-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Diabetes Research
p-ISSN: 2163-1638 e-ISSN: 2163-1646
2016; 5(4): 70-74
doi:10.5923/j.diabetes.20160504.02

A Study of Effect of Metformin and Gliclazide with and without Atorvastatin on Intimal Medial Thickness of Common Carotid Artery in Patients of Type 2 Diabetes Mellitus
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNavneet Kaur1, Jaswant Rai1, Sohan Singh2
1Department of Pharmacology, Government Medical College, Amritsar, India
2Department of Radiodiagnosis, Government Medical College, Amritsar, India
Correspondence to: Navneet Kaur, Department of Pharmacology, Government Medical College, Amritsar, India.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Aim: To evaluate the effect of metformin and gliclazide with and without atorvastatin on Glycemic control, Diabetic dyslipidemia and Serum C-reactive protein levels and their relationship to intimal medial thickness of common carotid artery. Materials and methods: In a prospective, double-blind, parallel and placebo-controlled study, type 2 diabetes mellitus patients randomized to either tab. Gliclazide 40 mg/day, metformin 500mg/day and atorvastatin 20 mg/day or tab. Gliclazide 40 mg/day, metformin 500mg/day and a matched placebo for a period of 24 weeks. Changes from baseline in fasting blood glucose (FBG), glycosylated haemoglobin (HbA1c), lipid profile, including total cholesterol (TC), LDL-C, high-density lipoprotein cholesterol (HDL-C), triglycerides (TG), C–reactive protein (CRP), intimal medial thickness (IMT) and liver enzymes (SGOT, SGPT) were observed.Results: Patients receiving metformin, gliclazide and atorvastatin had significantly greater percent reduction in TC (12.49%), TG (8.29%), LDL-C (18.58%), IMT (11.02%) and CRP (7.63%) and significant increase in HDL-C (10.11%) as compared to patients receiving metformin, gliclazide and placebo (p<0.0001). No significant differences were found in FBG and HbA1c levels between two groups (p>0.05). Change in intimal medial thickness showed significant positive correlation with change in CRP.Conclusions: The present study has indicated that this combination is more useful and beneficial for diabetic patients in lowering raised blood glucose levels within normal range and to prevent its various complications concurrently.
Keywords: Atorvastatin, Gliclazide, Intimal medial thickness, Metformin, Type 2 diabetes etc
Cite this paper: Navneet Kaur, Jaswant Rai, Sohan Singh, A Study of Effect of Metformin and Gliclazide with and without Atorvastatin on Intimal Medial Thickness of Common Carotid Artery in Patients of Type 2 Diabetes Mellitus, International Journal of Diabetes Research, Vol. 5 No. 4, 2016, pp. 70-74. doi: 10.5923/j.diabetes.20160504.02.
1. Introduction
- The prevalence of diabetes is rapidly rising all over the globe at an alarming rate. The status of diabetes has changed from being considered as a mild disorder of the elderly to one of the major causes of morbidity and mortality affecting the youth and middle aged people. [1] India has the world’s largest diabetic population. ICMR-INDIAB national study reported that there are 62.4 million people with Type 2 DM and 77 million people with pre-diabetes in India which is projected to increase to 101 million by the year 2030. [1, 2]According to ATP NCEP III guidelines, diabetes mellitus has been considered as cardiovascular equivalent. Diabetic patients are more prone to suffer from dyslipidemia and arterial hypertension, thereby increasing the risk of atherosclerosis which is the key factor in genesis of narrowing of lumen of blood vessels, ultimately leading to MI and stroke. [3] The key process in atherosclerosis is intimal medial thickening and lipid accumulation. In diabetic patients with sustained hyperglycemia, nonenzymatic glycation of apolipoproteins and other arterial proteins occur that may alter their function and have propensity to accelerate atherogenesis. [4] As a consequence of postprandial hyperglycemia, hypertriglyceridemia is induced. This suggests that improving glycemic control might reduce the inflammatory response supporting the link between inflammation and glucose metabolic disturbance. [5]Thus, management of this disorder is not only to lower raised blood glucose levels within normal range but also to prevent its various complications concurrently. The research is towards the development of treatment modalities which can decrease the atherosclerosis, thereby widening the lumen of blood vessels. Lipid lowering agents are usually prescribed with oral hypoglycemic agents. The present research work was planned to study the effect of atorvastatin as add on therapy to gliclazide and metformin combination on glycemic control, dyslipidemia and Serum C-reactive protein levels and their relationship to intimal medial thickness of common carotid artery.
