-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Diabetes Research
p-ISSN: 2163-1638 e-ISSN: 2163-1646
2016; 5(6): 141-146
doi:10.5923/j.diabetes.20160506.04

Diabetic Education Reduces Blood Pressure, Kidney Function and Glycemic Level in Central Hospital Nampula
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMadhumati Varma
Consultant Internist, Diabetologist, Working for Ministry of Health Mozambique, Central Hospital Nampula, Nampula, Mozambique
Correspondence to: Madhumati Varma, Consultant Internist, Diabetologist, Working for Ministry of Health Mozambique, Central Hospital Nampula, Nampula, Mozambique.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Diabetes is a chronic disease, uncontrolled blood sugar long period of time can complicate to hypertension, which is estimated 70-80% of population of diabetes. The uncontrolled hypertension in diabetes, is one of major risk factor to develop microvascular and macrovascular and chronic renal diseases. A clinical intervention study was carried out of 648 participants of diabetes in consultation of diabetes in central hospital Nampula. There were three sessions of education on an interval of one month, at baseline, at first follow up and at second follow up, participant being measured blood pressure on each visit and results of analysis of blood urea, creatinine and fasting blood sugar recorded which were done 2-3 day prior to following education session. The studies found, that there were significant decreased in blood pressure from baseline means of 131.02/71.73 mmHg to second follow up 120.95/68.79 mmHg with a standard deviation from baseline 24.35 mmHg/14.66 mmHg to second to follow up 19.95 mmHg/11.33 mmHg, blood urea and serum creatinine significantly decreased from baseline to the second follow up (P <. 001). The dependent variable fasting blood sugar found significantly (P=. 05) at baseline, at first follow up (P=. 005) and at second follow up (P=. 005) by post hoc Turkey test on compared with independent variables of blood pressure, blood urea and serum creatinine. The clinical educational intervention was highly effective against controlling blood pressure, blood urea and creatinine among participants of diabetes mellitus in the present study.
Keywords: Diabetes Mellitus, Blood pressure, Blood urea and creatinine, Effect education, Control, and participants
Cite this paper: Madhumati Varma, Diabetic Education Reduces Blood Pressure, Kidney Function and Glycemic Level in Central Hospital Nampula, International Journal of Diabetes Research, Vol. 5 No. 6, 2016, pp. 141-146. doi: 10.5923/j.diabetes.20160506.04.
Article Outline
1. Introduction
1.1. Background
- The diabetes mellitus is a chronic disease, causes chronic kidney disease 25-40 % of patients of diabetes type1 and 5-40 % of patients of diabetes type 2. [2] There is a correlation between blood pressure control and prevention of diabetic nephropathy. Hypertension is linked to metabolic syndrome. The blood pressure reduction in patients with diabetes prevents microalbuminuria which is a strong risk factor of Diabetic nephropathy. The ACE inhibitor and angiotensin receptor antagonists’ drugs of choice to control blood pressure and prevent microalbuminuria in diabetic patients. Diabetes, type 2 majors causes of hypertrophy of glomeruli due to increase glomerular filtration in uncontrolled glycemic control with patients with diabetes, which damages the kidney and accumulation of glycosylated ends products on the glomerulus. This mechanism initially causes selective protein filtration by basal membrane of glomerulus followed by nonselective proteinuria. Initially compensatory hyper function of glomerulus filtration followed by de-compensatory functioning of glomerulus. Finally, reduction in glomerulus filtration and renal failure. There is very important to prevent early stages of renal damage by controlling blood pressure and glycemic control.The patients with diabetes of central hospital Nampula, have poor knowledge of nonpharmacological treatment of diabetes, low and medium economic condition, non-availability of diabetic educator, completely depends on pharmacological treatment. The result of biochemical results shows some of patient’s have evidence of chronic renal failure. There is a strong need to arrange an educational session for increase knowledge of diabetes to better control of glycaemic, blood pressure and urea and creatinine. It is clear that when diabetic patients only utilize pharmacological treatments that it is not sufficient to control diabetes and complication [1].
2. Method
- Sample number and characteristicsThe study was conducted on basis inclusion and exclusion criteria’s of selecting a sample of 648 of participants in central hospital Nampula, for duration of 2 years. There were three education session at baselines, at first follow up and at second follow up.Organization of education sessionsThere were educator’s diabetologist, dietician, psychologist, physiotherapist, and diabetic nurse. The diabetic nurse took consent and accessed the patient’s clinical history before conducting a physical examination that included checking vital signs and fasting blood sugar. The physical examination was to be done by a physician and also noted the results of a fasting blood sugar, urea and creatinine analysis that tested, which had been conducted 2-3 days prior to the education session of baseline, first follow up and second follow up. Method of educationThe education sessions were in the form teaching, discussion and presentation. Topic for education taken brief overall knowledge of diabetes, diet, exercise, psychological, according to culture and socioeconomic need for a local population of Nampula.A Data was analyzed SPSS 17 version, and graphs made in Excel software.
