-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Clinical Practice
p-ISSN: 2326-1463 e-ISSN: 2326-1471
2012; 1(3): 18-20
doi:10.5923/j.cp.20120103.01
Catastrophic Obstetric Haemorrhage with Placenta Previa Accreta Complicated by Silent Scar Dehiscence : A Case Report
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRevathy Natesan Subramaniam, Siti Zawiah Omar
Department of obstetrics & Gynaecology Faculty of Medicine, University of Malaya Lembah Pantai, Petaling Jaya 50603, Kualalumpur, Malaysia
Correspondence to: Revathy Natesan Subramaniam, Department of obstetrics & Gynaecology Faculty of Medicine, University of Malaya Lembah Pantai, Petaling Jaya 50603, Kualalumpur, Malaysia.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Placenta accreta refers to abnormal placental implantation in which the placental villi is attached to the myometrium due to poorly formed or absent decidua basalis. Hence it is more common in the scarred area of the lower uterine segment that does not resist deep penetration by the trophoblast. This may result in complications in the peripartum period such as severe haemorrhage, scar dehiscence and rupture with a need for caesarean hysterectomy. The incidence of placenta accreta is rising, primarily because of the rise in caesarean delivery rates.Carefully selected cases with a prenatal ultrasound diagnosis can be managed conservatively with a multi disciplinary team which results in good outcomes. But in cases where placenta accreta occurs at the site of a previous cesarean section scar can lead to scar dehiscence or rupture long before the onset of delivery and the outcome may be disasterous. Conclusion: This report describes a patient with placenta previa with (unexpected) accreta who presented with a silent scar dehiscence and torrential haemorrhage.
Keywords: Placenta Accreta, Placenta Increta, Placenta Percreta, Scar Dehiscence ,Obstetric Haemorrhage
Cite this paper: Revathy Natesan Subramaniam, Siti Zawiah Omar, Catastrophic Obstetric Haemorrhage with Placenta Previa Accreta Complicated by Silent Scar Dehiscence : A Case Report, Clinical Practice, Vol. 1 No. 3, 2012, pp. 18-20. doi: 10.5923/j.cp.20120103.01.
1. Introduction
- Placenta accreta is associated with a high morbidity and most cases occur in concurrence with placenta previa. Placenta accreta is one of the most feared complications in obstetrics especially when undiagnosed. The incidence of placenta accreta is variable, and has been reported to be as high as one in 533 pregnancies, in a study by Wu et al.3With increasing numbers of caesarean sections being done nowadays, it is postulated that the incidence of placenta accreta would be on the rise and the risk increases with the number of previous caesarean sections7. Patients with placenta previa accreta have a significantly higher incidence of postpartum haemorrhage and are more likely to undergo emergency hysterectomy. The associated risks of injury to the urinary tract and other abdominal viscera contribute to maternal morbidity and mortality. When placenta accreta becomes further complicated by scar dehiscence as it happened in our case, (Figure 1&2 ) uterine conservation becomes difficult and hysterectomy becomes a better option due to intractable haemorrhage. The obstetrician’s main concern is to have an accurate diagnosis so they may appropriately adapt and plan the surgical procedure at the time of delivery. The development and advances of imaging and biological techniques can lead to reduced morbidity and optimize the management of Placenta accreta. The identification of biological markers such as cell-free fetal DNA or placental mRNA in maternal blood at eary pregnancy in patients with previous caesarean section and placenta previa can serve to monitor and aid in conservative treatment.12
 | Figure 1. Placenta Accreta with Scar dehiscence : intact Uterine serosa with incomplete rupture previous scar |
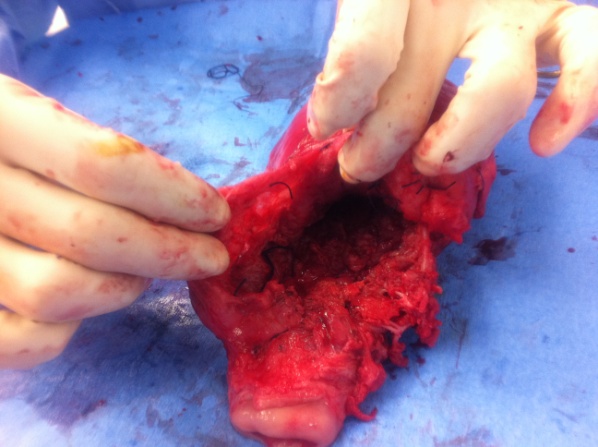 | Figure 2. Placenta Accreta with Scar dehiscence : intact Uterine serosa with incomplete rupture previous scar [lateral view] |
2. Case Report
 | Figure 3. An abdominal ultrasound picture shows placenta covering the cervical os With the foetal head above [28weeks] |
3. Discussion