2. Material and Methods
- Sixty type 2 diabetes mellitus patients in the age group of 35-60 years, male or female subjects with HbA1c levels > 7.0% and < 10% attending outpatient department of Medicine of Guru Nanak Dev Hospital Amritsar were recruited in the present study. Exclusion criteria: The diabetic patients with severe hypertension, significant valvular disease, history of myocardial infarction, stroke and coronary artery bypass surgery within the past 6 months, pregnant and lactating mothers, H/O renal, hepatic disease and muscle pain (fibromyalgia with associated raised CPK levels) and patients who had not received statins therapy for >3 months during previous 12 months were excluded. Participants of the study were made aware of the nature and purpose of this study and written informed consent was obtained. The study was conducted after obtaining approval from the Institutional Ethical Committee.Study DesignThe study was a randomized, double-blind, parallel, prospective and placebo-controlled. 2 groups of 30 patients each were formed randomly. Randomization was done by a pseudo number generation technique. The patients received either tab. gliclazide 40 mg/day, metformin 500mg/day and atorvastatin 20 mg or tab. gliclazide 40 mg/day, metformin 500mg/day and a matched placebo for 24 weeks. The modification in dose of metformin and gliclzide was guided by fasting blood glucose concentration. The patients were advised to continue with their dietary modifications and physical activity and they were explained the schedule of the drug treatment. Parameters of StudyAfter getting initial baseline, overnight fasting blood glucose, HbA1c, lipid levels (TC, LDL- C, HDL-C & TG), CRP, intimal medial thickness (IMT), SGOT and SGPT at the start (week 0) and subsequent levels were obtained at 24th week of the study. Fasting blood sugar was measured every 2 weekly using standard techniques on samples obtained from the subjects after overnight fasting. Lipid parameters namely serum highdensity lipoprotein cholesterol, serum triglycerides, and total cholesterol were measured using standard methods. Low-density lipoprotein cholesterol levels were calculated using Friedewald’s formula. CRP by Particle enhanced immunoturbidometric test with CRP Turbilatex kit and intimal medial thickness of common carotid artery was done by using a high resolution B mode ultrasound system ENVISOR (Phillips) version B.0.1 having an electrical transducer midfrequency of 7.5 mHz.Statistical analysis The blinding was opened at the end of the study and the patients who received metformin, gliclazide and atorvastatin were included in group I and those who received metformin and gliclazide and placebo in group II. The data generated was evaluated and expressed as mean ± SD of each variable. Paired student’s ‘t’ test within the group and unpaired ‘t’ test was applied when 2 groups were compared after completing the treatment. Pearson correlation coefficients were computed to assess any association between various parameters at baseline and at the end of the study.