3. Results
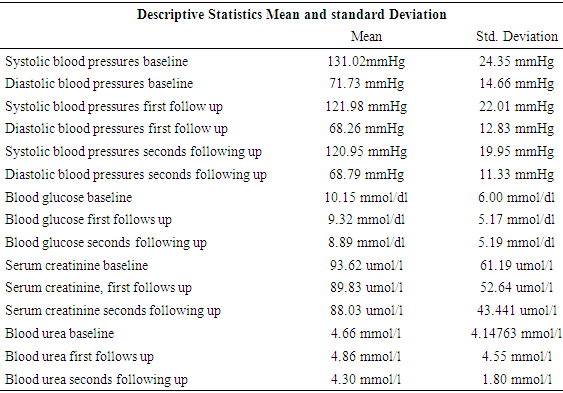
- The participants of central hospital Nampula of diabetic OPD, a sample of 648 was taken for study. The principal variable studied blood pressure, fasting blood sugar, urea, and creatinine from baseline to second follow up session of education. Summary table of descriptive Statistics Mean and standard Deviation:
|
|
|
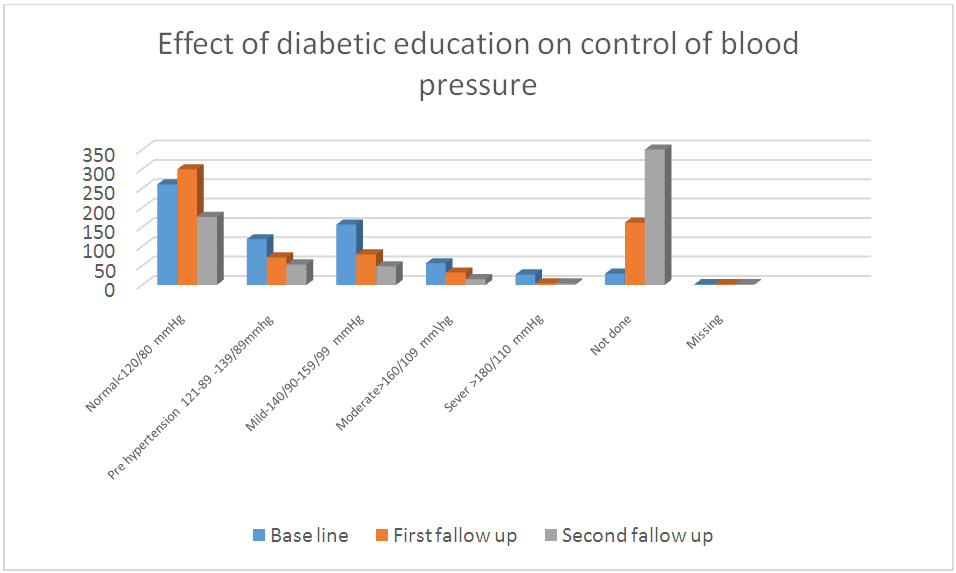 | Figure 1. Bar chart: In the above charts we see that distribution of the compared blood pressure at baseline, first follow up, and second follow up after diabetes education among participants |
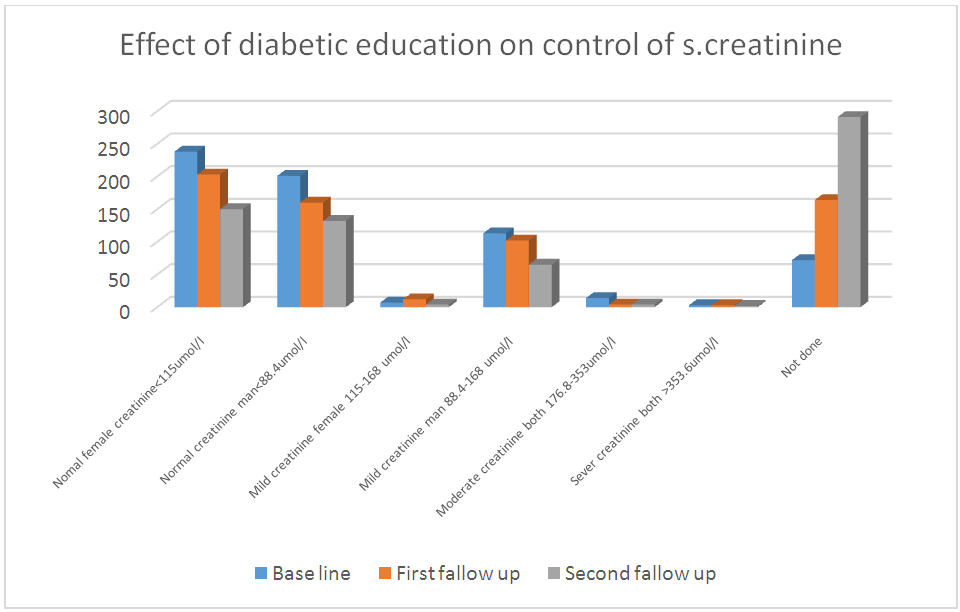 | Figure 2. Bar chart: In the above charts we see the distribution of the compared blood creatinine scores at baseline, first follow up and second follow up after diabetes education among participants |
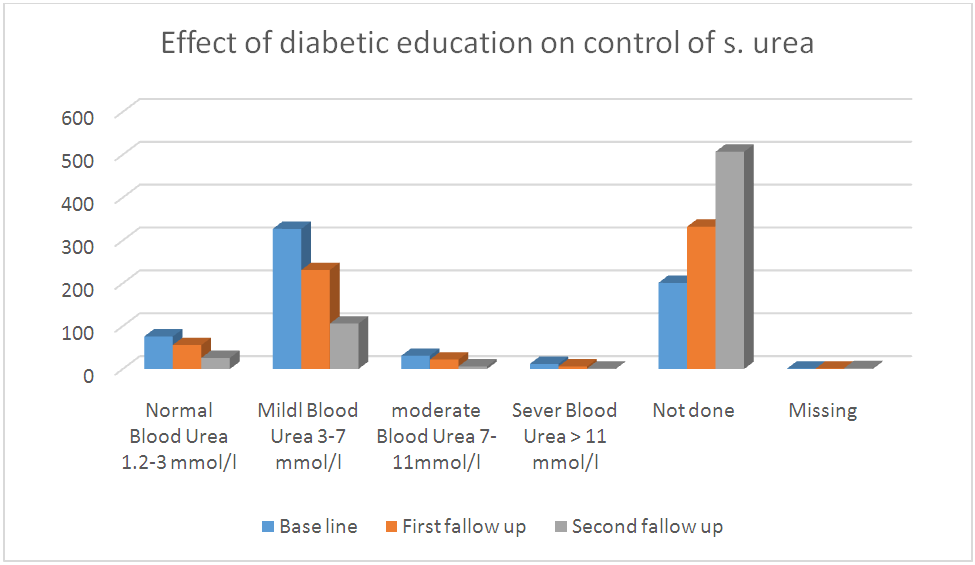 | Figure 3. Bar chart: In the above charts we see the distribution of the compared blood urea scores at baseline, first follow up, and second follow up after diabetes education diabetes among participants |
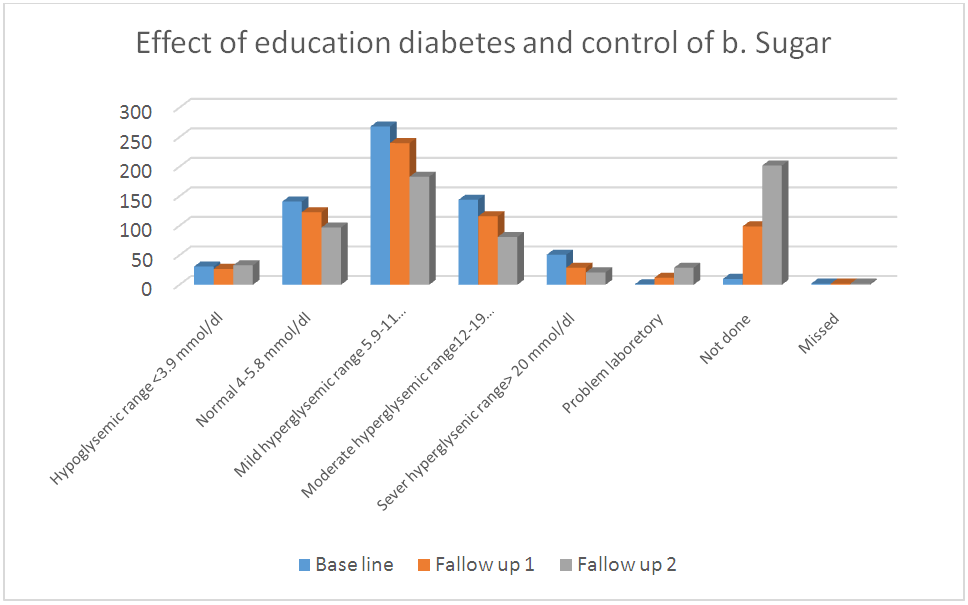 | Figure 4. Bar chart: In the above charts we see the distribution of comparing fasting blood sugar scores at baseline, first follow up, and second follow up after diabetes education among participants |
4. Discussion
- The blood pressure, urea, creatinine and fasting blood sugar was significantly improved after educational intervention in the present study. The knowledge provided by the education helped the participants gain good knowledge of education of diabetes by instructor and implemented in their lifestyle which confirmed by result of analysis. The previous studied which showed similar results, a Cochrane review [9] concluded that a reduction in blood sugars concentrations positive correlated with increased knowledge of diabetes. A Cochrane review [8] concluded that from group education of diabetes patients get motivated, start adherence to treatment and understand diabetes. In order to promote diabetes awareness, self-care behaviors can be useful [8] to described innovative