-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Diabetes Research
p-ISSN: 2163-1638 e-ISSN: 2163-1646
2017; 6(3): 68-72
doi:10.5923/j.diabetes.20170603.04

Conceptual Model of Diabetes Self-Management for Middle-Aged Population of Rural Area of Pakistan
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRashid M. Ansari, Hassan Hosseinzadeh, Mark Harris, Nicholas Zwar
School of Public Health and Community Medicine, UNSW, Sydney, Australia
Correspondence to: Rashid M. Ansari, School of Public Health and Community Medicine, UNSW, Sydney, Australia.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: The high prevalence of type 2 diabetes in Pakistan has been attributed to high-risk factors such as lack of physical activity, unhealthy food and eating habits among the Pakistani population. Aims: The main aim of this study is to explore the factors that may influence diabetes self-management in the middle-aged population of rural area of Pakistan and to present the potential outcomes. Materials and Methods: The study was guided by the results of systematic reviews of self-management of type 2 diabetes and highlighted five factors which are most important to influence the diabetes self-management. Of particular mention are the factors such as socio-demographic characteristics, behavioural and psychological characteristics, social support, self-management barriers and cultural characteristics in that population. Results: The potential outcomes derived from improved diabetes self-management in the middle-aged population include quality of life, reduction in HbA1c values and overall improvements in blood pressure and other cardiovascular risk factors. Conclusion: This study will help to improve the diabetes self-management approach in middle-aged population in rural area of Pakistan. The conceptual modeldeveloped in this study will provide a platform for future research and will help to better understand the contextual determinants of behaviours for future development of culturally appropriate interventions to support self-management activities.
Keywords: Type 2 diabetes, Conceptual model, Middle-aged population, Self-management
Cite this paper: Rashid M. Ansari, Hassan Hosseinzadeh, Mark Harris, Nicholas Zwar, Conceptual Model of Diabetes Self-Management for Middle-Aged Population of Rural Area of Pakistan, International Journal of Diabetes Research, Vol. 6 No. 3, 2017, pp. 68-72. doi: 10.5923/j.diabetes.20170603.04.
Article Outline
1. Introduction
- Diabetes mellitus is a pandemic disease and one of the leading threats to human health [1]. The 2014 estimates by the International Diabetes Federation (IDF) showed that there are a total of 371 million people suffering from diabetes in the world [2]. The estimates also showed that the disease accounted for approximately 4.8 million deaths. Type 2 diabetes is more prevalent among people aged between 40 and 59 years. The prevalence of type 2 diabetes is higher in Pakistan due to the sedentary lifestyle, obesity and other risk factors in the country [2]. The prevalence of lifestyle risk factors is 26.5% among the males aged 50–59 years and 35% among females with the same age group [3]. Economically, Whiting et al. [3] reported that more than 471 billion US dollars have been spent on diabetes healthcare globally. Pakistan is one of the developing countries where the health and economic impacts of diabetes have been felt. Whiting et al. [3] estimated that the prevalence rate of the disease in Pakistan is 7.6 -11% [3]. In the local context, it has been estimated that in 2030, the prevalence rate in Pakistan will increase to 15% (13.8 million populations) [4]. Therefore, Pakistan is ranked 7th on diabetes prevalence list [5]. Additionally, Pakistan is among the top 10 countries in the world for people with diabetes aged 20-79 years [3]. Type 2 diabetes mellitus is, therefore, a major public health concerns affecting the middle-aged population. This is because the middle-aged population in the country is overweight and obese. In addition, the population does not participate in an active physical activity and have unhealthy eating habits. This exposes the population to a high risk of type 2 diabetes [5, 6]. It was reported by Jafar et al. [5] that in a large population-based sample prevalence of overweight was 25% and obesity was 10% [5, 6]. The current literature revealed that diabetes self-management is the cornerstone of diabetes care [7]. There are several studies [8, 9] that have reported that diabetes self-management is associated with improved diabetes knowledge, self-management behaviours and clinical outcomes. However, in a meta-analysis of diabetes self-management programmes, Norris et al. [9] reported sharp declines in benefits within one month-post intervention suggesting that self-management interventions alone do not enable individuals to maintain behaviours changes. Therefore, it is evident that the behaviour changes after the implementation of self-management programmes require the co-existence of several factors. Fisher et al. [10] suggested that the quality clinical care and self-management are compatible and dependent on each. Therefore, in the absence of sound care, individual’s efforts may be misdirected, and expert clinical care will fall far short of its potential. A number of studies have also suggested that patient understanding and beliefs about health and illness may be shaped by historical and local contexts [11], whether respondents are thinking about health or behaviours in general or about their own [12] and personal experience and observation. Internationally, the leading work in the field of diabetes self-management by the American Association of Diabetes Educators (AADE) has resulted in the identification of seven principle self-care behaviours. These include healthy eating, being active, monitoring, taking medication, problem-solving, healthy coping and reducing risks [13, 14]. The conceptual model in this research will address the self-management approach and barriers to self-management of middle-aged population of Pakistan with diabetes aged between 40-60 years in line with the latest estimates of International Diabetes Federation on the greatest number of people with diabetes is between 40-59 years [3]. The model will be built upon previous studies on diabetes self-management in Pakistan and be guided by the recommendations from other studies carried out internationally on self-management of type 2 diabetes. The main aim of this study is to explore the factors that may influence diabetes self-management and to present the potential outcomes and to develop a conceptual model for enhancing the type 2 diabetes self-management among the middle-aged population of rural area of Pakistan. Aims and ObjectivesThe primary aim of this study is to explore the factors that may influence diabetes self-management among the study population and to present the potential outcomes and to develop a conceptual model for enhancing the type 2 diabetes self-management among the middle-aged population of rural area of Pakistan.Research Questions1. What factors affect the diabetes self-management practices?2. Does socio-demographic influence the diabetes self-management?3. What social and religious beliefs influence the experience and practice of diabetes self-management?
