Emad A.majed Isleem1, Yousef Aljeesh2
1Bachelor of Nursing from Palestine College of Nursing, Master in Public Health "Epidemiology" from Al Quds University, Palestine
2PhD in Public Health, Lecturer at the Islamic University in Gaza, Palestine
Correspondence to: Emad A.majed Isleem, Bachelor of Nursing from Palestine College of Nursing, Master in Public Health "Epidemiology" from Al Quds University, Palestine.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Abstract
This study aimed to evaluate the diabetic foot management in the governmental hospitals in Gaza Strip. The sample of the study consisted of 145 health care providers (54 physicians and 91 nurses) and 60 patients with diabetic foot (37 males and 23 females) admitted in the general governmental hospitals in Gaza Strip. For data collection, the researcher used questionnaire for health care providers, questionnaire for patients, checklist for hospitals, and focus group discussions. The results showed that 57.4% of physicians and 51.6% of nurses were familiar with diabetes mellitus to high extent, 55.6% of physicians and 49.5% of nurses were familiar with diabetic foot care to high extent. Concerning practices, the highest was in checking patients' blood sugar level (m= 4.689). There were no significant differences in treatment practices related to title, gender, hospital, experience, and qualification, but older age health care providers showed significant higher level of practice. For the patients, the overall knowledge about diabetes mellitus was above moderate (m= 2.931, 73.28%), and higher knowledge existed among male patients, those who are working, higher level of education, and higher income. For patients' compliance, the results of quantitative and qualitative data were (86.66% vs. 86.60%) for taking prescribed treatment on time, (81.32% vs. 100%) for visiting health care provider regularly, (46.66% vs. 26.6%) for soaking feet in warm water. In conclusion, the study emphasized the role of health care providers in health education, and the need to employ adequate qualified physicians and nurses to offer quality care to diabetic patients.
Keywords:
Diabetic foot, DM, DF, Evaluation, Management, Gaza Strip
Cite this paper: Emad A.majed Isleem, Yousef Aljeesh, Evaluation of Diabetic Foot Management in the Gaza Strip, International Journal of Diabetes Research, Vol. 4 No. 4, 2015, pp. 73-79. doi: 10.5923/j.diabetes.20150404.02.
1. Introduction
Diabetes mellitus is now one of the most common non-communicable diseases globally, and it affects both the young and elderly in any society. The incidence of diabetes is rising throughout the world; the figures estimated in 1995 were 135 million escalating to 151 million in 2000, and by 2025 it is anticipated that there will be 300 - 366 million diabetics all over the globe. In Palestine, it was estimated that the prevalence of DM to be 9.6% (Almoutaz, 2011). According to recent reports, the total number of new diabetic cases was 3,485 (1,793 in MOH and 1,692 in UNRWA) with incidence rate 24.2/10,000 population. One of the most serious complications of DM is the development of foot problems, including ulcerations and subsequent amputations. Foot ulcers develop in approximately l5% of people with diabetes and are a predisposing factor in approximately 85% of lower limb amputations. These figures reflected that DM and the suspected development of foot complications among diabetic patients in GS is worrying and even though the health care services have been developed since the establishment of the Palestinian National Authority, but still the number of diabetic foot complications is rising.
2. Objectives of the Study
- To evaluate the diabetic foot management in the governmental hospitals in Gaza Strip.- To identify the level of knowledge of health care providers about diabetic foot.- To examine the quality of practices of health care providers about diabetic foot.- To determine the differences in health care providers' practices about diabetic foot in relation to some variables (title, gender, hospital, years of experience, and qualification).- To identify the level of patients' knowledge about diabetes and diabetic foot care.
