-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Diabetes Research
p-ISSN: 2163-1638 e-ISSN: 2163-1646
2014; 3(3): 41-48
doi:10.5923/j.diabetes.20140303.03
Effect of Twelve Weeks Supervised Aerobic Exercise on Ulcer Healing and Changes in Selected Biochemical Profiles of Diabetic Foot Ulcer Subjects
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMaduabuchi Joseph Nwankwo1, Goddy Chuba Okoye2, Egwuonwu Afamefuna Victor1, Ezeukwu Antoninus Obinna2
1Department of Medical Rehabilitation, Nnamdi Azikiwe University, Nnewi Campus
2Department of Medical Rehabilitation, University of Nigeria Enugu Campus
Correspondence to: Egwuonwu Afamefuna Victor, Department of Medical Rehabilitation, Nnamdi Azikiwe University, Nnewi Campus.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Background and Objectives: Diabetes and diabetic complications represent a significant burden for the patients, their families and the society at large. This study evaluated the effect of aerobic exercise on diabetic ulcer healing and changes in selected biochemical profiles of individuals with diabetic foot ulcer.Methododology: The study employed a pretest-posttest randomized control trial design. Sixty one (61) subjects including 31 males and 30 females with diabetic foot ulcers were recruited to the study and were randomized using the pitcher bowl method to either receive the aerobic exercise with bicycle ergometer (Group One) or not (Group Two) but placed on their routine treatment alone. The study was carried out at Nnamdi Azikiwe University Teaching Hospital, Nnewi. Subjects reported to the clinic 3times a week and both groups were assessed for baseline data which included BMI, fasting plasma glucose, total cholesterol, and wound size area measurements. The follow up evaluations were done on a 2 weekly basis for the twelve weeks period. Initial aerobic exercise intensity was based on 60% of maximum heart rate (HR) achieved on a stress test. Each subject was progressed to 85% of the value for the twelve weeks. Results: The group one subjects had a significant decrease in wound size area after the intervention with p value = 0.001** (26.459.46 and 17.77.23) baseline for group one and two after intervention (1.97 4.17 and 7.93 4.08), the duration of diabetes were significantly correlated with percentage wound size reduction, (p = 0.37** and 0.037) after 4th week intervention. The study showed that fasting plasma glucose was significantly different but the total cholesterol level was not different in the experimental group compared to the non experimental group (p values = 0.03** and 0.56) post intervention.Conclusions: The study suggests that supervised aerobic exercise program should be an essential component of the treatment plan for patients with diabetic foot ulcer. Future studies should consider randomized control trial with a longitudinal design, incorporating sophisticated wound assessment tool, to rule out inaccurate measurements.
Keywords: Diabetes, Diabetic foot ulcer, Wound size area, Fasting plasma glucose, Total cholesterol level, Wound size reduction
Cite this paper: Maduabuchi Joseph Nwankwo, Goddy Chuba Okoye, Egwuonwu Afamefuna Victor, Ezeukwu Antoninus Obinna, Effect of Twelve Weeks Supervised Aerobic Exercise on Ulcer Healing and Changes in Selected Biochemical Profiles of Diabetic Foot Ulcer Subjects, International Journal of Diabetes Research, Vol. 3 No. 3, 2014, pp. 41-48. doi: 10.5923/j.diabetes.20140303.03.
