-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Diabetes Research
p-ISSN: 2163-1638 e-ISSN: 2163-1646
2017; 6(1): 24-33
doi:10.5923/j.diabetes.20170601.04

Evaluation of Oral Medication Adherence and Its Related Factors in Type II Diabetic Patients in Iran: A Systematic Review
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMahdieh Mashrouteh 1, Narges Khanjani 2
1Modeling in Health Research Center, Institute for Futures Studies in Health, Kerman University of Medical Sciences, Kerman, Iran
2Neurology Research Center, Kerman University of Medical Sciences, Kerman, Iran
Correspondence to: Narges Khanjani , Neurology Research Center, Kerman University of Medical Sciences, Kerman, Iran.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Many patients with diabetes do not take their medication according to schedule, while medical interventions in patients with type 2 diabetes can have a positive impact on clinical outcomes. In this systematic review, we identify the rate of adherence, and its determinants and interventions that can improve adherence to Diabetes Mellitus oral medications in Iran. Methods: We searched International and National electronic databases including Scopus, Web of Science, PubMed, Scientific Information Database (SID) and IranMedex on 14, May 2016 and we used the MeSH terms; “medication adherence” or “compliance” and “type 2 diabetes” and we restricted it for “Iran”. Studies were included in the review if they had reported the rate or score of adherence to diabetes mellitus oral medications in Iran. Quality assessment was performed using the STROBE checklist and Cochrane risk of bias tool. Results: The results of this systematic review indicated that medication adherence rates varied from 37.2% to 87%. The most frequent factors that had an effect on adherence were education level, age, the time interval between two visits, belief of drugs effectiveness and depression. Among the interventions, short message service (SMS) and telephone followup had the strongest effect on adherence. Median quality scores for observational studies was 19 and for clinical trials showed that more than half of them (4 out of 7) had a “high risk of bias”. Conclusion: This review shows that medication adherence in type 2 diabetes is lower than expected in Iran and we can improve it with SMS and telephone reminder messages and calls.
Keywords: Oral Medication, Adherence, Type 2 diabetes, Iran
Cite this paper: Mahdieh Mashrouteh , Narges Khanjani , Evaluation of Oral Medication Adherence and Its Related Factors in Type II Diabetic Patients in Iran: A Systematic Review, International Journal of Diabetes Research, Vol. 6 No. 1, 2017, pp. 24-33. doi: 10.5923/j.diabetes.20170601.04.
1. Introduction
- Adherence to (or compliance with) a medication regimen is described as the extent of prescribed medications by the physicians that patients take. Adherence rates for patients are usually defined as the percentage of the prescribed doses of the medication actually taken by the patient over a specified period of time [1].Adherence rates are higher among patients with acute conditions compared with chronic condition ones. Persistency among patients with chronic conditions is unfortunately low, decreasing mostly after the first six months of therapy [2].Adherence is determined by factors related to patients, conditions, socioeconomic status, the health system and therapy. Therefore, interventions which focus on improving medication adherence should aim all these factors, and the predominantly influenced one is the therapy-related component [3].A systematic review confirms that many diabetic patients take their medication less than the prescribed amount of it, in both Oral Hypoglycemic Agent (OHA) and insulin therapy. This study showed that 6–24 months after starting the medication, patients’ adherence to OHA therapy ranged from 36 to 93% [4].Evidence from the included studies suggests that pharmacist interventions directed at patients with type 2 diabetes can have a positive impact on clinical outcomes, as demonstrated by reduction in A1C, blood glucose, blood pressure, and BMI and by improvement in the lipid profile observed in the intervention group during the follow-up period in almost all studies [5].For acquiring glycemic control and preventing diabetic complications, pharmacologic management is necessary. Each patient with type 2 diabetes (T2DM) needs specific treatment that could manage cardiovascular disease risk factors, macro and micro vascular complications, and the risk of severe hypoglycemia [6].Factors affecting adherence to medications in T2D include smoking, depression, poly pharmacy, convenience of obtaining and administering the medication, patient motivation and education [7]. Also, there is a causal relationship between quality of life and adherence to diabetes treatments [8].Interventions to promote medication adherence should focus on simplifying treatment regimens and improving provider–patient communication and education [7].A review showed that SMS interventions can be most effective for management of type 2 diabetic patients [9]. Also, another review has suggested, electronic monitoring systems were useful in improving adherence for individual patients [4].In this study, we performed a systematic review to find the rate and determinants of adherence to Diabetes Mellitus oral medications in Iran. We also reviewed publications of interventions that improve adherence to oral medications in patients with type 2 diabetes mellitus (DM).