3. Results
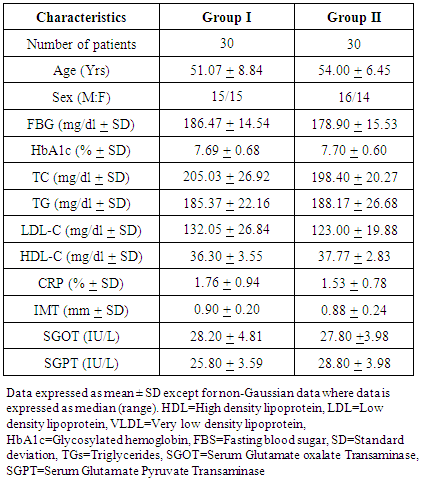
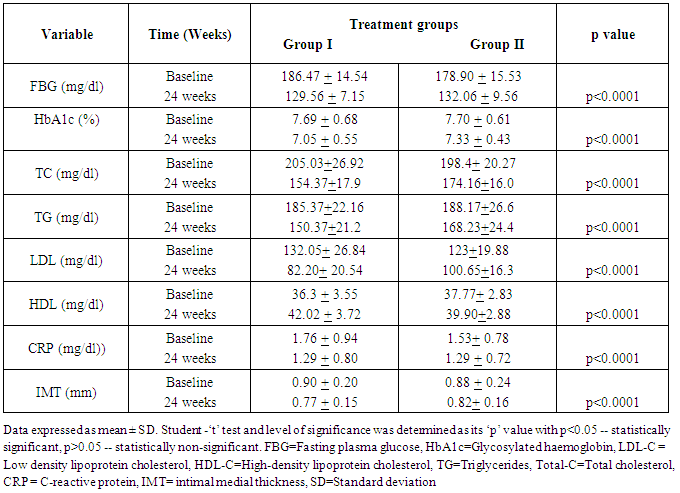
- A total of 60 patients were enrolled in this study. The baseline characteristics in two groups were comparable at the beginning of the study. As shown in [Table 1], baseline glycemic control, lipid profile, CRP and intimal medial thickness did not differ significantly in both groups. At the end of 24 weeks, there was a highly significant (p<0.0001) decrease in FBG and HbA1c levels in both groups. [Table 2]
|
|
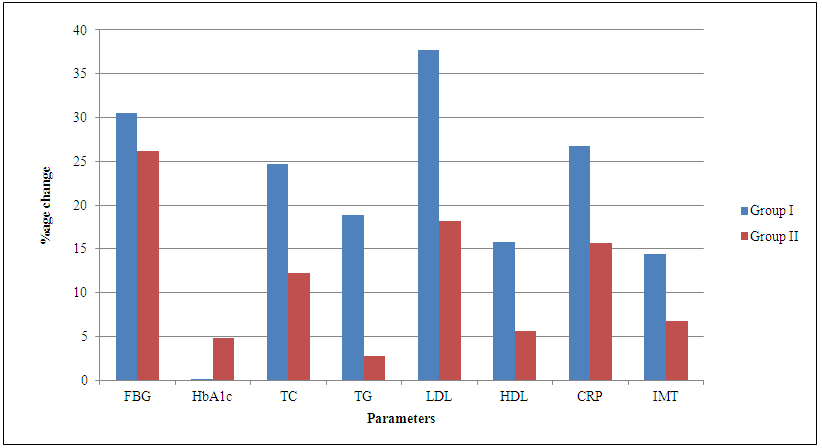 | Graph 1. Intergroup comparison of various parameters after 24 weeks |
4. Discussion
- FBG: In both groups, FBG levels decreased by 30.52% and 26.18% respectively after 24 weeks of treatment. Mean change in both the groups were statistically significant (p<0.0001) [Table 2]. The decrease in FBG in group I was more as compared to group II, although statistically non-significant (p>0.05). The fall in FBG in group II is similar to the fall reported by Lawrence JM et al and Vipul S et al. [6, 7] HbA1c: There was statistically significant decrease in the levels of HbA1c (p<0.0001) in both groups. The difference in decrease is not statistically significant (p>0.05) [Table 2]. Ristic S et al reported a mean change of 0.27% in HbA1c with use of metformin and gliclazide for 24 weeks which is lower than that observed in group II of present study. [8] The study by Vipul S et al has pointed out that atorvastatin has favorable effect on glycemic control and perhaps that is why high reduction in FBG levels and HbA1c were observed in group I as compared to group II in present study. [7]Lipid profile: The mean change in serum TC, TG, LDL-C and HDL-C in group I was significantly greater as compared to group II at end of the study (p<0.0001) [Table 2]. Charbonnel et al reported 7% fall in TG and 7% rise in HDL in patients on metformin and gliclazide combination therapy. [9] Tan KC et al reported that atorvastatin caused reduction in TC, LDL-C and TG by 32.94%, 50.1% and 23.1% respectively and increase in HDL by 2.6%. This reduction in TC, TG and LDL was higher but rise in HDL was less as compared to observations of the present study. [10] The increase in HDL is almost similar to the rise 15% as reported by Empen K et al in patients of diabetic dyslipidemia with the use of atorvastatin. [11] So it can be concluded that combination of atorvastatin with metformin and gliclazide is more effective in reducing the TC, TG, LDL-C and in raising HDL-C.CRP: A significantly greater reduction in the levels of CRP (p<0.0001) in group I as compared to group II [Table 2]. Dandona P et al reported 33% reduction in CRP levels on combination therapy with metformin and gliclazide for 4 months in poorly controlled type 2 DM patients which is more as compared to our findings in group II. [12] In contrast to findings of present study in group I, 17.4% reduction in CRP levels was reported with use of atorvastatin for 6 months by Tan KC et