-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Clinical Medicine and Diagnostics
p-ISSN: 2163-1433 e-ISSN: 2163-1441
2026; 14(1): 6-11
doi:10.5923/j.cmd.20261401.02
Received: Feb. 20, 2026; Accepted: Mar. 10, 2026; Published: Mar. 27, 2026

The Role of Videostroboscopy in the Preoperative Diagnosis of Benign Laryngeal Neoplasms
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLA. N. Abbasov1, G. S. Khaydarova2
1University of Business and Science, Tashkent, Uzbekistan
2Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: A. N. Abbasov, University of Business and Science, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Benign laryngeal neoplasms account for 50–70% of all tumors in this anatomical region and are detected in 15–25% of patients presenting with dysphonia. Despite the development of modern endoscopic technologies, accurate preoperative verification of lesion depth and structural involvement remains a significant clinical challenge. Objective: To investigate the clinical, functional, and endoscopic characteristics of benign laryngeal neoplasms in order to improve the accuracy of preoperative diagnosis and optimize surgical treatment strategies. Materials and Methods: The study included 102 patients with benign laryngeal tumors (papillomas, fibromas, and chondromas). Clinical examination, videolaryngoscopy, videostroboscopy, and morphological analysis were performed. Results: Differential videostroboscopic features were identified for different morphological types of benign laryngeal lesions. Papillomas were characterized by multiple lesions and inflammatory mucosal changes, fibromas by localized rigidity without deformation, and chondromas by deformation of the laryngeal framework and significant reduction of vibratory amplitude. Conclusion: Integration of videostroboscopy into the diagnostic algorithm significantly improves the accuracy of preoperative diagnosis and facilitates the selection of optimal surgical tactics.
Keywords: Benign laryngeal tumors, Videostroboscopy, Papilloma, Fibroma, Chondroma, Dysphonia
Cite this paper: A. N. Abbasov, G. S. Khaydarova, The Role of Videostroboscopy in the Preoperative Diagnosis of Benign Laryngeal Neoplasms, Clinical Medicine and Diagnostics, Vol. 14 No. 1, 2026, pp. 6-11. doi: 10.5923/j.cmd.20261401.02.
1. Introduction
- Benign laryngeal lesions occupy a significant place in the structure of organic pathology of the vocal apparatus and upper respiratory tract. According to epidemiological studies, their proportion accounts for 50–70% of all tumor and tumor-like processes of the larynx [1]. In outpatient otorhinolaryngological practice, this pathology is detected in 15–25% of patients presenting with complaints of dysphonia [2]. The social significance of the problem is associated with the high prevalence of voice disorders, especially among individuals of voice-speech professions, whose proportion reaches 30–45% [3].Benign laryngeal lesions are most commonly diagnosed in patients aged 25–55 years, which corresponds to the period of highest professional activity [4]. Gender differences are manifested in the predominance of vocal fold nodules in women (up to 60%), while polyps and hyperplastic processes are more common in men (55–65%) [5,6].A special place is occupied by laryngeal papillomatosis, the incidence of which accounts for 10–15% in the structure of benign laryngeal neoplasms [7]. The disease is associated with the human papillomavirus (HPV), predominantly types 6 and 11, the DNA of which is detected in more than 80% of cases of recurrent respiratory papillomatosis [8,9]. The juvenile form occurs with a frequency of 3–4 cases per 100,000 children, while the adult form occurs in 1–2 cases per 100,000 population [10]. Despite its benign nature, the disease is characterized by a high recurrence rate (up to 70%) [11].Vocal fold polyps account for 30–40% of organic lesions of the vocal apparatus [12]. Vocal nodules are more frequently detected in individuals with prolonged vocal load and reach a prevalence of 12–20% among voice professionals [15,16]. Laryngeal cysts account for 5–10% of cases, while vascular lesions represent up to 5%.The classification of benign laryngeal lesions is based on histogenetic, morphological, and clinical principles. Epithelial lesions (papillomas), connective tissue lesions (fibromas, polyps), vascular lesions (hemangiomas), cystic, and mixed forms are distinguished [5]. According to localization, supraglottic, glottic, and subglottic processes are identified. The clinical course is also taken into account, distinguishing primary and recurrent lesions, as well as solitary and multiple forms.Despite the existence of various classification systems, modern literature emphasizes the need for unification of terminology and morphological criteria. This would improve the comparability of research results and contribute to the standardization of therapeutic approaches.The clinical and anatomical features of benign laryngeal lesions are determined by the complex anatomical and functional organization of the larynx, which