-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Clinical Medicine and Diagnostics
p-ISSN: 2163-1433 e-ISSN: 2163-1441
2018; 8(3): 41-44
doi:10.5923/j.cmd.20180803.01

Pulmonary Sequestration which Diagnosed Incidentally after Injury in the Emergency Department
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJong Ha Kim, Jung Ho Kim, Sin Youl Park, Sam Beom Lee, Byung Soo Do
Department of Emergency Medicine, Yeungnam University College of Medicine, Daegu, Korea
Correspondence to: Jung Ho Kim, Department of Emergency Medicine, Yeungnam University College of Medicine, Daegu, Korea.
| Email: |  |
Copyright © 2018 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Pulmonary sequestration (PS) is a congenital lung malformation which supplied from aberrant systemic arteries. It has frequent respiratory complication such as recurrent pneumonia because it is abnormal lung parenchymal anatomy and generally identified by these respiratory symptoms. It is usually diagnosed by three-dimensional reconstruction CT or angiography. We experienced a case of asymptomatic PS which is incidentally diagnosed as mass-like lesion, and then finally confirmed by combination of serial computed tomography imaging without angiography in the emergency department. The patient was discharged without further evaluation. He had no respiratory symptoms, but may have them later and have to consider surgical treatment. We should know that asymptomatic PS may be found in the emergency department and treat appropriately.
Keywords: Congenital lung malformation, Pulmonary sequestration, Emergency department
Cite this paper: Jong Ha Kim, Jung Ho Kim, Sin Youl Park, Sam Beom Lee, Byung Soo Do, Pulmonary Sequestration which Diagnosed Incidentally after Injury in the Emergency Department, Clinical Medicine and Diagnostics, Vol. 8 No. 3, 2018, pp. 41-44. doi: 10.5923/j.cmd.20180803.01.
1. Introduction
- Pulmonary sequestration (PS) is rare structural congenital lung malformation with an estimated incidence of 0.15%-1.8%. [1] It is dysplastic lung tissue supplied by abnormal systemic artery and did not have normal connection with the tracheobronchial tree. [2]PS is divided into extralobar and intralobar type. More than one half of the extralobar type is diagnosed in patients younger than 1 year, which is associated with congenital heart disease, diaphragmatic hernia, and pulmonary hypoplasia. In contrast, more than one half of intralobar type is diagnosed by its pulmonary complications such as cough, fever, hemoptysis or chest pain in later childhood. [3]But asymptomatic patients are difficult to identify and they may live for life time without recognition. So they are diagnosed incidentally as regular health screening or management for other disease. [4]In this case, we diagnosed asymptomatic PS incidentally and also this case was specially diagnosed and finally confirmed by combination of serial computed tomography imaging without angiography in the emergency department.
2. Case Report
- A 38-year-old man visited at emergency department for left chest and left arm pain by mechanical compression due to press machine. His vital signs were stable and any other symptoms were not presented.The analgesic was administered immediately, at the same time blood tests, x-ray and electrocardiography were performed.Blood tests showed mild leukocytosis with a white blood cell count of 13,670/µL, a hemoglobin level of 15.3 g/dL and platelet count of 209,000/µL. The patient’s serum myoglobin level was 523.5 ng/mL and CPK level was 624 IU/L, which were slightly elevated above the normal range. Other test results were in the normal range.Chest x-ray film was taken to check traumatic injury and that shown multiple rib fractures at right 6-8th rib, but evidences of hemothorax and pneumothorax were not seen (Fig. 1). And left shoulder and arm x-ray were not shown gross abnormality.