2. Methods
- We searched International and National electronic databases including Scopus, Web of Science, PubMed, Scientific Information Database (SID) and IranMedex.Search strategyWe used MeSH terms “medication adherence” or “compliance” and “type 2 diabetes”. In International databases, we used “Iran*” to restrict our search and in National databases, search was carried out using English keywords and their Farsi equivalent terms. Also, we searched “ganjirandoc.ac.ir” database for thesis and “allconferences.com” for conference abstracts.There were no restrictions for time, type of publications or language. All database searches were done on 14 May 2016.Study selectionAll records were retrieved from the databases and two independent researchers screened the title and abstract of each record to find relevant publications. Disagreements were resolved by discussion. Studies were included in the review if they had reported the rate or score of adherence to DM medications in Iran regardless of the compliance/adherence definition criteria. Also, we considered studies about the determinants of medication adherence and interventions to improve it. Studies that reported only “self-care” in type 2 DM were excluded from the review.After the screening phase, the full-text of relevant articles was retrieved and evaluated. Decisions were made about including the studies by consensus.Quality assessmentQuality assessment was performed using an adapted version of the STROBE checklist for cross sectional studies [10] and the Cochrane risk of bias tool for clinical trials [11]. Data extraction and analysisTwo independent researchers reviewed the full text articles according to the inclusion–exclusion criteria.If articles were eligible for the study, then reviewers would extract data such as study characteristics, study design, adherence to medication (AM), definition and rate, the AM measurement tool (self-report, pill count, refill data, electronic medication monitors, or biological assessments), and AM determinants that were reported.