Article Outline
1. Introduction
- Background of StudyDiabetes mellitus is a group of metabolic disorders characterized by elevated levels of glucose in the blood (hyperglycemia) resulting from defects in insulin secretion, insulin action or both [1].Diabetes results in chronic hyperglycemia and hyperlipidemia that ultimately induces diverse multiple system pathologies; increasing the risk for atherosclerosis, coronary heart disease, stroke, myocardial infarction, renal disease and periodontitis. It is the third leading cause of death by disease in Nigeria and the sixth in the world generally and affects about 5.2% of its population [2]. People with diabetes have a 12–25% lifetime risk of developing a foot ulcer [3].An estimated 14.6 million persons are currently diagnosed with foot ulcers. In 2005 Nigeria had 19.4 million diabetes compared to 16 million in China which comes second. According to WHO by 2025, Nigeria will have 57.2 million diabetic while China will have 37.6 million diabetic patients. The economic burden that this large number of diabetics will place on our health care system even if a fraction were to develop complications is too enormous [4].Diabetic foot ulcers result from the simultaneous action of multiple contributing causes. The major underlying causes are noted to be peripheral neuropathy and ischemia from peripheral vascular disease [5].Diabetic foot ulcers is one of the most common and devastating complication of diabetes mellitus, the macro vascular and micro vascular changes and the neuropathy all contribute to changes in the lower extremity called the diabetic foot ulcer. Macro vascular and micro vascular changes produce tissue ischemia and skin changes that can cause ulcerations and infections and prevent healing. The inter relationship of all these factors; contribute to formation of lesions which results to gangrene and ultimately amputation [6]. More than 60% of diabetic foot ulcers are the result of underlying neuropathy [7]. The development of neuropathy in affected patients has been shown to be a result of hyperglycemia-induced metabolic abnormalities. One of the more commonly described mechanisms of action is the polyol pathway. In the development of neuropathy, the hyperglycemic state leads to an increase in action of the enzymes aldose reductase and sorbitol dehydrogenase. This results in the conversion of intracellular glucose to sorbitol and fructose [8].The accumulation of these sugar products results in a decrease in the synthesis of nerve cell myoinositol, required for normal neuron conduction. Additionally, the chemical conversion of glucose results in a depletion of nicotinamide adenine dinucleotide phosphate stores, which are necessary for the detoxification of reactive oxygen species and for the synthesis of the vasodilator nitric oxide. There is a resultant increase in oxidative stress on the nerve cell and an increase in vasoconstriction leading to ischemia, which will promote nerve cell injury and death. Hyperglycemia and oxidative stress also contribute to the abnormal glycation of nerve cell proteins and the inappropriate activation of protein kinase C, resulting in further nerve dysfunction and ischemia. Neuropathy in diabetic patients is manifested in the motor, autonomic, and sensory components of the nervous system [8].Damage to the innervations of the intrinsic foot muscles leads to an imbalance between flexion and extension of the affected foot. This produces anatomic foot deformities that create abnormal bony prominences and pressure points, which gradually cause skin breakdown and ulceration. Autonomic neuropathy leads to a diminution in sweat and oil gland functionality. As a result, the foot loses its natural ability to moisturize the overlying skin and becomes dry and increasingly susceptible to tears and the subsequent development of infection. The loss of sensation as a part of peripheral neuropathy exacerbates the development of ulcerations. As trauma occurs at the affected site, patients are often unable to detect the insult to their lower extremities. As a result, many wounds go unnoticed and progressively get worse as the affected area is continuously subjected to repetitive pressure and shear forces from ambulation and weight bearing [7].Foot problems constitute the primary cause of hospitalization of people with diabetes. Above 15% develops foot or leg ulcer. Amputation is common in diabetics and diabetic amputees that have had one amputation or more have 28% to 51% chance of needing a centralized one within five years [4].In individuals with diabetes, circulating endothelial progenitor cells are exposed to abnormal levels of plasma glucose. It has been demonstrated that patients with diabetes not only have fewer endothelial progenitor cells than healthy individuals, but the function of the endothelial progenitor cells that they do have is impaired leading to poor healing of diabetic foot ulcer [8]. Diabetic complications such as diabetic foot ulcer is as a result of peripheral neuropathy and /or large vessel disease due to hyperglycemic state of the individual patient, which overtime results in the irreversible covalent modification of structural protein and lipids (glycosylation) that compromises the extracellular matrix and connective tissues as well as vascular tissues [9]. These structural changes results in impaired capillary function and the release of oxidizing agents triggering systemic inflammatory process. Diabetic foot ulcer is associated with reduced nerve perfusion which is an important factor in the etiology of diabetic neuropathy [10].Despite attentive management of diabetic foot ulcers with multiple modalities such as surgical debridement, relief of pressure, and other standard measures, many diabetic foot ulcers persist as chronic, non-healing wounds that eventually leads to limb amputation [11]. However, high quality evidence on the effect of aerobic exercise on changes in biochemical profiles of diabetic subjects and wound healing were lacking. Previous pilot study by Donna [12], evaluated the effects of a four weeks ankle exercise as a treatment and prevention of diabetic foot ulcers in diabetics. In the study, the impact of exercise and no exercise were compared on wound healing using quasi experimental design by assessing the wound swab before and after 3months although the studies noted an improvement in results of wound swab analysis of diabetics on exercise compared to no exercise group it was not significant, the limitation of that study were short intervention period and inability of the researcher to assess changes in biochemical profiles of diabetic subjects and wound healing. Few studies have jointly estimated changes in biochemical profiles of diabetic subjects and the rate of wound healing in diabetic individual on exercise intervention.However, shortfalls in these previous studies targeted at assessing the effect of aerobic exercise as a means of promoting wound healing by possibly improving oxygen supply to the lower limbs of diabetics with foot ulcers and consequent changes in biochemical profiles of these subjects, necessitated the present study. This study investigated the effect of aerobic exercises on changes in biochemical profiles of diabetic subjects and rate of ulcer healing on patients with diabetic foot ulcers.