strategies for the improvement in diabetic control in Chinese patients through the continuing education of diabetes mellitus during patient examination and by increasing family involvement via diabetic knowledge [3], also emphasized repeated diabetic education sessions to improve metabolic parameters [4]. Another study had been done on an experimental and control diabetes, pre and post-test to see knowledge gain of diabetes, showed reduced in Systolic and diastolic blood pressure [7]. There are no study on diabetic education and effect on urea and creatinine. However some studies taken on education effect on prevent diabetic nephropathy. The education of diabetes in dialysis unite showed significantly improvement in lifestyle and glycemic control [10]. The severe kidney function can be prevented by control of blood pressure of diabetic patients [11]. The control of renal function, needs control of blood sugar and blood pressure to prevent renal complication in patients of diabetes [12]. There are other study which recommended complex carbohydrate should consume 50-60% of total calories intake of patient of diabetes to control diabetes and prevent renal function and its impairment. To slow the progression of kidney complications, protein intake should be limited to 0.8-1 g/kg IBW/d [13]. The sedentary lifestyles, obesity and aging increases complication of diabetes [17]. The study showed patients ability to do self-carrying and improve control of diabetes [18].
5. Conclusions
- The Diabetes education, in central hospital Nampula carried out in three education sessions were organized, at an interval of one month (baseline, first follow up and second follow up). Each participant was evaluated in each session regarding their blood pressure, blood sugar, urea and creatinine. The statistical analysis showed strong significantly positive effects on controlling of kidney functions. The control of blood sugar with blood pressure, urea, and creatinine significantly correlated. The major risk factor of development of chronic renal failure of diabetic patients reduced by improvement on blood pressure, urea, creatinine and fasting blood sugar of participants.