3. Methodology
Study design: Descriptive, cross-sectional, analytical design. The researcher used mixed method of quantitative and qualitative method.Study population and sample: The population of the study consisted of all the physicians, surgeons, and nurses who are working in surgical departments in all the governmental hospitals which offer treatment to diabetic foot patients in GS, their total number was 158 (60 physicians and 98 nurses), and 145 (54 physicians and 91 nurses) agreed to participate in the study with response rate 91.7%. In addition, the sample of the patients consisted of all diabetic patients who have foot complications and admitted to any of these hospitals during data collection period (purposive accidental sample). Their total number was 60 patients (37 males and 23 females). Setting of the study: This study was carried out in 6 general governmental hospitals which take care of patients with diabetic foot complications (Al-Najar, Nasser, EGH, Shohada al-Aqsa, Kamal Odwan, and Al-Shifa hospital).Instruments of the study: Questionnaire for health care providers and questionnaire for the patients, and checklist prepared by the researcher, and focus group discussions with three groups of patients.To check the appropriateness of the questions, the clarity of wording, the researcher distributed the questionnaire to a group of 8 expertise in public health, and a pilot study was carried out on a sample of 40 health care providers, and 40 patients selected randomly from all the hospitals. The participants in the pilot study were included in the actual sample. Internal consistency indicated good correlation of the items of the questionnaires, split half method and Cronbache alpha coefficient for health care providers questionnaire were (R = 0.608 and 0.779 respectively), and for the patients questionnaire were (R = 0.775 and 0.865 respectively). Statistical tests used for data analysis included frequency, percentage, mean, (t) test, One way ANOVA and post hoc Scheffe test. Also qualitative data were categorized and interpreted to integrate quantitative data.
4. Results
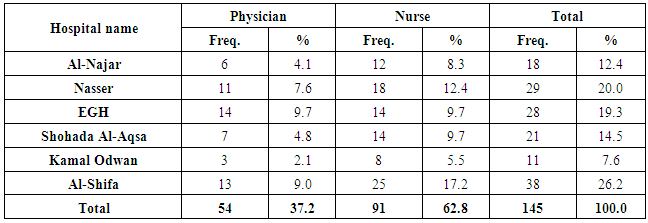
The results showed that 57.4% of physicians were familiar with DM to high extent, and 29.6% were familiar to moderate extent, while 51.6% of nurses were familiar with DM to high extent, and 39.6% were familiar to moderate extent. In addition, 55.6% of physicians were familiar with DF care to high extent, and 31.5% were familiar to moderate extent, while 49.5% of nurses were familiar with DF care to high extent, and 42.9% were familiar to moderate extent. Furthermore, 66.7% of physicians know to high extent that controlling blood sugar affects diabetic foot, and 24.1% know that to moderate extent, while 68.1% of nurses know to high extent that controlling blood sugar affects diabetic foot, and 25.3% know that to moderate extent. The results also showed that the vast majority of study participants (90.7% of physicians and 94.5% of nurses) had learned about diabetic foot during their study in the college, but only 37% of physicians and 26.4% of nurses received training about diabetic foot care during their work.Concerning practices the results showed that the highest scores were in the statement "I check the diabetic foot patients' blood sugar level every day and as needed" with mean score 4.689 and weighted percentage 93.78, followed by the statement "I give hypoglycemic drugs (insulin – metformin …) according to blood sugar level" with mean score 4.627 and weighted percentage 92.54, and "I perform dressing on patients' foot every day and as needed" with mean score 4.579 and weighted percentage 91.58. There were statistically insignificant differences at ≥ 0.05 in practices of health care providers about diabetic foot related to title (P = 0.182), gender (P = 0.376), hospital (P = 0.162), and experience (P = 0.099).Table (1). Distribution of health care providers by title and hospital name