2. Methods and Materials
- SubjectsThe subjects were known type 1 or type 2 diabetic mellitus patient. Informed consent were obtained from the participants prior to the study and medical history which include basal heart rate, blood pressure, date of diabetes mellitus diagnosis, medication and co morbidities were collected. The pre-exercise stress test was arranged to ensure clearance for participation. All subjects had normal cognition as determined by a Folstein mini-mental status examination score of >23. The study was a twelve weeks supervised aerobic exercise program, that involved sixty one accessible adults with mean age of 69±4.79, that participated in the study, they were randomly assigned into two groups using the pitcher bowl method, group one (experimental group) are 31 diabetics with foot ulcers (16 males and 15 females), group two (non-experimental group) are diabetic with foot ulcers (15 males and 15 females) attending the diabetic clinic of Nnamdi Azikiwe University Teaching Hospital, Nnewi.Inclusion CriteriaThey were recruited for the study based on meeting certain inclusion criteria which is as follows: eligible subjects were sedentary for at least 6 months prior to the study. All the subjects had diabetic foot ulcers as a result of type 1 or 2 with at least 1cm2 (greatest length x greatest width) and at least foot ulcer of 30 days duration. The protocol was designed according to the fundamental treatment principal of the expert panel to the 2004 American Diabetic Association [13] consensus development conference on diabetic foot wound care. Exclusion CriteriaSubjects with congestive heart failure, uncontrollable cardiac arrhythmias, severe valvular heart diseases, individuals with uncontrolled BP (systolic BP>165/mmHg), extreme claustrophobia, Hematological disease that affects mobility, impaired knee flexion of <1900 and severe illness that precluded them from exercising, were excluded from the study.Study DesignThe study was a pretest-posttest randomized control trial design without single or double blinding of the participants. Sampling TechniqueThe subjects were recruited using purposive non-probability sampling technique.Laboratory Test ProtocolFasting plasma glucuse test were done using the enzyme-linked immunosorbent assay which is a one step colorimetric assay to detect the level of blood (plasma) glucose. The principle is simply based on glucose oxidase enzyme oxidizing plasma glucose to form hydrogen peroxide and the hydrogen peroxide reacting with chromagen to form a coloured compound that is measured colorimetrically. It is preferred because glucose oxidase dose note react with other blood saccarides.Total cholesterol test were done using the enzyme-linked immunosorbent assay which is a one step colorimetric assay to detect the level of serum total cholesterol. The principle is simply based on an enzyme-coupled reaction that detects both free and cholesterol ester s. Cholesterol esters are hydrolyzed by cholesterol esterase into cholesterol, which is then oxidized by cholesterol oxidase to yield hydrogen peroxide and cholest-4-en 3-one (ketone). The hydrogen peroxide then reacts with the probe (Detection reagent) in a 1:1 stoichoimetry to produce stable fluorescent product. InterventionSubjects reported to the exercise clinic 3times a week, the two groups were assessed for baseline data which include height (using stadiometer), weight (using Hana bathroom scale, wound size area measurement was done for the two groups using transparent ruler to assess the wounds greatest length and width after which the wound size was calculated by multiplying the greatest length and width in centimeters. The follow up evaluations and wound size