6. Motivational Quotes
 There should be national policy on compulsory education session for new patients and continues education program for patients with diabetes to make healthy behavioral changes in order to control their diabetes and reduce the occurrence of renal complications.There was the weakness for the study some of the patients believe traditional medicine, nonadherence, sometime non availability of biochemical results from the laboratory, poor patient totally depends on government pharmacy and economic condition, not permitted to buy adequate food which recommended to diabetic patients, nonadherence of treatment, irregular follow up. Patients who lived district, distance from the hospital, not able to regularly attend three education sessions.One of the strengths of this study is that patients, follow instruction in motivation based on need and demands of patients.
There should be national policy on compulsory education session for new patients and continues education program for patients with diabetes to make healthy behavioral changes in order to control their diabetes and reduce the occurrence of renal complications.There was the weakness for the study some of the patients believe traditional medicine, nonadherence, sometime non availability of biochemical results from the laboratory, poor patient totally depends on government pharmacy and economic condition, not permitted to buy adequate food which recommended to diabetic patients, nonadherence of treatment, irregular follow up. Patients who lived district, distance from the hospital, not able to regularly attend three education sessions.One of the strengths of this study is that patients, follow instruction in motivation based on need and demands of patients. Contribution to Knowledge
- This study helped a patient to increase knowledge of diabetes and improvement in status of control of various aspects of diabetes.
Suggestion for Future Research
- However, future studies could be done on patient those chronic renal failure, on dialysis, in various levels of health care system.