al. [10]IMT: Group I showed significantly more reduction in IMT as compared to group II [Table 2]. Different studies have shown that metformin, gliclazide and atorvastatin provide similar reductions in IMT but effect of combination is not yet known. A study by Katakami N et al, significant reduced progression of 0.114 mm/ year (p=0.035) in IMT was reported with the use of metformin and gliclazide over a period of 3 year. [13] In no other study effect of metformin and gliclazide on IMT has been reported so far. In support with the findings of group I, a study by Davis M et al reported 15.3% fall in IMT after 8 weeks of treatment with atorvastatin. [14] But in another study, 7.26% reduction in IMT was reported with use of atorvastatin for 12 weeks by Mughal et al. [15] A meta-analysis demonstrated that treatment with atorvastatin significantly reduced CIMT in Chinese patients with type 2 diabetes. [16]At the start of the study, the IMT showed significant positive correlation with FBG, HbA1c, TC, LDL-C, TG and CRP in patients (p<0.01). This correlation was similar to Aftab S et al who reported positive correlation of IMT with HbA1c, TG, TC, HDL-C in type 2 diabetes mellitus patients, although did not assume statistical significance. [17] While Kanter SD et al found no association of IMT and serum TC, TG, HDL-C and LDL-C in diabetics. [18]After drug therapy for 24 weeks, group I showed significant positive correlation between change in IMT with change in CRP only (p=0.03) whereas in group II positive correlation between change in IMT seen with change in FBG and HbA1c. The correlation in change in IMT supported by Tan KC et al who reported no correlation between change in IMT to change in LDL-C or TG, but correlated significantly with the percent change in CRP. [9]Side effects: Cheng Y et al. reported similar incidence of nausea, vomiting (10-15%) with metformin and 1-2% incidence of hypoglycaemia with gliclazide. [19] These side effects were not serious enough for any of the patients to be hospitalized.
5. Conclusions
- The present study has demonstrated that 6 months of treatment using atorvastatin in combination with metformin and gliclazide was highly effective in reducing glycemic control and bringing lipid profile (TC, TG, LDL-C and HDL-C) and CRP concentrations near normal range in comparison to treatment with metformin and gliclazide alone. Intimal medial thickness was also decreased to greater extent. Atorvastatin in addition to producing favourable effect in dyslipidemia, which diabetic patients are more likely to suffer, also has pleiotropic effects. The pleiotropic effects of atorvastatin are independent of its effects on the lipid profile. The present study supported this evidence by showing no correlation between change in IMT and lipid profile. Thus combination is more useful and beneficial in diabetic patients. But to confirm its long term beneficial effect, further studies of longer duration and larger sample size are required.