 |
| |
|
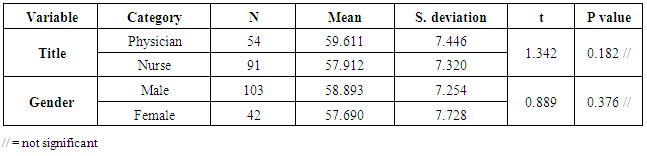
Differences in practices of health care providers about diabetic foot related to selected variablesTable (2) showed that there were statistically insignificant differences at ≥ 0.05 in practices of health care providers about diabetic foot related to title (t = 1.342, P = 0.182) and gender (t = 0.889, P = 0.376), which means that both physicians and nurses, males and females take care of diabetic foot without differences in health practices.Table (2). Differences in practices of health care providers about diabetic foot related to title and gender
 |
| |
|
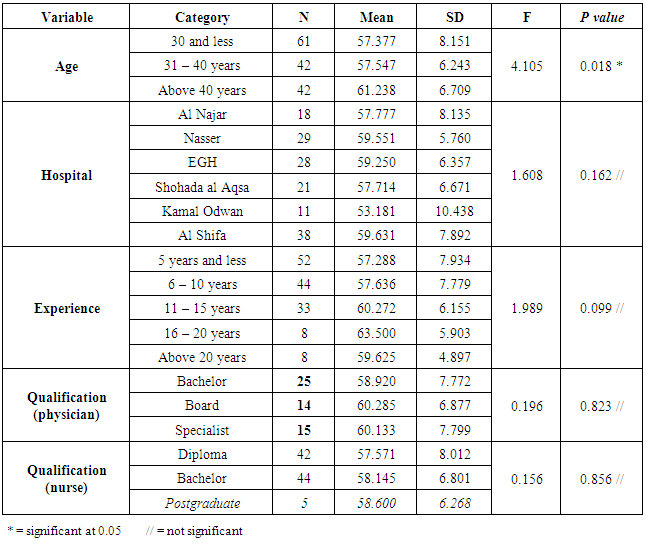
Table (3) showed that there were statistically insignificant differences at ≥ 0.05 in practices of health care providers about diabetic foot related to hospital (F = 1.608, P = 0.162), years of experience (F = 1.989, P = 0.099), qualification of physicians (F = 0.196, P = 0.823), and qualification of nurse (F = 0.156, P = 0.856). These results indicated that physicians and nurses from different hospitals, different experiences, and different qualifications do not have differences in their health practices. The results also showed that there were statistically significant differences at ≥ 0.05 in practices about diabetic foot related to age of health care providers (F = 4.105, P = 0.018), and to find the direction of these differences, Post Hoc Scheffe test was performed and it showed that the differences were in favor of health care providers who were above 40 years of age compared to those who were 30 years and less. This result revealed that older health care providers showed higher quality of practices about diabetic foot compared to younger health care providers, which could be attributed to the long years of working with diabetic patients and seeing many patients, and gaining more knowledge and skills in managing such patients.Table (3). Differences in practices of health care providers about diabetic foot related to hospital, experience, and qualification
 |
| |
|
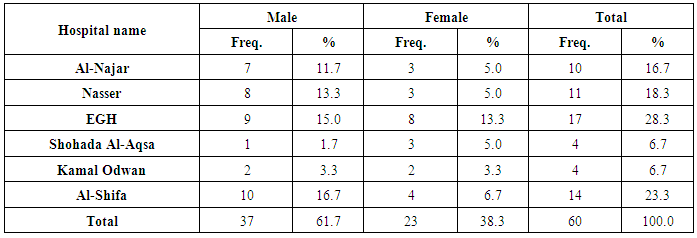
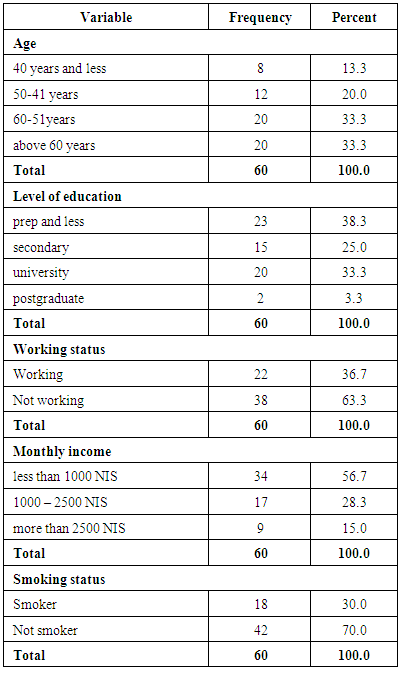
Knowledge of patients about DMThe highest score was in the statement "I know that Diabetes mellitus is a chronic disease" with mean score 3.650 and weighted percentage 91.25, followed by the statement "I know that Diabetes (as a disease) can be controlled" with mean score 3.333 and weighted percentage 83.32, and "I know that controlling blood sugar is important to avoid diabetic foot" with mean score 3.150 and weighted percentage 78.75. There were statistically significant differences at α ≥ 0.05 in knowledge of patients about diabetes related to gender (P = 0.043), and these differences were in favor of male patients, also differences were significant in relation to working status (P = 0.002), and these differences were in favor of those who were working. The results also showed that there were statistically insignificant differences in knowledge about diabetes in relation to smoking status (P = 0.388) and type of diabetes (P = 0.264), age (P = 0.145), marital status (P = 0.475), duration of diabetes (P = 0.410), type of treatment (P = 0.838). In addition, there were statistically significant differences at α ≥ 0.05 in compliance of patients to diabetic foot care related to type of diabetes (P = 0.038), and these differences were in favor of patients with type 2 diabetes, but differences were insignificant in relation to gender (P = 0.329), working status (P = 0.306), and smoking status (P = 0.826), age (P = 0.499), level of education (P = 0.269), marital status (P = 0.184), income (P = 0.100), duration of diabetes (P = 0.302), and type of treatment (P = 0.442).Table 4. Distribution of patients by gender and hospital name