assessment were done on a 2 weekly basis for the twelve weeks study period. If a subject pre-exercise blood pressure is >165/90mmHg, he was asked to rest for 10minutes and reassessed. No exercise was permitted that day if a lower resting blood pressure was not achieved. Subjects were tested for cholesterol level and fasting blood sugar level, if the sugar level was less than 100mg/dl. They were giving a chance to take a 15gm carbohydrate snacks and reassessed 20minute later to ensure that the blood sugar level was not dropping below 100mg/dl before exercise intervention. The exercise precaution was based on recommendation by American Diabetes Association [13].Exercise ProtocolInitial aerobic exercise intensity was based on 60% of max. HR achieved on a stress test.Each subject was progressed to 85% of the value over 12weeks. All subjects were engaged in an aerobic warm-up of at least 5minutes with perceived rating in the light range of Borg’s rating of perceived exercise scale [15], following the warm up, the subjects were instructed to start with a ten minutes exercise which was increased until the exercise intensity gets to the range of target heart rate and rate of perceived exertion (RPE) to commensurate with “somewhat hard”(4 point), HR and RPE were monitored to ensure subjects were exercising at their prescribed intensity throughout the study. Subjects were encouraged to increase their exercise time by 5minute each two weeks until they reach 50minute at the ninth week, which was maintained until the end of the 12weeks program [15].Each of the subjects were exercising under supervision throughout the study and rode on a bicycle ergo meter with foot interaction kept constant with a standard gym pedal and a specialized off-loading insole padding to relieve pressure on the ulcer. This study was conducted between 7th January to 6th May 2013. While the group two subjects were placed on the normal wound dressing, diet control, counselling and medication without any form of exercise.Instrumentation1. Stop watch model Heuer tracmate brand was used for time measurement2. Transparent ruler made in China was used to measure the greatest length and width of the wound3. Stadiometer model Butterfly brand made in China was used to measure subject’s height 4. Bicycle Ergometer model (PRO-ACTING Model) was used for non-weight bearing aerobic exercise5. Bathroom weighing scale Hana brand made in China was used to measure subject’s weight 6. Borg’s rating scale of perceived exertion was used to monitor subject’s level perceived exertion during exercise. It is an open ended scale from 0 (Resting) to 10 (Very very hard). The scale is reliable enough to account for differences in a subject’s personality and emotions and has a reliability coefficient of 90% between perception of exertion and physical activity load [16].7. Folstein mini mental scale was used to assess subject’s cognition8. ACU CHEK, ROCHE for measurement of fasting plasma glucose9. CholesTrak test kits (ACCUTECH) for measurement of total cholesterol profileEthical approvalThe ethical approval was sought and obtained from the Ethical Review Committee of the Nnamdi Azikiwe University Teaching Hospital Nnewi, before commencement of the study.Data AnalysisThe data obtained were analyzed using descriptive statistics of mean and standard deviation for all the variables and presented using tables and bar chart, inferential statistics of dependent and independent t-tests were used to explore differences in mean between the two groups and in the experimental group variables. Pearson’s moment correlations were used to determine relationship between the two groups and variables of the experimental group. The SPSS version 15 for windows was used for the analysis and the level of significance was set at p < 0.05.