3. Results
- In this review, we found 193 related articles which 21 articles were excluded in full text screening and 19 were eligible for data extraction. (Figure 1).Eleven out of 19 were in Farsi language and 10 of them were done with cross sectional design. Summary of the basic characteristics of articles can be seen in table 1.We extracted data from 19 studies. These studies were published from 2005 to 2015. The range of their sample size was from 60 to 371.We understood that there was not a unified definition for medication adherence in these studies. About half (nine) of the articles did not state the definition of coherence in their article; and other ones categorized medication adherence into two to four groups and the criteria for categorizing people were different in each article. Most of the studies used standard measurement tools for adherence, only two studies used pill counting method and one study used a researcher made questionnaire.We could not do a meta-analysis to estimate the pooled adherence rates or scores, because of the variety in the type of reporting, categorizing and data analyzing. (Table 2 and 3)In studies that reported medication adherence rates, these rates varied from 37.2% to 87%.We reported the factors related to medication adherence in table 2. The most frequent factors that had an effect on adherence were education level, age, the time interval between two visits, belief of drug effectiveness and depression.The most effective promoting factors (from the factors that a correlation had been reported for them) were extroversion and a powerful health locus of control (r=0.3); and the strongest factors with negative effects were depression, and weak general memory (r= -0.5 and -0.3 respectively).Interventions and their effects on medication adherence have been shown in Table 3. It seems like SMS and telephone followup messages and calls had the strongest effect on adherence.Quality scores calculated based on the STROBE checklist for observational studies ranged from 