 |
| |
|
Table 5. Distribution of patients by demographic variables
 |
| |
|
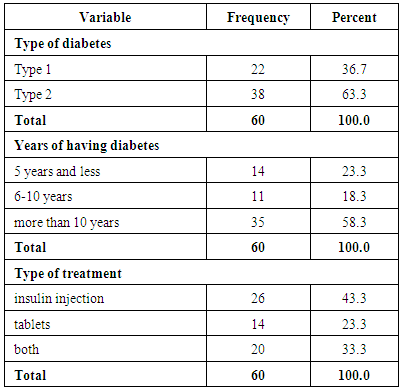
Table 6. Distribution of patients by Diabetes mellitus
 |
| |
|
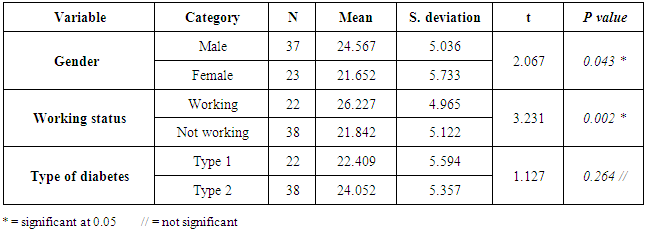
Differences in patients' knowledge related to selected variablesTable (7) showed that there were statistically significant differences at α ≥ 0.05 in knowledge of patients about diabetes related to gender (t = 2.067, P = 0.043), and these differences were in favor of male patients, also differences were significant in relation to working status (t = 3.231, P = 0.002), and these differences were in favor of those who were working, and type of diabetes (t = 1.127, P = 0.264).Table 7. Differences in knowledge of patients about diabetic foot care related to gender, work, and type of diabetes
 |
| |
|
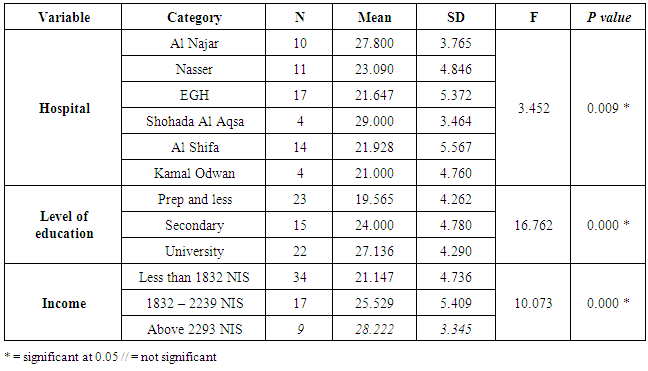
Table (8) showed that there were statistically significant differences at α ≥ 0.05 in knowledge of patients about diabetes related to hospital (F = 3.452, P = 0.009), but the post hoc Scheffe test showed that these differences were not statistically significant. Also, there were statistically significant differences at α ≥ 0.05 in knowledge of patients about diabetes related to level of education (F = 11.002, P = 0.000), and the post hoc Scheffe test showed that these differences were in favor of patients who have secondary and university education compared to those who have lower level of education (prep school and less). In addition, the results showed that there were statistically significant differences at α ≥ 0.05 in knowledge of patients about diabetes related to monthly income (F = 10.073, P = 0.000), and the post hoc Scheffe test showed that these differences were in favor of patients who have high and middle income compared to those who have low income.Table 8. Differences in knowledge of patients about diabetic foot care related to hospital, level of education, and income
 |
| |
|
The results also showed that there were statistically significant differences at α ≥ 0.05 in compliance of patients to diabetic foot care related to type of diabetes (t = 2.127, P = 0.038), and these differences were in favor of patients with type 2 diabetes, but differences were insignificant in relation to gender (t = 984, P = 0.329), and working status (t = 1.034, P = 0.306). Also, there were statistically insignificant differences at α ≥ 0.05 in compliance of patients to diabetic foot care related to hospital (F = 2.010, P = 0.092), age (F = 0.800, P = 0.499), level of education (F = 1.346, P = 0.269), marital status (F = 1.744, P = 0.184), monthly income (F = 2.397, P = 0.100), duration of diabetes (F = 1.222, P = 0.302), and type of treatment (F = 0.828, P = 0.442).Focus Groups ResultsThe researcher conducted three focus groups, one at Al Shifa hospital, one at EGH, and one at Nasser hospital. Each group consisted of five diabetic patients who were admitted in the hospital. Focus group interview questions concentrated on three major themes:a. Compliance to medication and dietary regime.b. Behaviors that contribute to improving blood circulation