried out in Rouen with a small sample had also found satisfactory results with regard to food control [16]. The varying levels of patient knowledge in our context could be explained by the insufficient means implemented in the therapeutic education of diabetic patients, which vary from one country to another and according to the organization and priorities of the health system. In developed countries, degenerative diseases are the priority with regards to public health problems, while in developing countries, infectious diseases have priority, especially in tropical areas. It should also be noted that it has been shown that patients who have consulted a dietician have a better knowledge of the disease than people who never consulted [17].Certain variables in our study such as sex, age group, level of education, age of diagnosis of the disease, mode of discovery and source of information received were not statistically associated with the level of knowledge of the patients surveyed. Royal et Al. have achieved the same result in their series [5].Patients in our study had a low level of adherence with hygieno - dietary measures. Only 24.6% stated that they regularly apply advices related to HDMs. This low adherence rate is similar to the data in the literature [12] and justifies the glycated hemoglobin level greater than or equal to seven observed in the majority of patients in our series. Indeed, a study carried out by the team of Jenkins et al. [17] in Canada on the diet favoring foods with a low glycemic index (nuts, green beans, lentils, pasta), showed that the group of patients who followed this dietary guidelines saw their HbA1c level reduced by one half point, compared to only 1/20th of a point for the other group. According to the same authors, HbA1c is a parameter that reflects the average level of glucose in the blood, minute by minute, over a period of two or three months and is an indispensable tool for evaluating diabetes control.The majority of patients had access to three meals a day identical to those of other family members. Thus, they found it difficult to make significant changes in the choice of menu that would not alter their diabetic balance. This results in the low adherence rate with the hygiene - dietary measures obtained. Fortunately, more than 50% of patients said they did not snack between the three main meals. Our study showed that patients who did not snack between meals had significantly good glycemic control (p = 0.035). This attitude should be promoted in diabetic patients during their education (Table 4).Besides diabetic balance measures, another important hygienic-dietary measure is physical exercise. Sixty point nine percent of patients reported being physically active. Our result falls within the range of results reported by Coulibaly et al. [6], with 57% and by the study by Silvera et al., in Ile de France which reported 66.8% [18].Being served a different menu other than the family meal because of diabetes remains the main obstacle mentioned by patients (49.30%), contrary to the study by Royal et al., [5] and the Norman survey [18] where the main obstacles to compliance with hygienic-dietary measures were fatigue and eating outdoors. In Africa, the meal time is a time of communion and sharing. Having a different menu from that of the rest of the family may be experienced by the patient as an exclusion from the family nucleus.
5. Conclusions
- The best weapon against diabetes is patients’ therapeutic education, which requires knowledge of the disease and how to manage it. We found during our investigation that the majority of patients received information about the non-drug management of their pathology and are quite familiar with it. But adherence to these measures remains a major problem for patients. This low adherence resulted in a high proportion of patients with uncontrolled diabetes. Given the low rate of compliance with HDMs, further studies are needed in order to propose suitable strategies to improve glycemic control of patients living with diabetes in Togo and thus prevent complications.