3. Results
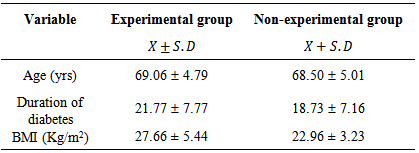
- A total of sixty one diabetic foot ulcer patients participated in this study. The subjects were randomly assigned into experimental and non-experimental groups comprising of Thirty One (16 males and 15 females) and Thirty (15males and 15 females) respectively. The patients were actively involved throughout the twelve weeks study without any of them absconding or dying before the end of the study.Socio demographic characteristics of subjectThe subjects had a mean age of 69.06±4.79 (experimental group) and 68.50±5.01 (non-experimental group). The duration of diabetes were 21.77 ± 7.77 for experimental and 18.73 ± 7.16 for non-experimental group, while their body mass indices (BMI) were 27.66 ± 5.44 and 22.96 ± 3.23(Kg/m2) for group one and two respectively. Table 1
|
|
|
|
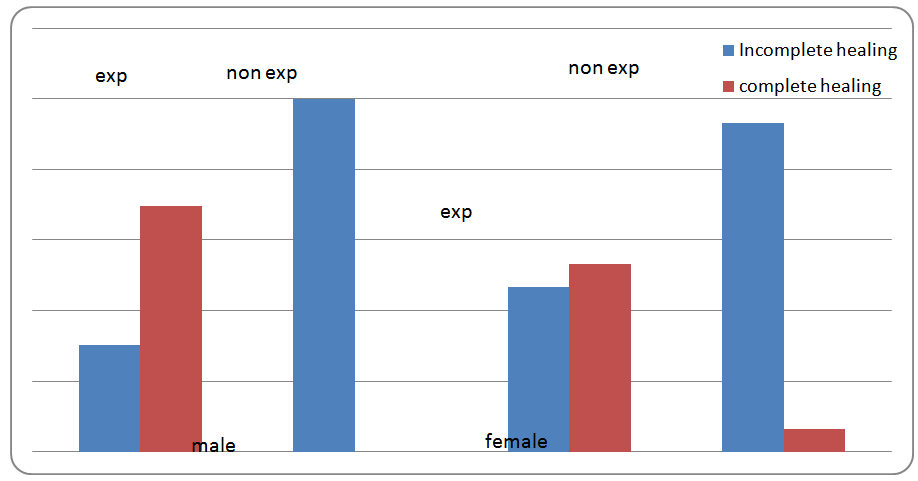 | Figure 1. The Chart showing percentage healing among the gender in both groups |
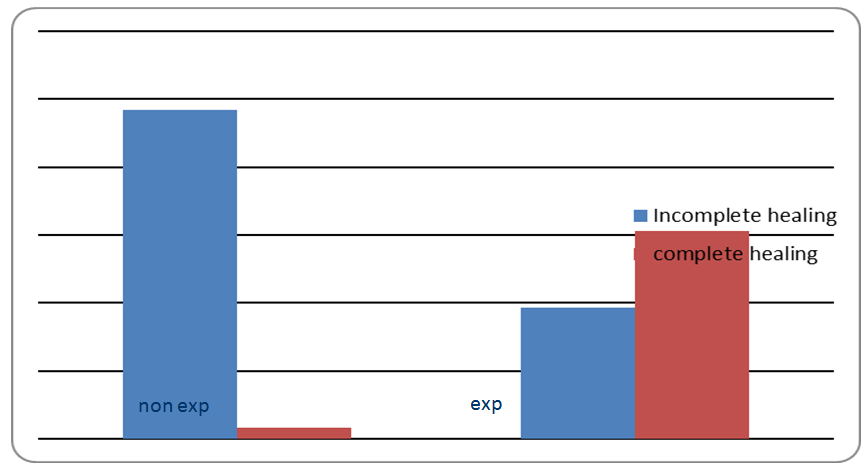 | Figure 2. The Chart showing percentage healing comparing experimental and non-experimental groups |
4. Discussion, Conclusions, Recommendations and Implication for Studies
4.1. Discussion
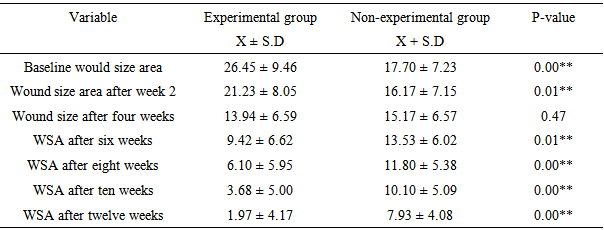
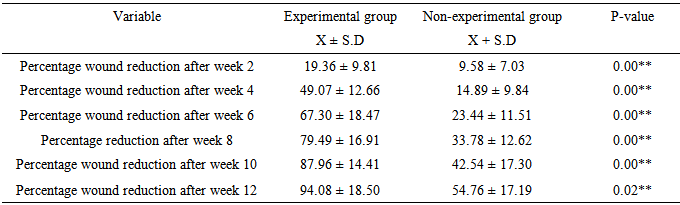
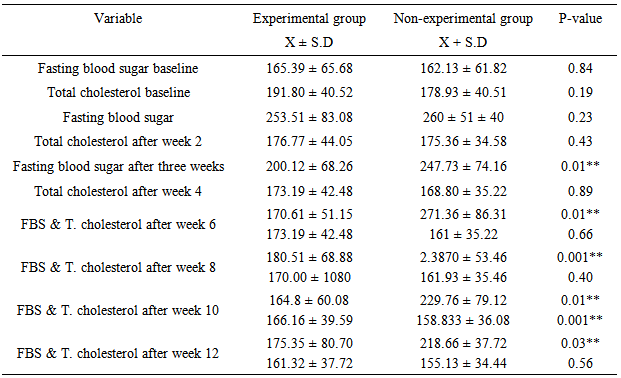
- The BMI of the experimental group were slightly higher than the non-experimental. This may have explained the higher baseline wound size area observed in the experimental group (26.45±9.46) compared to that of the non-experimental groups (16.27±1.15). Since BMI is a risk factor for development and worsening of diabetic foot ulcer as reported by Hansen et al, [18]; in their proposed guideline for exercise prescription for patients with type 2 diabetes.It was also observed in this study that the duration of diabetes was higher among the experimental group compared to non-experimental group (21.77±7.77 and 18.73±16), this may have contributed to the higher baseline wound size area shown by the experimental group.There were greater significant wound healing in the experimental group compared to the non-experimental group at the end of the twelve weeks intervention, this was reflected in the wound size area of 1.97±4.17 for experimental group compared to 7.93±4.08 for non-experimental with p value of 0.001** from the independent t-test. The results were similar to the findings of Yardley et al, [19] that conducted a study on the effects of performing resistance and aerobic exercise on glycemic control in patients with diabetes which reported a significant wound healing in foot ulcers.The result of the present study showed that after four weeks of exercise intervention, the wound size areas significantly correlated with percentage wound size reduction with r and p value of (0.719** and 0.001) This shows that with adequate treatment of diabetic foot ulcer, there is a marginal wound size reduction taking place as observed in the non-experimental group but with aerobic exercise intervention the wound size reduction rate doubles as in the experimental group. Meanwhile, the percentage wound size reductions were higher after the fourth week of aerobic exercise intervention (49.07 ± 12.66) which is similar to the findings of Donna, [12]. Therefore with exercise intervention, about 66.76% (male) and 53.33% (female) had 100% wound size reduction at the end of the 12 week intervention. While in the non-experimental group, none of the male subjects had complete healing and about 6.67% female had complete wound healing at the end of 12 week intervention. In summary 61.29% of the experimental group subjects had