in lower limbc. Seeking health education for better understanding of the disease conditions.The first theme asked the patients to talk about their diet and food consumption and medication. The results showed that 46.6% of patients comply to dietary regime always, 26.6% followed dietary regime sometimes, while 26.6% do not follow dietary regime. One patient said "I eat everything as the other family members, I don't follow any regime" another patient said "I had diabetes since six years, one day I was watching TV, there was a program about DM, in the program they mentioned that dietary regime will control blood sugar, so, I stopped medication and followed diet with low sugar content, but did not check my blood sugar for a long time. One day, I had chest infection, the doctor asked for blood sugar and it was very high, then I started to take my medication again". Concerning medication, the results showed that 86.6% of patients take their medication on time as prescribed, while 13.2% sometimes follow medication times. One patient said "I take injection two times a day, morning to inject myself. Now I take the injections on my own, and I check my blood sugar every two weeks in the clinic". The second theme asked the patients about behavioral measures that contribute to improving blood circulation in lower limbs to avoid the development of DFU. The results showed that only 26.6% of patients soak their feet in warm water always, 20.0% sometimes soak their feet, and 53.3% don't soak their feet in warm water. One patient said "I wash my feet for praying, but I don't soak my feet in warm water, and no one told me about soaking feet in warm water". In addition, only 20.0% of patients inspect their feet and toes always for bruises or ulcers, 73.3% inspect their feet sometimes, and 6.6% don't inspect their feet. Furthermore, 86.6% of patients always dry well between toes, 6.6% sometimes dry between their toes, and 6.6% don't dry. All the patients 100% said that they have their nails cut properly, they get help from their wives and sons in cutting their nails. many patients said we soak feet in warm water, but not every day, dry between toes. Other patients said "my wife help me in cutting my nails and inspecting my feet, and others get help from their daughter or son" another patient said "I soak my feet in sea water". Only 33.3% always wear well-fitted shoes, 6.6% wear proper shoes sometimes, and 60% don't wear well-fitted shoes. One patient said "I wear sandals most of the time, no one told me about how to buy proper shoes", in contrast another patient said "I buy well-fitted leather shoes that are fitted well in my feet, also the shoes should not be rigid". Wearing proper shoes that are fitted well in feet and manufactured from flexible material is important to avoid pressure and diminish blood supply in the feet, which would lead to ulceration in the feet. All the patients said that they visit the doctor in the clinic on regular bases, but they mentioned that they go to the clinic to get their monthly medication. Only 33.3% of patients walk or exercise every day, 46.6% walk sometimes, and 20% of patients don't walk nor exercise.The third theme asked the patients about health education and the results showed that only 20% seek health education always, 46.6% attend health education sessions sometimes, and 33.3% don't seek or attend health education programs. To avoid complications, one patient said "the diabetic patient needs to eat a balanced diet, walk daily, deal with diabetes as a friend not enemy, soak feet in warm water, and inspect the feet for lacerations or bruising".