2. Materials and Methods
2.1. Literature Search Strategy
- The following keywords were used during the literature search; “type 2 diabetes”, “diabetes knowledge and awareness”, “Diabetes health education”, “semi-structured qualitative interviews”, “quantitative analysis and self-management of type 2 diabetes.” All the retrieved articles were checked, and the articles that involved self-management of type 2 diabetes or diabetes knowledge or awareness were considered. This strategy led to the identification of 47 relevant articles.
2.2. Inclusion Criteria
- The initial literature search was broad enough to scope the quantity of contemporary qualitative research on the self-management of type 2 diabetes. The inclusion criteria for the articles was that they should be published in peer-reviewed journals between January 1993 to August 2013, should be related to self-management of type 2 diabetes, should use qualitative and quantitative methods and should be available in English language. The other inclusion criteria was the middle-aged population aged 40-60 years (specific interest in the population of Pakistan) with poorly controlled type 2 diabetes – in line with the highest number of diabetic patients within the age groups of 40-59 years reported by International Diabetic Federation (2). In addition, studies must report qualitative/quantitative research on diabetes self-management, diabetic complications, quality of life, and patient-doctor relationship or interaction.
2.3. Exclusion Criteria
- The articles were excluded if their focus was theoretical research only and were not related to diabetes self-management but otherwise related to diabetes.
2.4. Outcome of Interest
- The outcome of interest during the literatures review were qualitative descriptions or interpretations of personal view or social experiences in the local context on the self-management of type 2 diabetes, healthcare system use, quality of life and identification of knowledge gaps for future research. The outcome of interest from the quantitative studies was the measures of improved diabetes such as exercise self-care, improved physical activity, HbA1c and BMI which will be analyzed in quantitative studies to associate self-management programs with the outcome.
2.5. Characteristics of the Identified Literature
- In the selected 47 articles, participant sample size varied from n=9 (25) to n=500 (26) with the mean sample size of n= 54. Principles of grounded theory was most frequently used to interpret transcribed semi-structured interview and focus group data and, researchers were interested in facets of experience associated with having type 2 diabetes and in developing new theories from the analysis of participant accounts. In order to provide a contextualizing overview of the identified literature, an overall analysis of the literature reveals that the authors identified culturally mediated experiences of type 2 diabetes in terms of ethnic/cultural groups. The analysis also shows that researchers provided perspectives of newly diagnosed patients, discussed the ways in which people with diabetes perceived health care professionals and service delivery and the social construction of diabetes management. However, limited studies were found in the literature search on diabetes self-management highlighting the patient-doctor interactions. Most of the qualitative studies found in Pakistan are related to diabetes knowledge and awareness aimed at promoting the self-care of diabetes in that region. The quantitative studies focused on the association between diabetes self-management programs and improved clinical outcome. Out of the 47 identified studies, 41 studies from the literature search representing self-management in context, suggesting that the multiple contextual factors identified are fertile ground for further research. The studies also suggested that context should be given particular attention for researchers to gain understanding of the process of diabetes management. Two of the 41 studies that represented self-management in context were quantitative articles that investigate the association between social support and improved outcome. Four studies represented gender and self-management while 2 studies represented the physician-patient relationship. Three conceptual themes were identified from the analysis of the identified literature. These include (i) self-management in context, (ii) physician-patient interactions on self-management, (iii) Gender and self-management.