performs respiratory, phonatory, and protective functions. Even limited structural changes in the mucous membrane and the lamina propria of the vocal folds can significantly disrupt the biomechanics of phonation [15,16].The most vulnerable area is the region of the true vocal folds, which is due to their high vibratory load and the structural features of Reinke’s space—the superficial layer of the lamina propria that provides the mucosal wave essential for normal phonation. It is within this layer that polyps, nodules, and Reinke’s edema most commonly develop.The main clinical manifestation is dysphonia (up to 90% of cases), presenting as hoarseness, reduced vocal intensity, and rapid vocal fatigue. When lesions are localized in the subglottic region, inspiratory dyspnea and stridor may occur.Vocal fold polyps are typically characterized by unilateral localization and disruption of the symmetry of vocal fold vibration. Vocal nodules are usually bilateral, located at the junction of the anterior and middle thirds of the vocal fold, and form the characteristic “hourglass” configuration during phonation. Laryngeal papillomatosis is distinguished by multiple papillary proliferations and a tendency for spread. Cysts and vascular lesions may lead to significant functional impairment as their size increases.The clinical and anatomical features of benign laryngeal lesions represent an important section of modern otorhinolaryngology, since the anatomical and functional organization of the larynx determines the specific characteristics of the clinical manifestations, diagnosis, and treatment of this pathology. The larynx is a complex organ that performs respiratory, phonatory, and protective functions, and any structural changes in its mucous membrane, submucosal layer, or cartilaginous framework affect the quality of phonation and the patency of the airways [8]. Benign laryngeal lesions, despite the absence of invasive growth and metastasis, may significantly disrupt the biomechanics of the vocal folds, leading to chronic dysphonia and, in some cases, to stenotic phenomena.Anatomically, the larynx is divided into the supraglottic, glottic, and subglottic regions, each of which has specific morphological and functional characteristics [11]. The most vulnerable area with regard to the development of benign lesions is the true vocal folds, which is explained by their maximal vibratory load and the structural features of the lamina propria of the mucous membrane. The lamina propria consists of superficial, intermediate, and deep layers, forming the so-called Reinke’s space, which plays a key role in the vibration of the vocal folds [17]. It is within this layer that polyps, nodules, and edematous changes most commonly develop due to microtrauma and vascular disturbances [13].The clinical manifestations of benign laryngeal lesions are determined by their localization, size, morphological structure, and the degree of impairment of vocal fold closure [7]. The most common symptom is dysphonia, the frequency of which reaches up to 90% among patients with this pathology [3]. Dysphonia may manifest as hoarseness, reduced vocal intensity, rapid vocal fatigue, and alterations in voice timbre and range. When the lesion is localized in the subglottic region or reaches a significant size, inspiratory dyspnea and stridor may develop [1].Vocal fold polyps are characterized by unilateral localization, most often located on the free edge of the middle third of the vocal fold, and may have either a soft or dense consistency. Morphologically, they are represented by edematous or fibrous stroma with dilated vessels and signs of chronic inflammation. Clinically, polyps manifest as persistent hoarseness and a sensation of a foreign body in the throat. Their anatomical location disrupts the symmetry of vibration, causing asynchronous oscillations of the vocal folds.Vocal fold nodules, in contrast to polyps, usually have a bilateral symmetrical character and are formed at the junction of the anterior and middle thirds of the vocal folds. Their development is associated with chronic vocal overuse and functional dysphonia [16,17]. In the early stages, nodules present as soft edematous lesions, but over time they undergo fibrotic transformation [1]. The anatomical feature of their location results in the formation of the characteristic “hourglass” configuration during phonation [9].Laryngeal papillomatosis is characterized by multiple papillary proliferations of the mucous membrane, predominantly in the supraglottic and glottic regions [5]. The lesions have an irregular surface and tend to exhibit diffuse growth. Clinically, papillomatosis manifests as progressive dysphonia, and in cases of extensive involvement, respiratory insufficiency may develop. In children, the disease is often accompanied by frequent recurrences and involvement of the subglottic space.Laryngeal cysts are predominantly localized within the vocal fold or in the region of the laryngeal ventricles. They may be retention or epidermoid cysts and are characterized by well-defined borders