5. Discussion
The management of diabetes poses a challenge to the health care providers as well as to the patients themselves. Since diabetes is a chronic disease, most diabetic patients need to continue their treatment regime for the rest of their lives, so, competent self-care is required, which could be developed from a thorough understanding of the disease process and the management challenges by the patients. Lack of knowledge and malpractice from the side of health care providers and patients has been one of the major obstacles in the management of diabetes.The study results showed that health care providers were familiar with diabetes and had good knowledge about diabetes and diabetic care. Similar results were reported in a study conducted by Babelgaith et al., (2013) which showed that the majority of participants had a good general knowledge of diabetes and its management. In addition, the clinical audit carried out by UNRWA (2012) showed that knowledge, attitudes and practice of medical officers revealed good knowledge of diabetes and diabetes care, and proper adherence to technical instructions. In contrary, a study conducted in Nigeria found that the knowledge of diabetes in patient care was fair and acceptable among specialists and resident doctors, while nurses had very low knowledge of diabetes (Olamoyegun et al., 2013), another study conducted in Pakistan found that the overall mean knowledge about diabetes among all the participants was 50%, and that there were no statistical differences in terms of knowledge between different specialties (Ahmed et al., 2012).In addition, the practices of health care providers about diabetic foot were of good quality. A study conducted in Yemen found that the majority of health care providers monitor the symptoms of complications, monitor blood glucose level every visit, the study also concluded that although HbA1C is very important in monitoring the control of diabetes and a good indicator of the patient's compliance with the treatment, it is not commonly monitored in Yemen, probably owing to the unavailability of the test or due to its high cost (Babelgaith et al., 2013), another study presented in a symposium in Cape town, South Africa, Nov. 15, 2014, concluded that capacities, knowledge, and practice of type 2 diabetes care were poor among health care providers (Mafuta, 2014). Furthermore, a study carried out by the Cleveland Clinic in Ohio (2014) found that the overall level of knowledge of diabetes management was lower than expected, also, there were no differences in knowledge based on education level or years of experience.Regarding the patients, the results showed that they have a moderate fragmented knowledge about the disease and even their rating was low in the compliance to treatment of diabetic foot, which was evidence in low engagement in exercise and sport activities, poor seeking of health education from the treating health care providers or from media and articles. Previous studies showed variations in results; a study conducted by Desalu, (2011) found that 78.4% of patients had poor information about foot care, and Elbagir, et al., (1996) reported that 90% of screened diabetic patients had poor knowledge about their disease and 96.3% had poor awareness about its control. Another study conducted in Nigeria found that only 30.1% of patients had good knowledge about diabetes, 68.8% were unaware of the first thing to do when they found redness/bleeding between their toes and 61.4% were unaware of the importance of inspecting the inside of the footwear for objects (Desalu et al., 2011). Concerning compliance, previous studies showed also low level of compliance and poor practice among diabetic patients; a study conducted in northern of West Bank showed that 42.1% of patients had good compliance and 42.7% of the study participants were considered non-adherent to treatment (Sweileh et al., 2014), lower results were obtained by Desalu et al., (2011) as only 10.2 % of patients had good practice of diabetic foot care, 78.4% of patients with poor practice had poor knowledge of foot care, and 88.6% failing to get appropriate size footwear. Another study found that only 14% of respondents had good practices for foot care (Hasnain and Sheikh, 2009). In Saudi Arabia a study conducted by Khan et al., (2012) showed that the overall prevalence of therapeutic non-compliance of the participants was 67.9%, and in Egypt, the overall rate of adherence among the patients was found to be suboptimal and non-acceptable (Shams and Barakat, 2010).In conclusion, the results emphasized the role of health care providers in health education to increase the level of knowledge and awareness of patients about diabetic foot care to minimize the unwanted complications that could affect the quality of life for the diabetic patients. Health education plays a major role in controlling blood sugar levels and avoiding subsequent complications. From the focus groups interviews it was obvious that there was inadequate health education, and efforts should be directed towards emphasizing health education in health facilities and encourage patients to increase their participation in health education programs to increase their understanding and awareness about the seriousness of the DM with its anticipated complications.