3. Results
- The Conceptual Model for the StudyThe model presented in Figure 1 provides a conceptual framework of self-management of type 2 diabetes. The model explores the relationships between the variables that influence the self-management of type 2 diabetes among the middle-aged population of Pakistan. The literature review informed that these variables can be grouped together into five categories: socio-demographic characteristics, behavioural and psychological characteristics, social support, cultural characteristics and barriers to self-management. These categories are identified in the conceptual model as related factors that may influence self-management of type 2 diabetes among the middle-aged population of Pakistan. The conceptual framework provides seven key interrelated components comprising the model and includes: socio-demographic characteristics (age, gender and education), behavioural and psychological characteristics (monitoring of blood sugar, Adherence to diet and physical activity), social support (family and friends), barriers to self-management (lack of knowledge, self-confidence, financial and family support), cultural characteristics (cultural beliefs, dietary preferences), Type 2 diabetes self-management (individual and community), and health outcomes (quality of life, HbA1c, Obesity, BMI and CVD risk factors). This model postulates that socio-demographic characteristics, behavioral and psychological characteristics, social support, barriers to self-management, and cultural characteristics impact Type 2 diabetes self-management. These factors together then predict health outcomes. In Pakistani culture, strong family bonds are important and highly valued [15, 16]. Medical treatment and decision should be made within the family members rather than by the discretion of an individual [17-19]. Thus, the model also assumes that self-management of type 2 diabetes primarily takes place within a family context, and both individuals and family members are influenced by Pakistani culture.
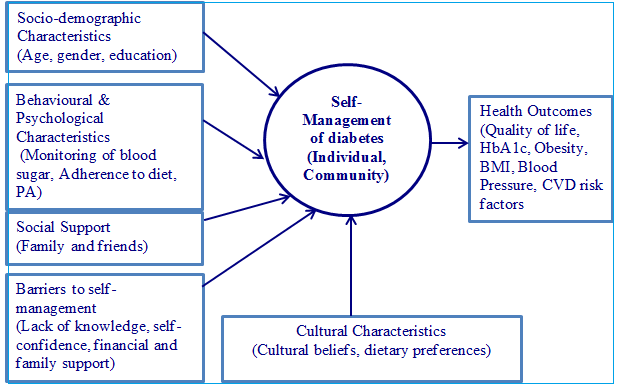 | Figure 1. Conceptual framework of self-management of type 2 diabetes |
4. Discussion
- The conceptual model presented here serves as an initiative for a better understanding, development, and testing of type 2 diabetes self-management interventions in the middle-aged population of Pakistan. The use of such kind of model reflecting cultural and social norms of the community that identifies the key variables influencing type 2 diabetes self-management and potential outcomes from effective management, may provide guidelines for future research and interventions. The future research work bridging the gap in knowledge, may be addressed by investigating the impact of cultural characteristics on type 2 diabetes self-management in Pakistani community. There is no quantitative study conducted in literature so far addressing that issue in local community. The strength of our study is that we have conducted systematic literature review to guide us to develop the conceptual model for type 2 diabetes. However, according to the Walker-Avant methodology [20], it does not require a systematic review when performing conceptual model development but such models may be subject to future modifications. In addition, our systematic literature review has demonstrated knowledge gaps, which can be used to guide future research and the knowledge gained from future research will help to modify the current conceptual model. Secondly, there have been no randomized controlled trials exclusively for the middle-aged population of Pakistani with Type 2 diabetes. The relationships reported in this model should be tested and verified by future intervention or clinical trials. Based on the review of the literature, the following conclusions can be drawn. First, more attention should be directed to family-focused interventions for Type 2 diabetes patients in Pakistan. There are a number of personal characteristics that are difficult to modify, including gender and linguistic barriers. Therefore, interventions that focus solely on personal characteristics may show little promise for successful self-management approach. Secondly, the effectiveness of interventions to improve family functioning should be tested for the impact on enhancing Type 2 diabetes self-management in Pakistani population. The conceptual model presented provides an important step to guide self-management of Type 2 diabetes in middle-aged population of Pakistan. The gap in the literature is problematic for the purpose of tailoring a self-management intervention for this population. With limited resources and inadequate utilization of health care service, self-management of Type 2 diabetes becomes a great challenge in rural area of Pakistan [21]. Although, the awareness of self-management of type 2 diabetes in Pakistani population is emerging, more research is needed to describe the family barriers to better self-care, to identify the predictors for effective self-management, and to test a culturally-appropriate randomized controlled trial that enhance self-management of type 2 diabetes [22]. The future research may be directed to apply this conceptual model to locate the most important determinants, which will be the first step to develop and test a much-needed self-management intervention study for this underserved group of patients in rural area of Pakistan.
5. Conclusions
- Self-management of type 2 diabetes is important for middle-aged population of rural area of Pakistan to achieve better diabetes related health outcomes. Self-management behaviours are influenced by multiple factors, including socio-demographic characteristics, behavioural and psychological characteristics, social support, barriers to self-management, and cultural characteristics. The relationships reported in this conceptual model should be tested and verified by future clinical trials. In addition, more research is also needed to identify the interactions between these factors. This conceptual model can be used to better understand the contextual determinants of behaviours which could facilitate in future the development of culturally appropriate interventions to support the self-management activities.