17 to 21 (Median=19, Mean=18.6) out of a total of 22 possible items (0.5 points given for partial reporting). Also, we checked the quality of clinical trials by the Cochrane risk of bias tool that categorized studies to “low risk of bias” (1 study), “high risk of bias” (4 studies) and “unclear risk of bias” (2 studies). (Table 4)
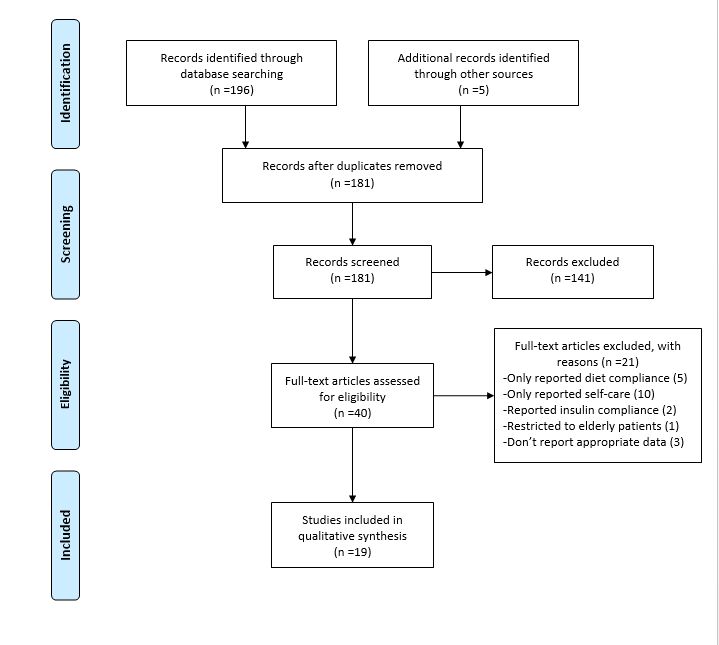 | Figure 1. Flow Diagram of study selection |
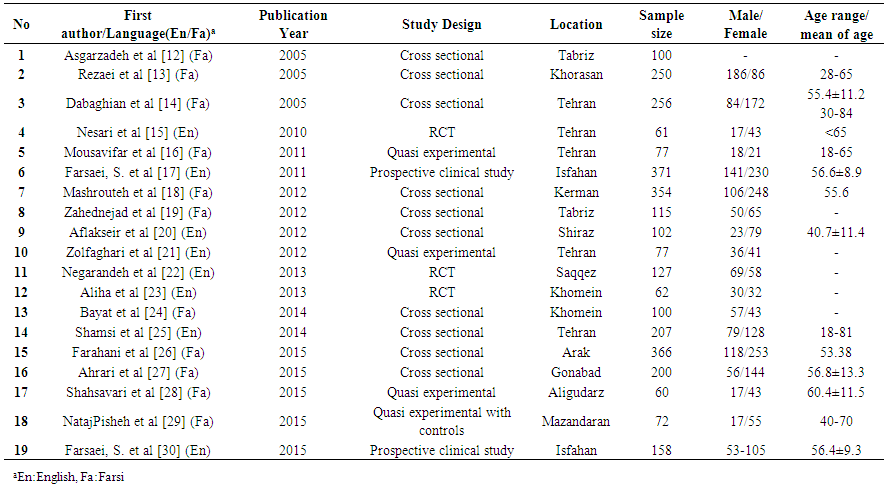 | Table 1. Summary of basic characteristics of studies (Table of primary studies) |
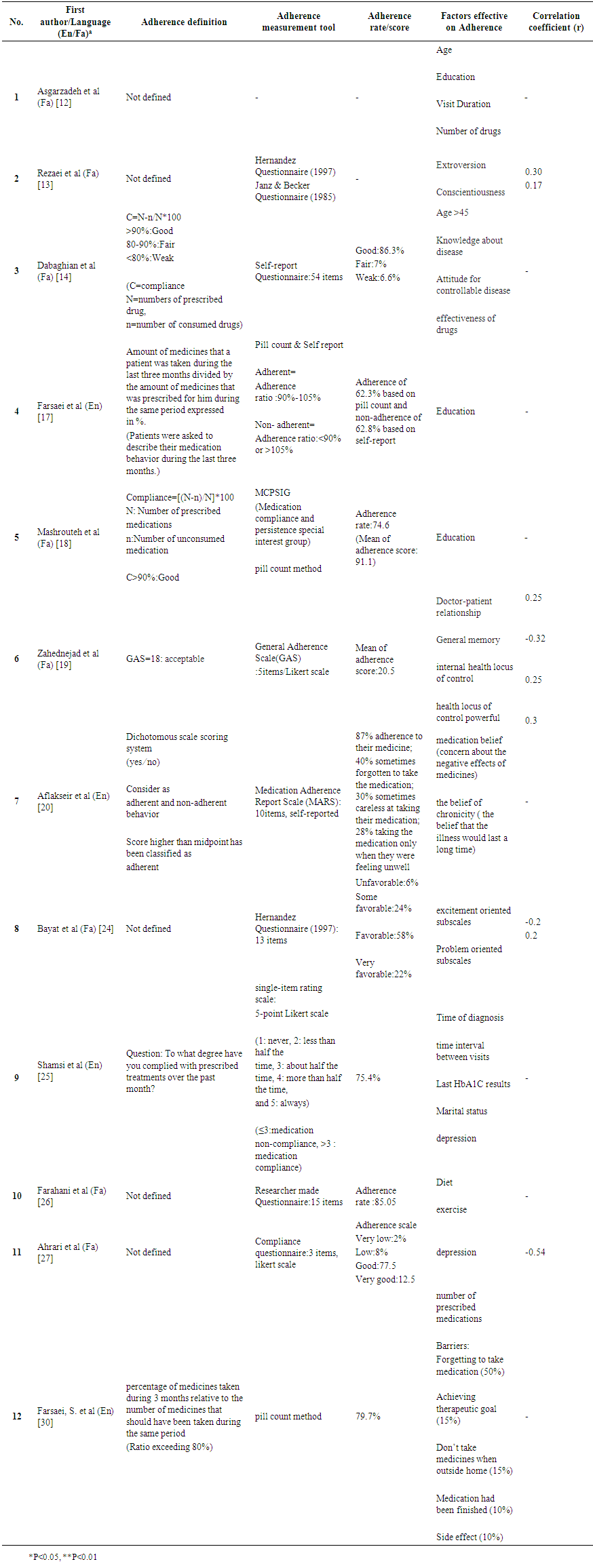 | Table 2. Summary of the result of observational studies about adherence |
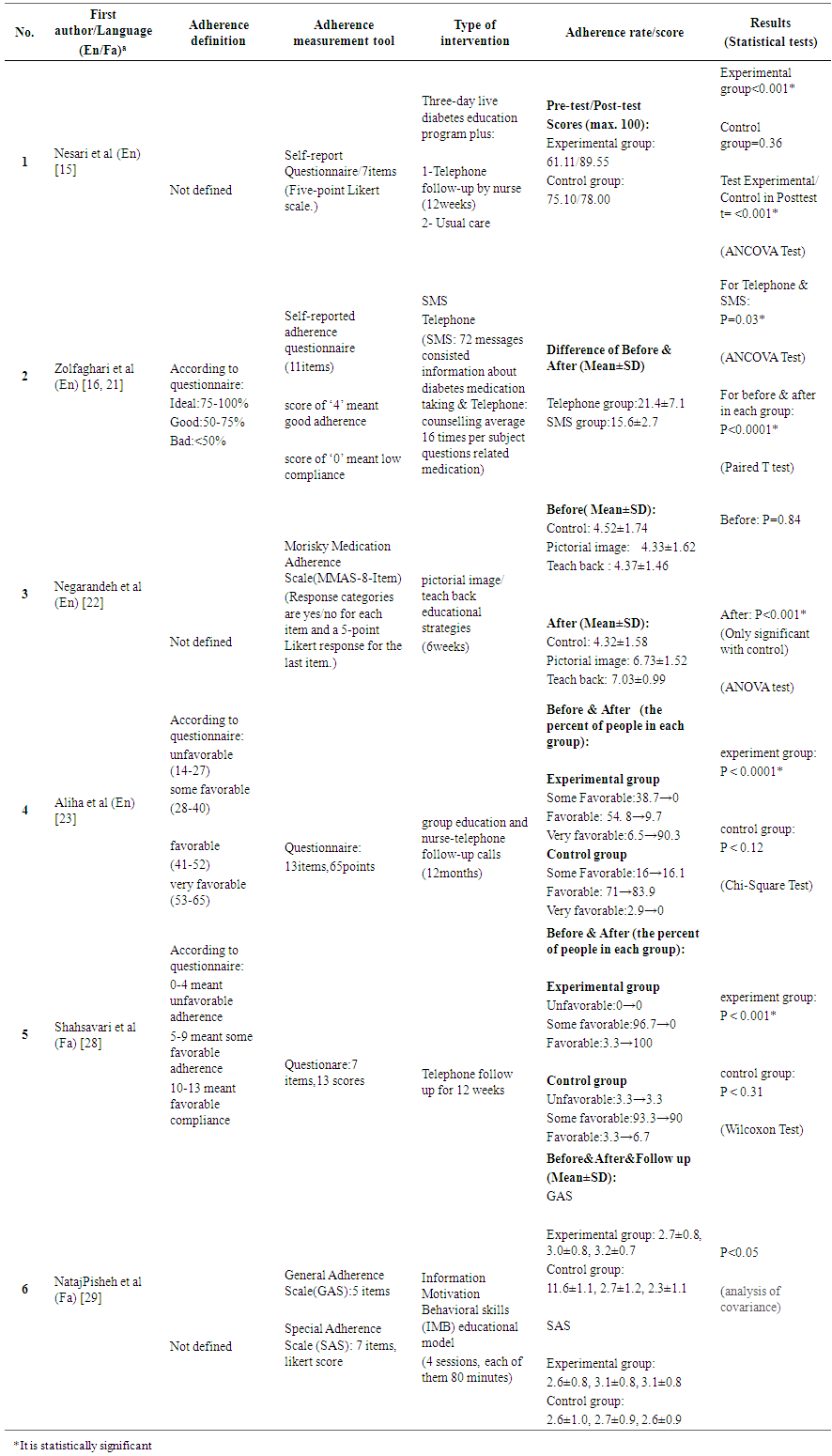 | Table 3. Summary of the result of clinical trial studies about adherence |
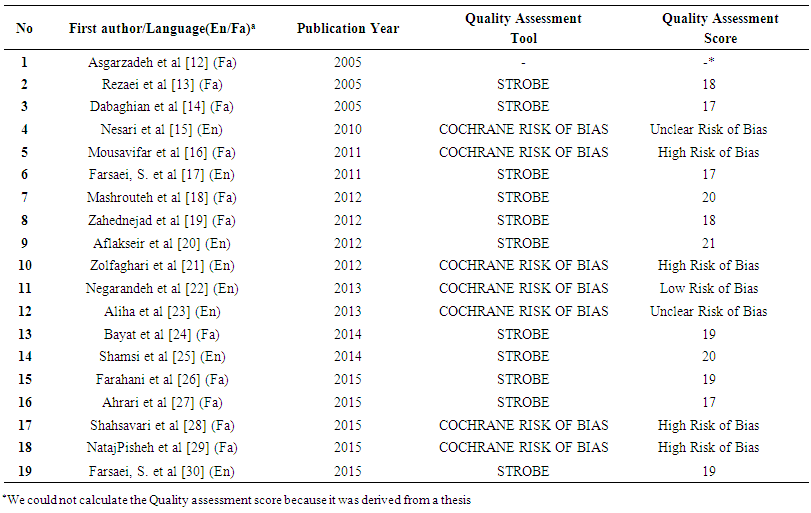 | Table 4. Quality assessment of the studies |
4. Discussion
- This systematic review shows that many patients with diabetes in Iran took less than the prescribed amount of oral medication.Although obvious evidence shows that diabetes management (including diet, exercise, and adherence to medications) decrease diabetes complications about 53–63% and also 46% reduction in mortality [31], studies reported a wide range for adherence in Iran. In a systematic review that was conducted in 2015, and included 27 original studies, the prevalence of adherence to oral and insulin therapy in type 2 diabetes ranged from 38.5 to 93.1% and only in 22.2% of the world studies, the adherence rate was more than 80% among the studied population [32]. Also, another systematic review based on 20 reports in 2004 showed that adherence to oral hypoglycemic agent therapy in diabetic patients ranged from 36 to 93% [4].The existing methods for adherence measurement can be classified into direct and indirect methods. There is not any gold standard method and each method has its advantages and disadvantages. Direct methods include observed therapy and detection of a drug or its metabolite concentrations or a biologic marker that