- The term placenta accreta is used to describe abnormal placental implantation with firm adherence to the uterine wall. The hallmark is the absence of the decidua basalis with an imperfect development of the fibrinoid (Nitabuch’s) layer. The risk factors for placenta accreta include placenta previa, a previous scar in the uterus, high parity, pregnancy at a late age and maternal smoking. The association between placenta previa and prior uterine scarring greatly increased the chance of developing placenta accreta . To and Leung reported a 35 fold increase in placenta accreta in patients with a scarred uterus10. Once previa occurs the risk of accreta is more likely to increase due to the imperfect development of the decidua basalis in the scarred area. Myometrial invasion of trophoblastic islands at the site of a previous cesarean section may cause uterine rupture long before the onset of delivery, as it happened in our patient.The most useful modalities for evaluating placental position and implantation are transabdominal and transvaginal ultrasonography. In studies with more 30 subjects, the sensitivity and specificity of ultrasound for detection of placenta accreta was 77 to 90 percent and 71 to 97 percent, respectively4. Finberg et al. reported a positive predictive value of 78% and a negative predictive value of 94%, with Doppler sonography and magnetic resonance imaging 5. In placenta accreta the hypoechoic boundary between the placenta is lost and the placenta appears continuous with the bladder wall. However, false positives can occur . Visualization of intraplacental sonolucent spaces (venous lakes or placental lacunae) adjacent to the involved uterine wall are strongly suggestive of placenta accreta. The above parameters were not not very specific in this patient. Dehiscence of the previous caesarean section scar was an unexpected finding in this patient. In a situation with a catastrophic hemorrhage and scar dehiscence severe fetal anoxia occurs and leads to increased foetal morbidity. In our case it took about 20 minutes from the time of diagnosis to delivery. However, action within a short time plays an important role in preventing maternal exsanguination and maternal death, before definitive surgical intervention can be successfully initiated. The incidence of emergency hysterectomy in cases of placenta previa accreta was 50% compared to 2% in the non-accreta group. The high incidence of the post partum haemorrhage, blood transfusion and emergency hysterectomy in cases of placenta accreta compared to placenta previa ascertains the severity of this condition6. Uterine conservation in placenta accreta requires multidisciplinary efforts, including the obstetrician, an intervention radiologist, anaesthetist, and the urologist/general surgeon in certain cases. The ability to secure haemostasis intraoperatively is the main determining factor as to whether uterine conservation can be considered or not8,9.Hysterectomy can be an undesirable action to take especially in low parity patients and in a conservative Malaysian population. Usually this step is taken when other traditional measures taken to stop hemorrhage fail. Once massive obstetric hemorrhage occurs it may not be possible to make uterine vasculature react to vasoconstrictor drugs because of the possible lack of constrictor reactivity of the uterine vasculature8. This failure of constriction may play a pivotal role in uncontrollable hemorrhage. Early diagnosis is important so that the patient can be prepared and adequately counselled with regard to treatment options available and their possible consequences. In our case, adequate resuscitation and urgent hysterectomy seemed to be the most appropriate treatment of choice. Regarding treatment, hysterectomy is probably the best option in a situation where haemostasis cannot be secured. The inconsistent premonitory signs and the short time for instituting definitive therapeutic action makes the scar dehiscence secondary to placenta accreta a more fearful event.
4. Conclusions
- The recent advances made in biology can detect and should play a future role in developing a better understanding of placental invasion. Co-operation of modalities like Magnetic resonance imaging hand in hand with ultrasound may provide more accurate diagnosis of placenta previa and the serious co-existing placenta accreta. Inclusion of MR imaging in the routine evaluation of patients with placenta previa may reduce hospital stays and reduce unfavorable outcomes.