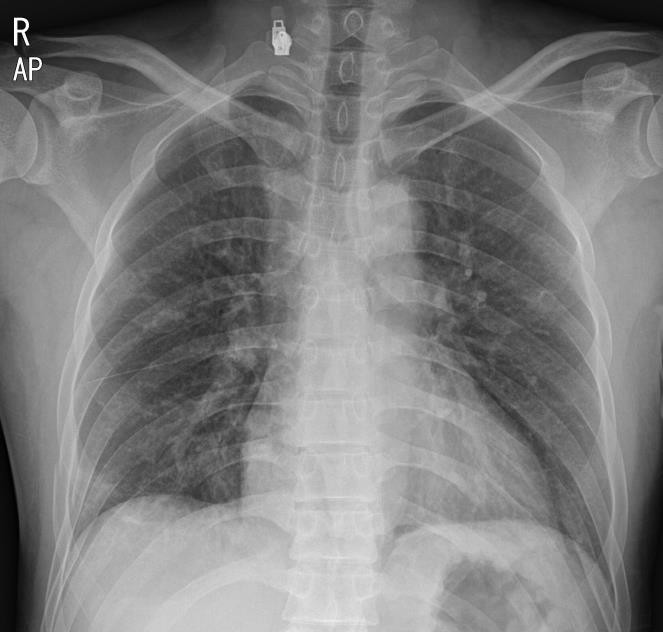 | Figure 1. Simple chest X-ray shows no abnormal mass lesion without multiple rib fractures at right lung field |
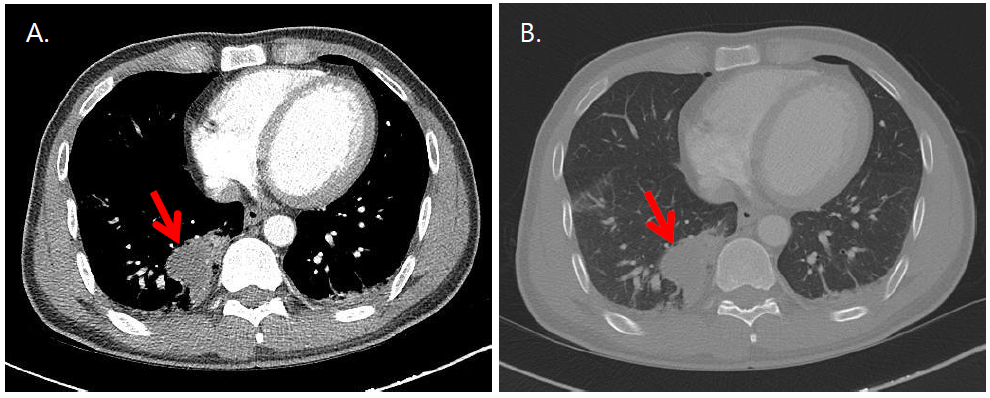 | Figure 2. Chest CT shows a mass-like lesion adjacent to spine at right posterior lung field (arrows indicated). A. enhanced transverse view, B. enhanced lung setting view |
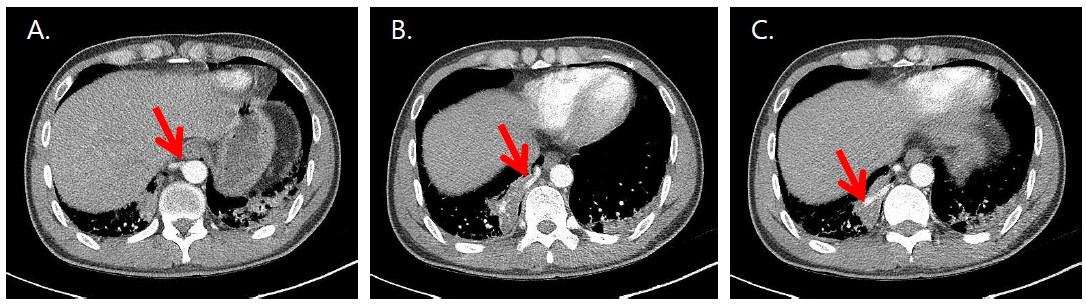 | Figure 3. Serial enhanced transverse chest CT films show a mass-like lesion, it’s blood supply directly from the descending thoracic aorta. (arrows indicated in order to A, B, and C) |
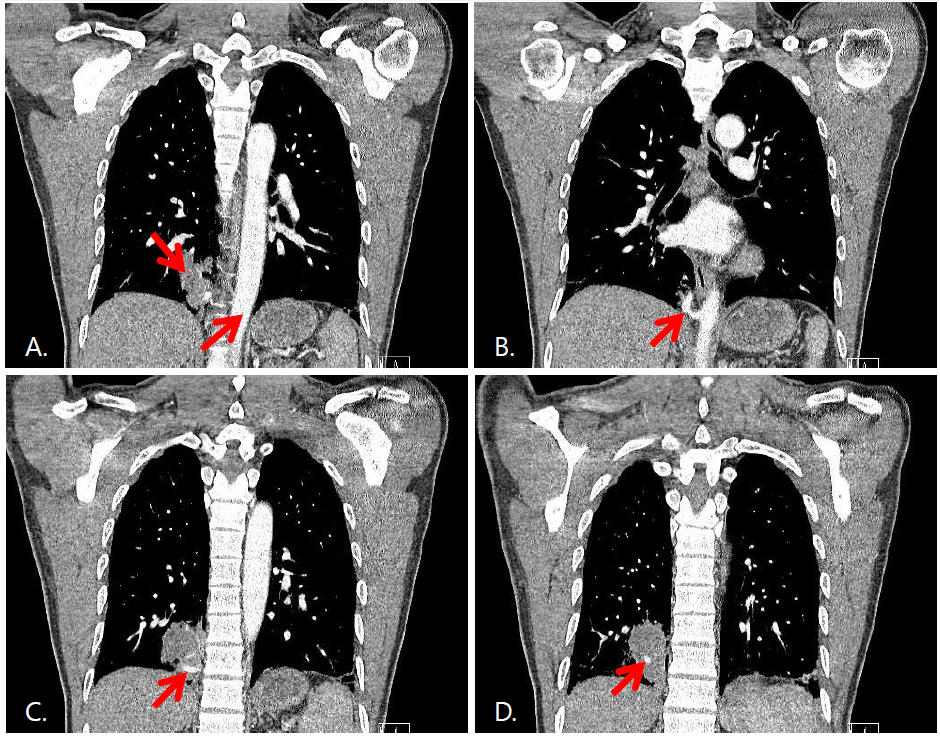 | Figure 4. (A) Enhanced coronal view of chest CT shows a mass-like lesion and the descending thoracic aorta. (B, C, D) Serial enhanced coronal views of chest CT show it’s blood supply directly from the descending thoracic aorta. (arrows indicated in order to B, C, and D) |
3. Discussion
- PS is rare structural congenital lung malformation. It is dysplastic lung tissue supplied by abnormal systemic artery and did not have normal connection with the traheo-broncial tree. [2] In 1777, Huber introduced the first description of the disease, as an accessory pulmonary lobe and Pryce use the term PS and divided by intralobar and extralobar type. [5] Intralobar type is located within the lung and does not have its own visceral pleura but extralobar type is located outside the normal lung tissue and has its own visceral pleura. [1]Generally, PS is located at the lower lobes and intralobar type is 75%-90% of all cases. Three-fifths are of intralobar sequestrations are located the left lower lobe, and two-fifths are located the right lower lobe. Extralobar sequestrations