-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Computer Science and Engineering
p-ISSN: 2163-1484 e-ISSN: 2163-1492
2024; 14(1): 15-23
doi:10.5923/j.computer.20241401.03
Received: Feb. 19, 2024; Accepted: Mar. 3, 2024; Published: Mar. 9, 2024

Design of a System to Reduce Patient Crowding at UTH
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLOwen Hangoma, Dr Evaristo Musonda, Ir D. Mubiligi
Electrical and Electronics Engineering Department, University of Zambia, Lusaka, Zambia
Correspondence to: Owen Hangoma, Electrical and Electronics Engineering Department, University of Zambia, Lusaka, Zambia.
| Email: |  |
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Patients at Zambia’s main Hospital, face challenges of long queues, prolonged waiting times between appointments, overcrowding, last minute appointment cancellations or rescheduling without prior notification. Patients are given “same-time” appointments, where patients are basically given the same time of appointments and have to contend for the services. Same-time appointments bring about overcrowding and time wastage on the patients side as well as unwarranted pressure on the medical personnel. Hospital patient appointments maybe made by the front desk personnel which may not be aware of the intricate details of the patients’ conditions. Investing in a patient information and appointment system help reduce these problems by efficiently outlining patient-to-staff relation. This mapped patient-staff relation and other mathematical and scientific models on patient appointments should reduce the waiting times, overcrowding and cancellations of appointments. The system will help medical personnel with scheduling of appointments and bookings, for consultations, tests or scans as well as give a quick brief patient history for better diagnosis and continuity of care. The system will not require alteration of existing processes but process variables quickly and efficiently within the existing appointment models and procedures. The system will help to easily standardise the patient appointments procedures consequently reducing scheduling time, improve patients flow and overall health care delivery.
Keywords: Electronic Health Strategy, Scheduling, Waiting list, Hospitals stay time, Patient crowding
Cite this paper: Owen Hangoma, Dr Evaristo Musonda, Ir D. Mubiligi, Design of a System to Reduce Patient Crowding at UTH, Computer Science and Engineering, Vol. 14 No. 1, 2024, pp. 15-23. doi: 10.5923/j.computer.20241401.03.
Article Outline
1. Introduction
- This research paper focusses on the design of a Hospital patient information and appointment system that is aimed at reducing patient crowding, stay and waiting time at the University Teaching Hospitals (UTH) in Lusaka Zambia.
1.1. Problem Statement
- The UTH is the main Hospital in Zambia and is one of the few referral hospitals that can attend to a number cases requiring specialist care and treatment. The hospitals have seen an exponential rise in a number of patients it attends to and admits [1]. With rising numbers of patients seeking medical services from the institution, it has become very difficult to avoid crowding [1] [2], long patient queues [3] and consequently long patient waiting time. Dr. Nakamba [3] in his Article noted a number of things that contribute to patient long stay at UTH, some of them being Human Factors, Lack of standardised admission processes, communication failures, inefficient information systems, no continuity of care and so on. A number of reasons of long stay at the hospital given by Dr. Nakamba can be minimised by a well-developed system hence, effectively reducing the long patient waiting time at UTH.The most common challenge for hospitals, their managers, and employees is to reduce operational costs and reach efficiency targets as most hospitals operate with limited resources [4]. Their quest to streamline the organization has traditionally prevented patients from moving comfortably throughout their visits and re-visits. Instead, patients are often placed in long waiting lines while receiving minimal information throughout their stay [4].
1.2. Motivation
- COVID-19 pandemic has been a wakeup call that a patient appointment system that would help hospital staff to spread out patient visits throughout a good period, can help maintain social distancing required according COVID-19 health guidelines and avoid crowding in the hospitals [2].Reduced patient waiting time at the hospitals is another motivation. In almost in all public hospitals, the waiting before one gets an appointment and waiting time between appointments is long painful and the process is not very friendly.Appointments at the Hospital are given on same time or first come first save basis and patients arrive at the Hospitals the same time, even though it may be obvious that others will not be attended to immediately or the same day. Patients may have to wait longs hours sometimes more than eight hours or days or weeks before the can simply see a consultant. This trend is one of the main causes of crowding and patients’ long wait times. Long queues can worsen a patient’s situation or can get worse whilst on these queues.
1.3. Overview
- This research will help medical personnel better manage outpatient and inpatient appointments, tests scheduling and provide seamless check-in for patients as they see consultants. The system offers strict and standardised patient appointments and auto scheduling, with a lot of work taken off the staff’s shoulders, they can focus on meeting and supporting for better experience.
1.4. Application of the Research
- This research provides means and mechanism for standardised and strict steering and control of patient flow in the hospitals. It will provide staff with real-time information on services and providers, tests schedules and provide seamless and controlled check-ins and controlled flow of patients as they seek medical services. The system would automate and minimise a lot of challenges faced by patients and staff [17]-[21] in hospitals.
1.5. Related Work
- There are a number of systems hospital appointments scheduling exist as projects individuals, organisations as well as government. A study on crowding management at UTH was done by Nakamba [3] in his article “HEALTH QUALITY MANAGEMENT- REDUCING CROWNDING”. The government through hospital management besides having strategies and policies on the use of ICTs in health sector [6], it also attempts to reduce crowding in the Hospital Premises by only allowing personnel in the premises that are seeking and assured to get service [1] [2]. Waiting or containment zones are provided as patient wait for services unlike to avoid localised crowding within the hospital premises. Government and Non-Governmental Organisation have also partnered on projects on patient-staff ratio monitoring Systems, patient health care continual and so on. A number of researches have been done on the appointments and scheduling [5] [7] while other with crowd management mind [8]-[16].
2. Methodology
- Descriptive research was used in order to provide an accurate and detailed description of the research problem. In this research methodology, a quantitative and qualitative approach were adopted, where a prototype was designed and experiments were done on the system. Comparisons with other patient crowding management systems were done.
2.1. Research Tools
- Tests were conducted on the system applications developed. The Mobile applications were installed on Infnix hot 6 mobile devices and while web and database applications were installed on the desktops and its performance tested and simulated the results met the primary objectives and was satisfactory. Automation of hospital appointment was done using a database and web application as well as a mobile phone application. Other tools that were used in this study include; Android studio for mobile phone app development, MySQL DBMS for Database Creation and Management, PHP, JavaScript and Apache for web development and testing.
2.2. System Design Testing and Simulation
- Experiments and tests were done, 13 people helped simulate what would be the actual environment the patients and doctors would be exposed to or experience. People involved in the study performed roles of being the patients or health staff during the enacting and testing phase.
2.3. Applications Development Process
- The Web and Mobile android Applications were developed and tested for functionality. The mobile application was tested in the android studio emulator as well as on an actual android phone of model Infinix Hot 6.
2.4. Patients Flow
- From the data that was corrected and analysed from literature review, patient flow at the hospital was summarised as shown in figure 1 below. The activities at the hospital showed a pattern or trends. These trends revealed an order or the chronology, the importance and likeliness of occurrence and possible bypass/skipping of some of activities and stops at the Hospital. The Patient Hospital visit flow diagram outlines and groups related activities into definite Nodes or stops called stations on the patient flow. The stops/stations are facilities or functions where patients get a particular service in the hospital. These stations may be skipped depending on the nature of the visit and the priority of the case severity.
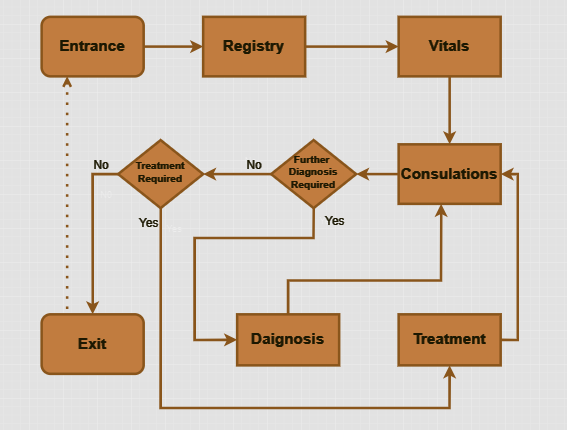 | Figure 1. Patient Hospital visit Flow Chart |
2.5. Requirements
- A number of system requirements were identified and compiled. A system to reduce patient crowding and hospital waiting time hence reduce patient hospital visitation time was envisioned. It was discovered that our project has requirements that a general patient appointment system may have and the additional ones for example, the purpose of this project, a system to check patient concentrations and strict control of patient flow and the requirements were identified as follows;• Timely notification on appointment rescheduling or cancellation.• Memory of previous and pending appointments.• Patient-to-staff Mapping.• Good prediction of hourly, daily, weekly, monthly and yearly averages of the number of “first comer” and “turn around” patients.• Online booking and notifications.• Tracking of the number of patients in a queue and number of staff available at every station.• Accept data on max number of patients that can be attended to at every station within a given period and calculate recommended number of patients in the premises.• Update patients on number of pending patients ahead and approximate waiting time. • Patient waiting list Management.• VIP and Ordinary Patient differentiation.• Resource Sharing availability prediction and Management.
2.6. Design
- The System design has three main components and these are, Database, Web Server and GSM SMS Module, Shown in figure 2 below is the core system design and components.
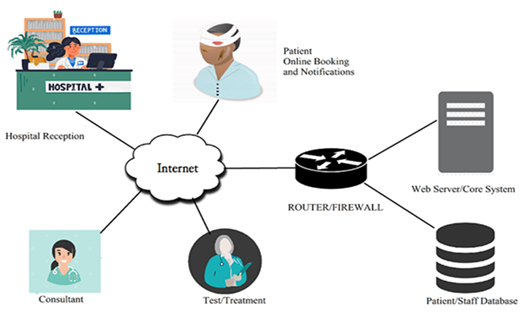 | Figure 2. Main System Design and Components |
2.6.1. Data Flow
- In order to achieve the aim, the system needs to keep and track the master scheduling list, track the current hospital visits and work out availability of staff and services.
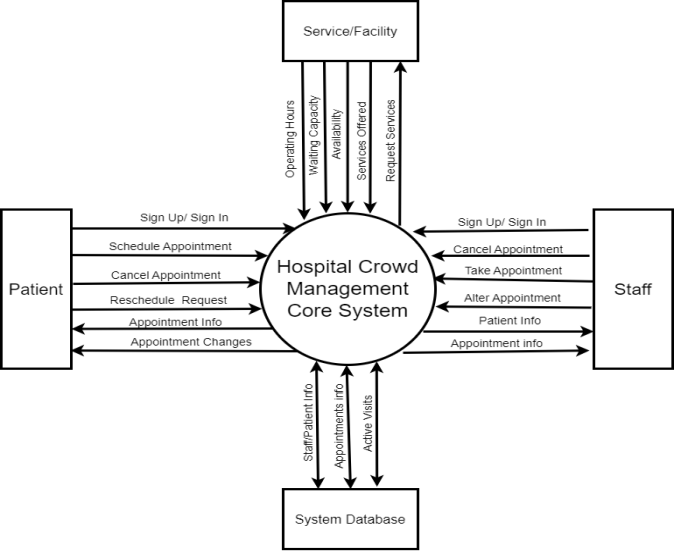 | Figure 3. Design Context Diagram |
2.6.2. Database Design
- From the identified requirements, number of database Entities and relationships were identified. The identified requirements were used to come up a database relational model. The database design has relations/tuples as listed and shown in the schema in figure 4 below.n PatientContains the patients details that important in identifying and reaching the patients, details like contact details, residential address and next of keen.n Staff Staff Relation just like the Patient relation contains entries that identify the Staff and their contact details.n Stations This relation contains the details about that facility on its availability and services conducted there.n Vitals This table contains readings from the patient for each particular visit.n Appointments These are the scheduled appointments, in the past, present or future. Dates, patient, assigned Staff/Consultants are some of the entries found here.n Consultants These Consultants are health professionals and members of Staff that gather and Analyse data from patients and draw conclusions and advise on findings to the patients on behalf of the hospital. This relation contains professional Job description and the services the services the consultants can attend to. n Staff_availabilityStaff Availability contains the details about the periods the staff is available for work to attend to patients.n office_timeThis where the time a facility or station’s working periods are defined. Holidays, days of the week and so on can be defined here.n visits This relation contains the data accumulated during a patient’s visit. This is also a record of the past visits.n active_visits Records current and active visits’ data that is import in steering the flow of patients in the premises. This data helps track the current location ad possible next stations of the patient in the provisional steps in the patient hospital visit. These Tables or relations contains fields that represent that particular relation and represents data that is required for system to effectively control and steer the patient flow in and out of the Hospitals.
 | Figure 4. Database Schema |
2.6.3. Database Physical Implementation
- The database was implemented using MySQL Database Management System software running on windows platform. The database access is done by a web application with PHP server side scripting. Database data definition, data Manipulation, and data access and any there processes on the data are primarily done by the web application which is the interface between user and database.
2.6.4. Patient Data Security and Storage
- The storage and management of patient data, as well as obtaining patient consent, are critical aspects of implementing a system to reduce patient crowding at the University Teaching Hospitals (UTH) in Zambia. Below are recommendations for storing patient data and ensuring patient consent:1. Centralized Database:• Implement a centralized database system to store patient information securely.• Utilize a reliable Database Management System (DBMS) such as MySQL, as mentioned in the methodology.2. Database Design:• Follow the conceptual and physical design outlined in the document, including entities like Patient, Staff, Appointments, Consultants, and others.• Ensure that the database design complies with data protection and privacy regulations.3. Security Measures:• Implement robust security measures to protect patient data from unauthorized access.• Use encryption for sensitive information and secure communication channels between the web server and the database.4. Backup and Recovery:• Regularly backup the database to prevent data loss in case of system failures or other unforeseen events.• Establish a recovery plan to quickly restore data in case of a database failure.
2.6.5. Patient Consent
- 1. Informed Consent:• Develop a clear and concise informed consent form that outlines the purpose of collecting patient data, how it will be used, and the security measures in place.• Ensure that patients understand and agree to the terms before their data is collected.2. Opt-In Mechanism:• Implement an opt-in mechanism where patients actively agree to participate in the system.• Clearly state that participation is voluntary and that patients have the right to withdraw consent at any time.3. Transparent Communication:• Communicate transparently with patients about the benefits of the system, how it improves their experience, and the measures taken to protect their privacy.• Provide contact information for any questions or concerns regarding data usage...4. Compliance with Regulations:• Ensure that the system complies with local and international data protection regulations in Zambia.5. Patient Education:• Conduct awareness campaigns to educate patients about the new system, emphasizing the positive impact on reducing waiting times and improving healthcare services.6. Continuous Monitoring:• Regularly monitor and audit the system's consent management processes to ensure ongoing compliance with regulations and ethical standards.By following these recommendations, you can establish a patient data management system that prioritizes security, transparency, and patient consent, contributing to the success of the overall initiative to reduce patient crowding at UTH.
3. Results
- The system design and simulation results showed a lot of evidence that if fully and properly implemented or installed at UTH or any other Hospital, it would greatly help reduced patient crowding at the hospital. The system closed a lot of gaps between the patient and the health givers that would help improve relationships between patients had hospital staff and management. From the results it was shown that the system would give staff more time to do critical and core functions than spend much time in steering and managing patients’ stay at the hospital and management of appointments at the hospital. Some of the findings from simulated results are as discussed in the subsequent sections below.
3.1. Observations
- The system showed some improvement on a number of challenges the hospital faces when it comes to patient crowding management. The positive outcomes demonstrate potential of use of ICTs in health care. The design promoted the need for patients to visit the hospital only when the Service assured and won’t be delayed. The observations were made and are as listed below;• Sequential appointments or patient arrival at the Hospital unlike patients arriving at the same time as it happens currently.• Steered and controlled flow patients during hospital visits reduced patient waiting time and hence increased patient comfort.• Improved patient Staff relationship and awareness Reduced time spent on patient appointment management Standardised processes of patient appointment scheduling.• There was little or no change in the time to handle a patient for a numbers services sought after.• Missed and Cancelled appointments were clearly reported and health care alerted as well as the patients reminded.• The Design did not make any distinction between outpatient and in-patient however this distinction could be made by available functions of priority in patient cases set by staff.• Emergency cases, Status (i.e. VIP, VVIP, Aged) or perhaps any other differentiation of patients was only identified by the level of urgency or priority as acknowledged and defined by the staff.
4. Discussions
- Three research objectives were identified that were found to be useful in developing a feasible patient crowd management system design. The crowd Management system would oversee and manage the patient waiting list, the accessibility and availability of medical services and facilities as well as the presence of medical providers. The System would be accessed both on-site and off-site for the benefit of patients and as well as medical staff. Chapters three, four, and a portion of chapter two have all had in-depth discussions of these study objectives. In order to achieve the first objective, the comparison of systems currently in use at UTH and world around in crowd management and healthcare appointments, and procedures were made by review of pertinent literature produced by academicians and other authors in this field. This made it easier to examine various patient crowding management techniques, such as use of automatic, smart or manual systems. The existing system were examined in order to improve the design of the patient crowding control system at UTH hospitals. In the literature review, specifics that address this research goal are presented. The advantages of this crowd management system over existing hospital appointment systems have also been discussed and it has been thoroughly examined. The system is a web based and is built on a web server, database, mobile phones, Database and web and Mobile applications. The codes can be checked and tested in android studio with a virtual mobile phone emulators as well as the real smart phone device. A web Server and database were deployed and the mobile phones and PCs were connected during testing.Objective two as discussed in chapters one, to be met, the patient hospital visitation activities and trends have been analysed as a tool that would help develop a patient crowd management conceptual model. In achieving this objective, we identified functional and non-functional activities of patients and staff during appointments and patients hospital visitations. Non-Functional activities that are not core to a patient getting medical service but are important to the comfort and a good working relationship between the patient and the medical staff. Formulation and Listing of system requirements was done and conceptual model was developed.In order to achieve the third objective, the system was developed and tested and the system is functioning in accordance with the design requirements. Significant aspects of the system's components and the design process were covered in Design section above, and the results section presents the findings to that effort. The medical staff providing medical services and the individuals in need of or seeking medical attention can easily use the system by following a few easy procedures.
5. Challenges and Shortfalls
- While the designed system aimed at addressing issues related to patient crowding and patient waiting times, there are a number of shortcomings and challenges that should be considered for further improvement. Challenges were experienced during research at almost all the stages research. Developing the mobile and web applications and correcting data were some of the hurdles this study faced.
5.1. Challenges
- The following were some of the difficulties encountered during the research and the system's design and development;a. Creating applications: Android Studio was installed on low end PC and it was slow for comfort and speedy development, it took a long time and required patience. Android took up significant space of hard disk drive (HDD) and RAM memory, virtual devices simultaneously took up a significant amount memory.b. The Android application debugging and testing: When booting the Android application on the hardware used, it was occasionally slow and even slower to test on the emulator in Android Studio. Due to the sluggish creation and termination of the software, we had to wait a long period to test it on a physical device (a smartphone). c. Update of Android Studio: Android Studio frequently asks for updates. Testing the developed app on the most recent iterations of Android Studio presented a challenge, since errors kept occurring. It took some time to get rid of these bugs. The pace was negatively impacted, and it took some time to fix.d. Emulator Shortfalls: Not all functions that would be available on the actual phone were available on the Android emulator which required me to switch between the emulator and actual phone.e. The Single PC was used as a web server, database management system and web client during development. As the result some communications bugs were difficult to catch until different PCs were used slowing the whole process. The Bugs were discovered later which required more debugging time.f. Web Application coding was done using simple text editors which made the development process slower and difficult to debug code.
5.2. System Shortfalls
- Although was able to meet the primary objectives, the system has these shortfalls:a. Limited Distinction Between Outpatient and Inpatient:Due to shared resources between inpatients and outpatient, the system does not make a clear distinction between outpatient and inpatient cases. It could be beneficial to incorporate features that cater specifically to the needs and processes associated with inpatient visits.b. Emergency Cases Handling: The system does not explicitly address the handling of emergency cases. Emergency cases might require a different and expedited and complex process, although this can be handed by higher case priority the feature programmed into.c. Lack of Integration for Real-Life Data:The system doesn't incorporate real-life data readings (e.g., temperature, blood pressure) for patients with specific medical conditions. Integrating real-time health data could enhance the advisory function and provide more personalized recommendations for patients.d. Limited Differentiation of Patients:The system only identifies patients based on the level of urgency or priority as acknowledged by the staff. Further differentiation based on emergency status, VIP, VVIP, or age could provide more tailored services and prioritize specific cases.e. SMS Notification to Offline Doctors/Patients:The system lacks a feature to notify doctors via SMS in case they are offline which would delay possible timely data update.f. Maintenance Master patient waiting list: The recommendation for a master list should be carefully implemented to ensure data security, privacy, and compliance with regulations. This list needs to be accessible by facilities under different management so they know expected guests.Addressing these shortcomings will contribute to the overall effectiveness and usability of the patient information and appointment system, leading to better patient experiences and improved healthcare delivery at UTH.
6. Conclusions
- Despite a number of systems on patient databases, information and appointment management systems that have been developed over the years, there exists less to no adoption in the most of the public hospitals in Zambia especially at UTH. Patients have continued to be subjected to long waiting queues and cancellation or postponement of appointments mostly due to poor appointment scheduling and no waiting lists management. Patient crowding at UTH has only gotten worse as the country’s population increase and so are the people seeking medical services from the institution.This research sought to find out and address the issue of patient crowding and reasons for poor use of digital systems in hospitals in managing patient appointments, crowding and treatments advisory and many other advisory functions that can be performed by digital systems. The goals of this research were achieved by the system's design results. Consequently, we can more accurately anticipate patient congestion with the use of this automated technology approach, allowing us to take the necessary action to either avoid or minimize the issue. In order to give users/patients greater freedom in scheduling appointments and to guarantee that they will receive services upon their visit, information about their intentions to visit the hospital and the services they are seeking can be obtained from them in advance. Due to their portability and the established system's real-time appointment updates, mobile phones and PCs make it simple to track users or patients from anywhere at any time. When using computers and smartphones for personal healthcare services, it's critical to evaluate their accuracy and dependability.The creation of these intelligent patient crowd control devices, which offer low-cost solutions to crowding issues without requiring direct patient interaction or physical presence, has the potential to significantly alter the healthcare system during the COVID-19 pandemic. Because a variety of parameters are monitored, crowding can be predicted well before it happens. When changes occur over an extended period of time, patients can be called in when they are guaranteed a better level of care and attention. After a number of simulations and tests, error correction, and debugging, the system was finally able to function as expected and read and display the data that staff and patients might require.
7. Recommendations
- We recommend deliberate and strict management of patient waiting lists for all the Hospitals, clinics and other facilities the patients visit at UTH. We also recommend that these lists be shared and combined into one master list to hep crowd management at the institution.We recommend availability of staff and services should be logged and strictly adhered to throughout year or the period under consideration.It is recommended that the patient be availed with the provisional map and possible routes (flow charts) they would take during their visit at the hospital so that can mentally visualise their visit progression. It is recommend that each equipment, service or station at the station should have an availability, booking and utilisation logs so as the system can give a more accurate advice.Our idea for the system going forward is to give mobile users access to a list of doctors and staff that they may subscribe to, along with their location. This will allow them to select medical professionals who are closest to them, making it easier for the local doctors to contact them in an emergency. We advise backup plan for appointment for users/patients in the event that the initial doctor scheduled to see them is unavailable or far away, allowing the patient to be contacted and seen by the backup physician.We suggested that, because this was not included in our work, the system should in the future be able to create SMS and send notification alerts to the doctor in case the doctor in question is offline.We recommend real-life data (i.e. temperature and blood pressure) reading and collection from patients with certain medical conditions so as enable prompt automatic advisory function to the patient on when they can visit the medical facilities as well as automatic advice and selection of the severity of the patient condition by the system.