and a smooth surface. When small, cysts may remain asymptomatic, but an increase in their size can lead to impairment of the vibratory function of the vocal fold.Vascular lesions, including hemangiomas, are more often detected in the subglottic region and in young children. Their clinical significance is associated with the risk of airway stenosis. Morphologically, they are represented by proliferation of vascular elements and may have either a capillary or cavernous structure.A special group includes contact granulomas, which are localized in the posterior parts of the vocal folds in the region of the vocal processes of the arytenoid cartilages [15]. Their formation is associated with trauma to the mucous membrane during intubation, gastroesophageal reflux, and hyperfunction of the vocal apparatus [1]. Clinically, they manifest as discomfort, pain during phonation, and frequent throat clearing.The anatomical features of the blood supply and lymphatic drainage of the larynx also influence the course of benign processes [15]. The rich vascular network contributes to the development of edema and inflammatory reactions, especially in the region of Reinke’s space [11]. At the same time, the limited submucosal space in the subglottic region explains the rapid development of stenotic phenomena even in the presence of small lesions [7].Modern visualization methods have significantly expanded the understanding of the clinical and anatomical features of this pathology. Video laryngoscopy allows detailed assessment of the localization and size of the lesion [2]. Videostroboscopy provides the possibility to analyze the vibratory function of the vocal folds and detect asymmetry of oscillations [7]. The use of high-frequency endoscopy and narrow-band imaging increases the accuracy of differential diagnosis.Morphofunctional studies demonstrate that even small lesions can significantly disrupt the mucosal wave and alter the biomechanics of phonation. The severity of clinical manifestations does not always correlate with the size of the lesion, which emphasizes the role of its localization and depth of tissue involvement [9]. An important aspect is also the condition of the contralateral vocal fold, which may undergo compensatory changes [6].Thus, the clinical and anatomical features of benign laryngeal lesions are determined by the complex organization of the vocal apparatus and the functional load on its structures. The localization, morphological type, and size of the lesion form the individual clinical profile of the disease [10]. Understanding these features is essential for selecting an adequate diagnostic and therapeutic strategy, as well as for predicting disease outcomes [8].Aim of the studyTo develop and substantiate an improved algorithm for videostroboscopic differential diagnosis of various forms of benign laryngeal neoplasms.
2. Materials and Methods
- The study included 102 patients with benign laryngeal tumors who underwent examination and treatment at the ENT Department of the Multidisciplinary Clinic of Tashkent State Medical University between 2024 and 2026.The patients were divided into three groups according to the morphological type of the tumor. Group I consisted of 34 patients with laryngeal papillomas, Group II included 40 patients with laryngeal fibromas, and Group III comprised 28 patients diagnosed with laryngeal chondromas.The inclusion criteria were age 18 years or older, the presence of clinically and histologically confirmed benign laryngeal tumors, and the presence of characteristic clinical manifestations such as dysphonia, hoarseness, or respiratory disturbances. The diagnosis was confirmed using videolaryngoscopic examination followed by histological verification. All patients provided written informed consent prior to participation in the study.Patients were excluded from the study if there was a suspicion of malignant laryngeal tumors or histologically confirmed high-grade epithelial dysplasia. Additional exclusion criteria included severe decompensated systemic diseases (cardiovascular, renal, or hepatic failure), acute infectious diseases, autoimmune disorders, and pregnancy or lactation.The diagnostic protocol included a comprehensive clinical evaluation consisting of clinical examination, indirect laryngoscopy, videolaryngoscopy, videostroboscopy, and histological examination.Functional assessment of vocal fold vibration was performed using videostroboscopy and included evaluation of the mucosal wave, amplitude of vocal fold oscillations, symmetry of vibration, and completeness of glottic closure during phonation.Statistical analysisStatistical analysis was performed using SPSS software (version XX, IBM Corp., USA). Categorical variables were presented as percentages and compared using the Chi-square (χ²) test or Fisher’s exact test when appropriate. Continuous variables were expressed as mean ± standard deviation and analyzed using Student’s t-test or one-way ANOVA.A p-value < 0.05 was considered statistically significant.Confidence intervals (95% CI) were calculated where applicable.
3. Results
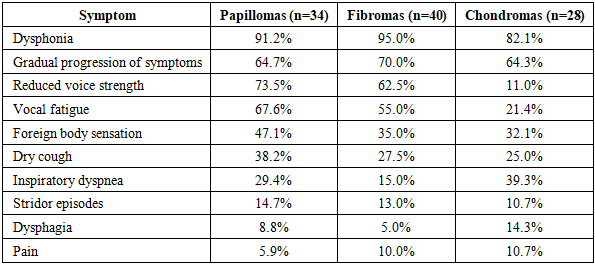
- The most common clinical manifestation across all groups was dysphonia, with no statistically significant difference between groups (p = 0.18).However, several symptoms demonstrated statistically significant differences:• Reduced voice strength was significantly more frequent in papillomas and fibromas compared to chondromas (χ² = 18.4, p < 0.001)• Vocal fatigue was significantly higher in papillomas (χ² = 12.7, p = 0.002)• Inspiratory dyspnea was significantly more common in chondromas (χ² = 9.6, p = 0.008)
|
|
|

|
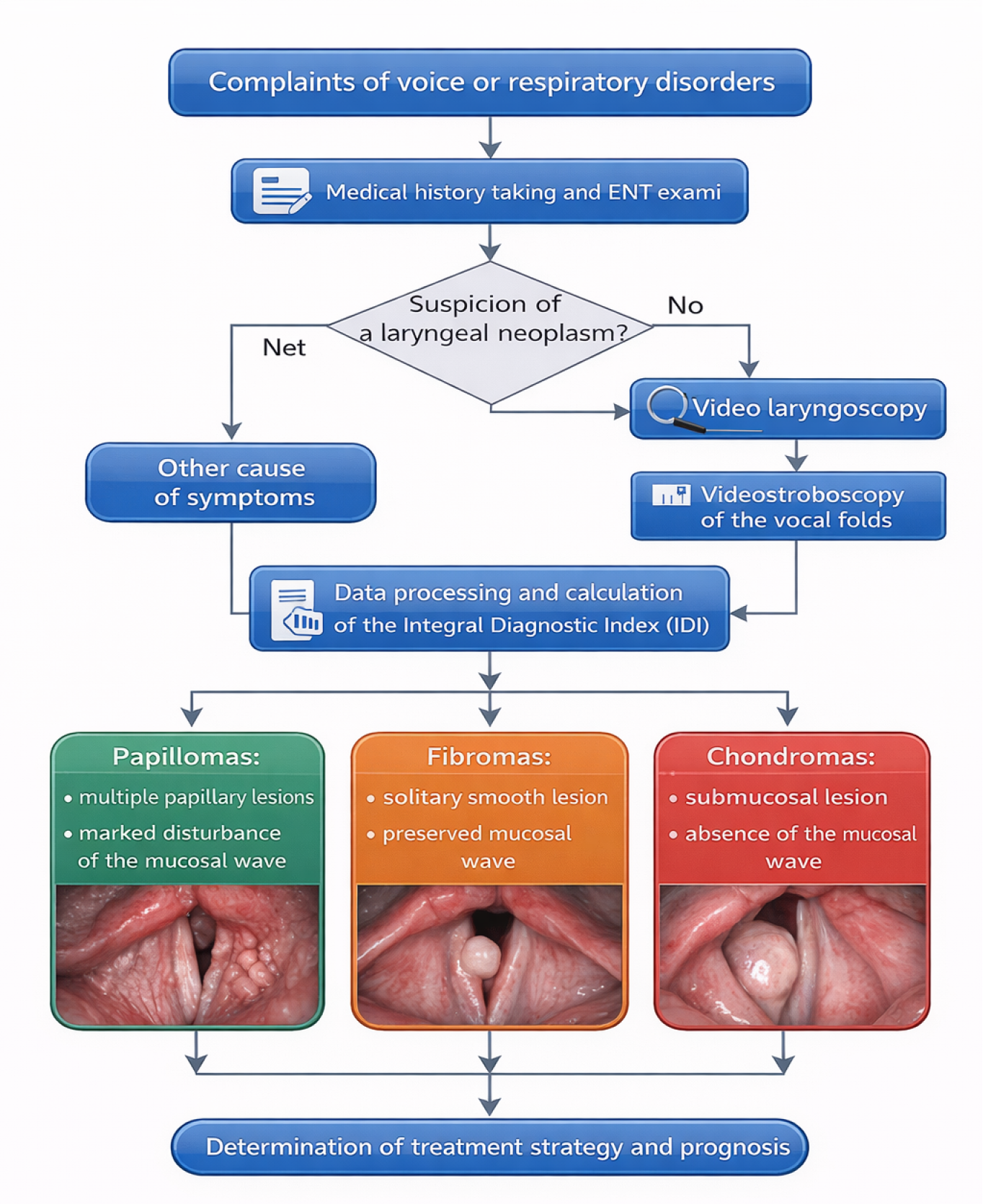 | Figure 1. Algorithm of videostroboscopic diagnosis of benign laryngeal neoplasms |
4. Discussion
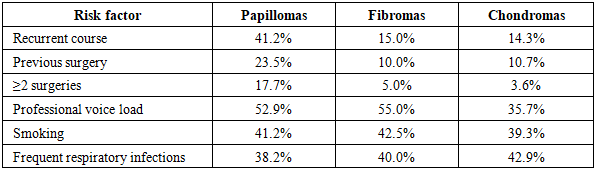
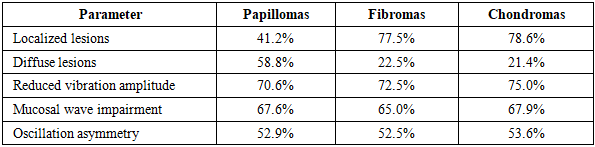
- The present study demonstrated statistically significant differences in clinical and functional characteristics of benign laryngeal neoplasms depending on their morphological type.Papillomas showed a significantly higher rate of recurrence (p = 0.004) and inflammatory changes (p < 0.001), which is consistent with their viral etiology and chronic course described in previous studies (Derkay et al., 2019).Fibromas were characterized by localized lesions without significant inflammatory changes, confirming their primarily mechanical origin associated with chronic vocal load.Chondromas demonstrated a significantly higher prevalence of respiratory symptoms (p = 0.008) and laryngeal lumen narrowing (p = 0.02), which is explained by their localization within the cartilaginous structures of the larynx.Importantly, videostroboscopic parameters such as mucosal wave and oscillation symmetry did not differ significantly between groups (p > 0.05), indicating that structural rather than purely functional parameters are more valuable for differential diagnosis.These findings highlight the importance of combining clinical, endoscopic, and functional data in a comprehensive diagnostic algorithm.The results of this study are consistent with international data and confirm that videostroboscopy significantly improves the accuracy of preoperative diagnosis and helps to determine optimal surgical tactics.
5. Conclusions
- Benign laryngeal tumors demonstrate different clinical and functional characteristics depending on their morphological type and depth of involvement.Videostroboscopy allows identification of differential diagnostic features of papillomas, fibromas, and chondromas and significantly improves the accuracy of preoperative diagnosis.Integration of videostroboscopic examination into the diagnostic algorithm contributes to optimal selection of surgical treatment strategies.