has been added to the drug, in blood or urine. Direct approaches are expensive, difficult for the health care provider, and may be manipulated by the patient. Indirect methods of adherence measurement include questioning the patients about using their prescribed medication via a questionnaire or diary, pill counting, revealing rates of refilling prescriptions, using electronic medication monitors and measuring physiologic markers. These methods seem to be are easy to use, but can be lead to bias and overestimation of patient adherence [1].In this systematic review, all studies applied indirect methods that may have led to unreliable results. It is recommended to measure adherence with one of the direct methods to show the real medication adherence. In this study, the most reported repeated factor that had a positive effect on medication adherence in type 2 diabetic patients was education. In addition to that some factors such as age, visit duration, belief in drug’s effectiveness, and depression, were more frequently mentioned in papers than others.In a cohort study that was done on 2015, patients who were younger, new to diabetes, and on a few other medications were more at risk for non-adherence [33]. Higher income and depressive symptoms were significant independent determinants of medication non-adherence in young adults with type 2 DM that were reported in another study [34].A medication adherence survey that was made available on WebMD showed that patients who reported receiving verbal and written education from their healthcare staffs had greater adherence but those with diabetes for longer than 2 years were less affected by education. Also in women and older people education had a greater effect on adherence [35].Our study showed the most interventions that were done for improving adherence, were telephone and SMS (short message service) follow up which were highly effective on oral medication adherence.In two studies, significant changes were not seen between groups that were prompted with SMS and