References
| [1] | Ahmed, A., Abdul Jabbar, Zuberi, L., Islam, M., & Shamim, K. (2012). Diabetes related knowledge among residents and nurses: a multicenter study in Karachi, Pakistan. BMC Endocrine Disorders, 12,18. (www.biomedcentral.com) |
| [2] | Almoutaz, A., Al-Sharief, E., & Al-Sharief, A. (2011). The diabetic foot in the Arab World. The Journal of Diabetic Foot Complications, 3(3), 55-61. |
| [3] | Babelgaith, S., Baidi, M., & Alfadly, S. (2013). Assessment of the knowledge and practice of health care professionals towards diabetes care in Mukalla, Yemen. International Journal of Pharmacy Teaching & Practices, 4(4), 826-831. |
| [4] | Desalu, OO., Salawu, FK., Jimoh, AK., Adekoya, AO., Busari, OA., & Olokoba, AB. (2011). Diabetic foot care: self-reported knowledge and practice among patients attending three tertiary hospital in Nigeria. Ghana Medical Journal, 45(2), 60-65. |
| [5] | Elbagir, N., Eltom, A., Elmahdi, M., Kadam, M., & Berne, C. (1996). A population based study of the prevalence diabetes and impaired glucose tolerance in adults in northern Sudan. Diabetes Care ,19, 1126-1128. |
| [6] | Hasnain, S. & Sheikh, NH. (2009). Knowledge and practices regarding foot care in diabetic patients visiting diabetic clinic in Jinnah Hospital, Lahore. J Pak Med Assoc, 59(10), 687-690. |
| [7] | Mafuta, E., Kapongo, R., Lulebo, A., Mutombo, P., Claude, J., & Bieleli, I. (2014). Assessment of health service delivery capacities, health providers’ knowledge and practices related to type 2 diabetes care in Kinshasa primary healthcare network facilities, Democratic Republic of the Congo. Third Global Symposium on Health Systems Research, At Cape town, South Africa, Nov. 15, 2014. |
| [8] | Olamoyegun, MA., Iwuala, SO., Akinlade, OM., Olamoyegun, KD., & Kolawole, K. (2013). Assessment of diabetes-related knowledge among health care providers in a tertiary health institution in Nigeria. Nigerian Endocrine Practice, 7(1). (http://www.ajol.info/index.php). |
| [9] | Sweileh, W., Zyoud, SH., Abu Nab'a, RJ., Deleg, MI., Enaia, MI., Nassar, SM., & Al-Jabi, SW. (2014). Influence of patients' disease knowledge and beliefs about medicines on medication adherence: findings from a cross-sectional survey among patients with type 2 diabetes mellitus in Palestine. BMC Public Health, 14:94.(www.ncbi.nlm.nih.gov/pubmed). |
| [10] | Shams, M. & Barakat, E. (2010). Measuring the rate of therapeutic adherence among outpatients with type 3 DM in Egypt. Saudi Pharm Journal, 18(4), 225-232. |
| [11] | The Cleveland Clinic – Ohio, (2014). Measuring nurses’ knowledge of diabetes management. CHEST Physician, 31(9), 41. |
| [12] | UNRWA, (2012). Clinical audit of diabetes care among Palestine refugees. World Diabetes foundation. |
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML