-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Clinical Medicine and Diagnostics
p-ISSN: 2163-1433 e-ISSN: 2163-1441
2019; 9(3): 41-46
doi:10.5923/j.cmd.20190903.01

The Crucial Prognostic Role of Serum Cholinesterase in Detecting Liver Disease
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLHeba-t-Allah Hamdy El-sayed1, Eman Fekry Mohamed1, Karima Youssef Ahmed1, Iman Mohamed Said ElBagoury2
1Department of Internal Medicine, Faculty of Medicine for Girls, Al- Azhar University, Cairo, Egypt
2Department of Clinical Pathology, Faculty of Medicine for Girls, Al- Azhar University, Cairo, Egypt
Correspondence to: Eman Fekry Mohamed, Department of Internal Medicine, Faculty of Medicine for Girls, Al- Azhar University, Cairo, Egypt.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

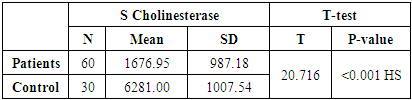
Liver diseases are considered as the foremost cause of morbidity and mortality around the world, especially in developing countries and classified into acute and chronic liver disease. Further, hepatocytes synthesize the cholinesterase (ChE) and enhances their catalysis through hydrolysis mechanism of the acetylcholine to into choline and acetic acid. This study aims to give a comprehensive account of the vital prognostic and diagnostic marker role of cholinesterase of liver cirrhosis over other known liver function tests (LFTs) like ALT, AST, serum albumin and serum bilirubin. Subjects and methods: this study was conducted on 60 livers cirrhotic Egyptian patients, divided into three groups according to their Child-Pugh score and 30 healthy volunteers as a control group. Serum biomarkers for the liver disease were measured (cholinesterase, AST, ALT, Serum Albumin, Serum Bilirubin) in parallel with an abdominal ultrasound examination was made for all participants. The results: There was a highly significant decrease in serum cholinesterase levels in all patient groups diagnosed with liver cirrhosis compared to control and more in decompensated patients. Conclusion: the present study concluded that the blood cholinesterase can be used as an imaging profile for the degree of liver damage and prognostic level of cirrhosis.
Keywords: Liver function tests, Liver cirrhosis, Cholinesterase
Cite this paper: Heba-t-Allah Hamdy El-sayed, Eman Fekry Mohamed, Karima Youssef Ahmed, Iman Mohamed Said ElBagoury, The Crucial Prognostic Role of Serum Cholinesterase in Detecting Liver Disease, Clinical Medicine and Diagnostics, Vol. 9 No. 3, 2019, pp. 41-46. doi: 10.5923/j.cmd.20190903.01.
Article Outline
1. Introduction
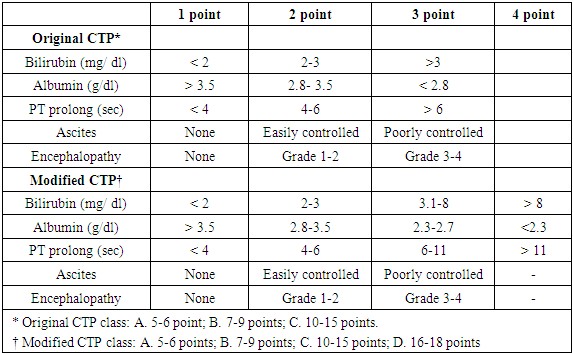
- Liver cirrhosis is considered as a noteworthy reason for death worldwide and a particular prickly national issue in Egypt [1]. In developed countries, regular reasons for cirrhosis, including, chronic viral hepatitis B, C [2]. Moreover, hepatitis C, alcoholic and nonalcoholic liver diseases have been considered the most well-known reasons for cirrhosis in the United States and were considered as the fundamental driver for roughly 80 percent of patients of the liver transplantation shortlist somewhere in the range of 2004 and 2013 [3]. Furthermore, individuals share needles for infusing medications and human services laborers or crisis specialists who might be presented to sullied blood are most defenseless and dependably in danger for contracting and spreading hepatitis C in risk for liver cirrhosis [4]. Patients with decompensated cirrhosis develop many serious and life-threatening symptoms and complications with early manifestations of rapid cirrhosis such as fatigue, loss of appetite, weight loss, nausea or abdominal pain and spider navi may develop on the skin [5].Besides, late phases of cirrhosis improve the progress to a decompensated phase with the development of edema, ascites, Jaundice, Itching (pruritus) developed from the development of bile items, Palmar erythema; in men gynecomastia, or shrinkage of the testicles, simple wounding and excessive bleeding may happen [6]. Patient with liver cirrhosis can be classified according to child score into child A, B and C. Moreover, the Child-Pugh score is still one of the important prevailed prognostic evaluation models for the chronic liver diseases ranging from light damage to cirrhosis that can be used in selecting the treatment quality. Moreover, it was considered as the most indicator of death in spite of the nonappearance of ascites, encephalopathy, and jaundice in the patients with compensated cirrhosis indicating that even subtle abnormalities in laboratory parameters are predictive of death [7]. The Pugh change of the Child-Turcotte characterization utilizes two clinical factors, ascites and encephalopathy, and three laboratory parameters such as serum bilirubin, albumin levels and prothrombin time as in table 1. Every factor is allotted a score from 1 to 3; with the total aggregate score figuring out the CTP score [8].
|
2. Subjects and Methods
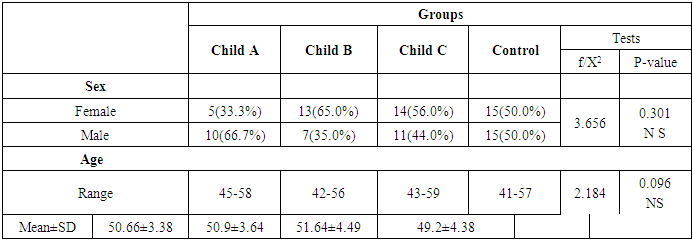
- This study is a case-control study. A total of 60 cirrhotic Egyptian patients with cirrhotic liver, age and sex were matched. The samples were classified as follows: 28 males (46.7%) and 32 females (53.3%) and their ages ranged from (42-59) years with mean±SD (50.45±3.92). All cases were admitted to the internal medicine department at El Zahraa University Hospital from November 2016 to September 2017. 30 apparently healthy volunteers were included in the study as a control group as follows: 15 males (50%) and 15 females (50%) and their ages ranged from (41-57) with mean ±SD (49.2± 4.38) years.Ethical consideration:All study participants' have stated oral consent before their enrollment in the study.Exclusion criteria: the present investigation has utilized some avoidance criteria that will restrain patients portrayed with one of them to be denied from the enrollments, for example, age under 18 years, history of albumin or blood transfusion a month earlier the enrollment, pregnant female, and a history of liver neoplasm or transplantation.Inclusion criteria for the study were: full history and clinical evaluation, laboratory investigations, including (Complete blood count (CBC) using Sysmex, KN21, liver enzymes (alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin, direct bilirubin, serum albumin), Kidney function tests (urea, creatinine), and Na & K. All of them were carried out using Cobas 311 clinical chemistry autoanalyzer, ROCH diagnostic company, Coagulation profile and Serum cholinesterase and abdominal ultrasonography.Sample collection and storage:Seven ml of venous blood was collected under complete aseptic technique conditions from patients and control in a sterile vacutainer tube. 1ml has been collected on Ethylenediaminetetraacetic acid (EDTA) solution for complete blood picture., 3ml was used in plain tube and left to clot followed by centrifuged at 2000×g for 10 minutes for serum separation, 2ml of blood was collected on citrate and centrifuged at 2000×g for 5 minutes for plasma separation to be used for PT, PC, and INR estimation. Routine biochemical investigations for liver and kidney have been measured almost immediately. The activity of serum cholinesterase was assessed with 2h of sample separation depending upon the reduction assay of the butyrylthiocholine substrate according to the Boehringer reagent kit protocol (Boehringer Mannheim GmbH, Mannheim, Germany) on an Olympus AU5400 Automatic Analyzer (Olympus Ltd., Tokyo, Japan).Statistical analysisSPSS software for Windows (ver. 20.0; SPSS, Chicago, IL, USA) was used for the statistical analysis of database management. Descriptive results were expressed as the mean ± standard deviation (SD). The unpaired t-test was carried out to compare the mean ±SD between every 2 groups and ANOVA to assess the differences between more groups. Additionally, the comparison of cholinesterase, albumin, and serum prothrombin times between the different groups has been calculated using the Pearson correction test. The statistically significant difference was assessed with P<0.05.
3. Results
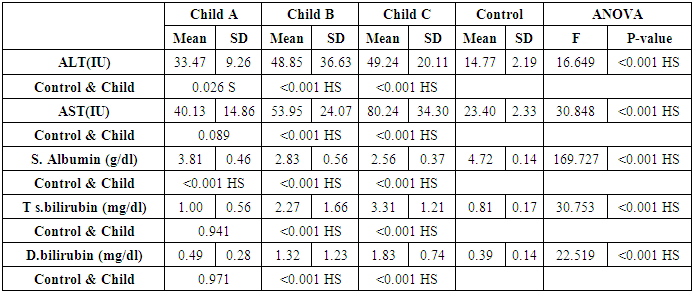
- The present study included a total of 28 male and 32 female patients with a mean age of (50.45±3.92 years). The patient’s basic demographic, laboratory analysis and endoscopic structures are summarized in Table 2. Moreover, Child-Pugh score for cirrhosis patients classified them to Child A group with 15 (25%), Child B with 20 (33.3%) and Child C groups in 25 (41.6%) as shown in table 2.
|
|
|
|
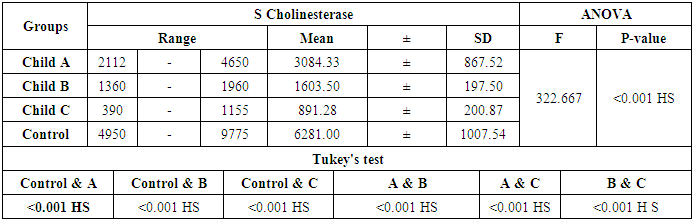
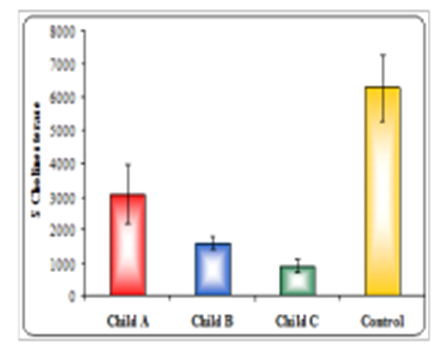 | Figure 1. Comparison between Serum cholinesterase in all groups |
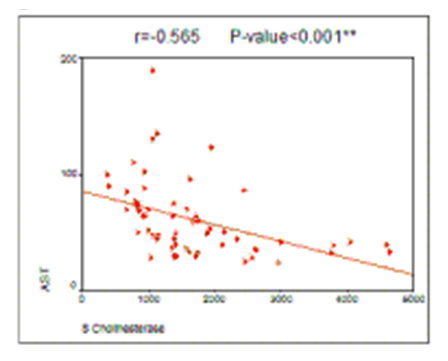 | Figure (2). Correlation between serum cholinesterase and AST |
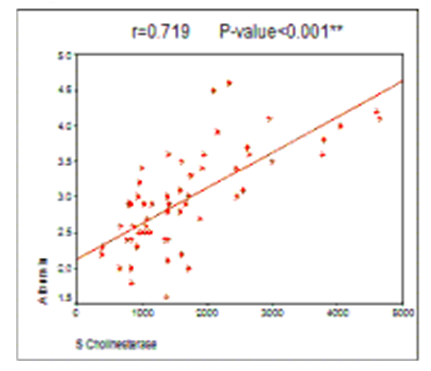 | Figure (3). Correlation between Albumin and serum cholinesterase |
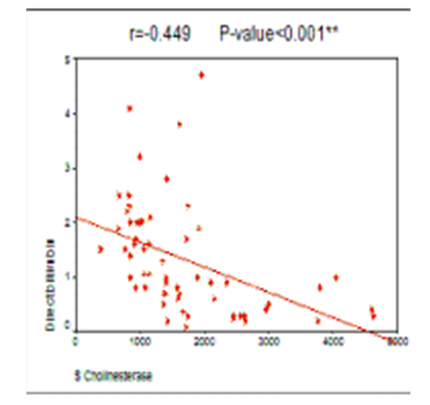 | Figure (4). Correlation between Total bilirubin and serum cholinesterase |
4. Discussion
- Cholinesterases are a group of enzymes that habitually considered in relationship with numerous pathological mechanisms. As acetyl-cholinesterase (AChE) is the enzyme responsible for the inactivation of cholinergic neurotransmission and its up-regulation was considered the main triggering factors for Alzheimer's disease [16], neuromuscular disorders, and tumorigenesis [17]. Serum BChE activity levels have been widely used as a test of liver function and only a few studies, including a low number of patients have assessed cholinesterase levels in human liver, but have not included cirrhotic patients [18].The present study was aimed to use cholinesterase as an another fundamental marker for detecting the liver cirrhosis damaged and severity parallels with the conventional liver diagnosis tests and Child score. The common conventional tests may be abnormal not only in liver dysfunction diseases, but also in illnesses not associated with liver dysfunction, such as non-hepatic disease such as myocardial infarction [19].This paper is considered as a modest contribution to the ongoing discussions about the vital diagnostic role of cholinesterase in the cirrhotic liver. So, particular attention was paid to the evaluation of serum ChE as a biomarker of liver cirrhosis by studying its levels among patients who were with either compensated or decompensated in comparison to healthy volunteers as controls. Additionally, construct the correlation between ChE and other diagnostic markers of liver function such as serum albumin.The present study revealed a significantly lower level of serum ChE among cirrhotic patients than control healthy volunteers according to their Child Score. The data obtained are broadly consistent with Ramachandran et al. [15], who revealed that the main three different grades of liver cirrhosis Child A, Child B, and Child C exposed significantly decreased values of serum cholinesterase. Moreover, the present study also showed that serum cholinesterase was higher in patients with compensated cirrhosis than decompensated cirrhosis patients. These results were matched with the study of Ruchi et al. [20] who concluded that serum cholinesterase can be used as a pivotal marker to distinguish between compensated and decompensated cirrhosis. Furthermore, the present study revealed that the serum levels of ChE were positively correlated with serum albumin levels and negatively with both total and direct bilirubin.Our results supported the fundamental role of ChE and were consistent with Ramachandran et al. [15] results who proved that ChE levels reflect the functional integrity of the liver. Also, serum level of ChE was negatively correlated with prothrombin time and INR as that was previously reported by Meng et al. [10] and Chromy et al. [21] they showed that cirrhotic patients have bleeding diathesis as blood clotting factors reduced in liver dysfunction.Additionally, our results were not consistent with Garcı ́a-Ayllo ́n et al. [18] who observed non-significant changed in the enzyme activity in comparison to controls, but concur with their results in other side, as they detected a significantly increased change in level of protein and mRNA of AChE expression and soluble AChE-R. Therefore, the increase in the level of AChE protein was explained by its association with the decrease in BChE activity in both serum and cirrhotic liver.
5. Conclusions
- Based on the results, it can be concluded that the research into the role of cholinesterase has been very successful in detecting the early stages of liver cirrhosis. So, the findings of our research are quite convincing, and thus the following conclusions can be drawn: 1) the severity of liver damage according to the Child-Pugh score can be detected and diagnosed by the serum level of cholinesterase. 2) the amalgamation of supportive results could be used precisely in appraising the liver function degree. Additionally, Serum cholinesterase is higher in compensated than decompensated cirrhosis.
6. Recommendations
- Serum cholinesterase levels estimation can be used as a routine diagnostic test besides other traditional liver function tests to precisely evaluate the probable grade of liver damage.