telephone. However, there were significant differences from pre to post test in each group for adherence to medication [16, 21]. In another two articles, a nurse-led telephone prompt was effective in enhancing the level of adherence to a diabetes therapeutic regimen [15, 23].Some studies showed the positive impact of SMS prompts on medical adherence in diabetic patients [36, 37], but there was a study that showed using SMS messages failed to increase adherence [38].In this systematic review, two studies used an educational model as an intervention to improve medication adherence and in both of them, education had positive effects [22, 29]. In Nigeria, a regular combined education program influenced patients’ medication adherence positively [39], but in Korean immigrants in the USA, educational programs on diabetes self-management showed no impact on medication adherence [40]. According to a systematic review that was done in 2015 including 49 studies and 40 interventions, a large number of interventions (27 articles, about 58.5% of studies) failed to show a positive impact on medication adherence. It is therefore very difficult to understand and predict what type of interventions will be the most effective in improving adherence to anti-diabetic medications, but some interventions could be used alone or in combination with other interventions to improve the outcome of patients [41].Based on quality assessment, we think that the quality of the observational studies was relatively acceptable, but we could not rely on the trial results.This review has some limitations. Studies included in this review were not excluded based on their quality. Also, since the method most frequently used to determine medication adherence was self-report, we could not completely trust the results either.
5. Conclusions
- Medication adherence in type 2 diabetes is lower than expected in Iran and the best interventions for improving it are SMS and telephone (message and call) reminders including recommendations about using their drugs.