are mostly located the left lower lobe, however about 10% of extralobar sequestrations can be located subdiaphragmatic area. Also it is sometimes positioned on bilateral. [6-8]Most PS is suspicious by symptoms caused by its pulmonary complications such as cough, fever, hemoptysis or chest pain and diagnosed by plain radiography, ultrasound, CT, angiography, and magnetic resonance imaging. Asymptomatic patients are difficult to identification and sometimes, they are diagnosed incidentally. Three-dimensional reconstruction CT can help to detect anomalous vessels and differentiate between intralobar and extralobar type. Angiography is not routine diagnosing method, but the gold standard to determine arterial supply. [9]We could find a lung mass by chest CT. It required a differential diagnosis the cause of bleeding, because it was discovered during trauma evaluation. This case was diagnosed by combination of serial CT imaging but did not taken angiography.Asymptomatic PS does not need surgical treatment at all. If patient does not have any symptoms, we can choose follow-up in out-patient department. If patient present respiratory infectious sign or respiratory distress, we may consider surgical treatment. If there are no contraindications, surgical resection is the standard of treatment for all patients with PS. [10, 11]This case is asymptomatic PS that diagnosed incidentally. Although it was asymptomatic, it can cause respiratory complication later. So if any patient will visit to the emergency department even though disease or trauma, we have to consider PS if abnormal lung mass is seen and check the serial contrast-enhanced computed tomography imaging in the emergency department.