complete wound healing within 12 week and 3.33% of the non-experimental subjects had complete wound healing after 12 week intervention.The result of this study showed that percentage wound size reduction after twelve week intervention showed a progressive increase in the experimental group from the baseline to the end of the intervention (19.36±9.81 after two weeks and 94.08±18.50 after 12 weeks which was significantly higher than that of the non-experimental group (9.58±7.03 after two weeks and after twelve weeks 54.76±17.19) the p-value at 95% CI was 0.02**. This is in support of the fact that aerobic exercise had a significant effect on wound healing in the present study. These findings were in line with the study of Donna, [12] but contrasted with the findings of Dube et al, [17] that conducted a study on the effect of exercise on diabetic patients with neuropathic ulcer in Indonesia.It was observed that there were significant differences in fasting blood sugar in the experimental group compared to the non experimental group at week four, week 6, week 8, week 10 and week 12 but the total cholesterol level had significant difference at week 10 only which was not in agreement with other studies such as that of Donna, [12] and Dube et al, [17] that both reported progressive improvements of total cholesterol in the experimental group compared to the non-experimental group. This may be attributed to type of diet or test kit utilized in this study or that the aerobic exercise intensity was not enough to cause a significant effect on the total cholesterol level, while the fasting blood sugar may have changed as a result of the combined effect of drugs the subjects were using at the time of the study and the aerobic exercise program.
4.2. Conclusions
- Aerobic exercise was found to significantly increase wound size area and percentage wound size reduction in the experimental group at the end of the twelve weeks intervention. The wound size area at fourth week significantly correlated with the percentage wound size reduction, which also supports the fact that wound healing, was greatest at the fourth week of the aerobic exercise intervention in the experimental group. It is possible that chronic ulcer in diabetic subjects may mean slow or no healing at all. The outcome of this study suggest that diabetic patient with foot ulcers may require a minimum of about three sessions of aerobic exercise of at least sixty minutes per week for reduction in fasting plasma glucose as well as for effective healing to take place.
4.3. Recommendations
- It is recommended that aerobic exercise should be an essential component of any treatment plan for patients with diabetic foot ulcer.The aerobic exercise program should be designed by an expert and will require strict supervision to rule out possible contraindications of aerobic exercise in diabetic foot ulcer subjects.It is also recommended that moderate intensity, supervised endurance and resistance exercises be incorporated by an adequately qualified personnel for a sustained recovery to be achieved.
4.4. Limitations of the Study
- The wound assessment tool is crude and may have introduced some inconsistencies in the result of this study.The sample size is small and the absence of blinding may have limited categorical generalization of the findings of this study.
4.5. Implications for Further Studies
- A study with longitudinal design is advocated to rule out the possibility of extraneous variables such as the effect of patient’s age on the rate of ulcer healing.The use of sophisticated wound evaluation tool with well-established psychometric property is advocated in future studies to rule out the possibility of inaccurate measurements.