-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Clinical Medicine and Diagnostics
p-ISSN: 2163-1433 e-ISSN: 2163-1441
2018; 8(1): 1-6
doi:10.5923/j.cmd.20180801.01

Quality of Life of Saudi Patients with Dermatologic Disorders
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBassam Ahmed Almutlaq1, Fatemah Kadhem Aljishi2, Rawan Ahmed Gaafar3, Lina Abdulmohsen Alyousif4, Hussain Gadelkarim Ahmed1
1University of Hail, College of Medicine, Saudi Arabia
2Imam Abdulrahman Alfaisal University, Saudi Arabia
3Umm Al-Qura University, Saudi Arabia
4Qassim University, Saudi Arabia
Correspondence to: Hussain Gadelkarim Ahmed, University of Hail, College of Medicine, Saudi Arabia.
| Email: |  |
Copyright © 2018 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: In recent years, an increasing consideration has been given to the impact of dermatologic disorders on the quality of life of dermatology patients. Thus the aim of the present study was to assess the quality of life of Saudi patients with various dermatological conditions in different regions of Saudi Arabia. Methodology: A cross-sectional survey included 756 patients with various dermatologic conditions was conducted. An Arabic online questionnaire from Dermatology Life Quality Index questionnaire was adopted in this study. Data were analyzed by SPSS program version 22. Results: The sample was consisted of 75.8% women and 24.2% men. The major skin problem among patients was Acne (59%). Quality of life was almost good in 61.5% of the studied subjects (21% were not affected at all and 40.5% were slightly affected), while 1.3% of the respondents were largely affected by skin problems. The quality of life of the study group showed statistically significant relation with gender and age (p=0,001 and p=0,020 respectively). Conclusion: The quality of life in studied patients with skin problems, was relatively good. To promote higher quality of life among patients, further studies are recommended.
Keywords: Dermatology, Quality of life, Skin disorders, Saudi Arabia
Cite this paper: Bassam Ahmed Almutlaq, Fatemah Kadhem Aljishi, Rawan Ahmed Gaafar, Lina Abdulmohsen Alyousif, Hussain Gadelkarim Ahmed, Quality of Life of Saudi Patients with Dermatologic Disorders, Clinical Medicine and Diagnostics, Vol. 8 No. 1, 2018, pp. 1-6. doi: 10.5923/j.cmd.20180801.01.
1. Introduction
- Psycho-dermatology focuses on the boundary between psychiatry and dermatology [1]. The skin is the largest and the most visible organ in the body. It is the most important factor determining the appearance of the individual and his/her personal and social perceptions. More than just disfigurement, dermatologic disorders are associated with a variety of psychopathologic problems that can affect the patient [2]. A wide range of skin disorders can theoretically be associated with psychiatric morbidity as a result of their effect upon quality of life and body image of the patient [3]. On average 30-40% of all dermatologic patients also have psychological problems diagnosed by ICD-10 [4]. A recent British Association of Dermatologists’ published the results of a nationwide survey by dermatologists, highlighting the urgent need for (at least) regional psycho-dermatology services. Results found that an overwhelmingly 85% of dermatology patients have indicated that the psychological aspects of their skin disease is a major component of theirillness [5].Many studies were conducted in the context of determining specific psychopathologies associated with different skin disorders. One study has shown that the most frequent psychiatric disorders in skin diseases are depressive and anxiety disorders, with prevalence rates of 20 and 17%, respectively [4]. Another large cross-sectional multicenter study among dermatological out-patients in 13 European countries found a significantly higher prevalence of clinical depression, anxiety disorder, and suicidal ideation among patients with common skin diseases compared with the controls [6]. Regarding the overall effect of skin disorders on the quality of life of patients, psoriasis, chronic urticarial, eczema and acne are among the four dermatological problems which can affect a person self-esteem and quality of life, when prognosis is very poor [7]. Moreover, almost 91% of lichen planus patients had impairment in their dermatological quality of life with majority (62.5%) having moderate to severe impairment [8]. In a study of 217 psoriasis patients with associated depression, 9.7% acknowledged a "wish to be dead," and 5.5% reported active suicidal ideation [2]. Adult patients with atopic dermatitis can have substantial salary loss from missed work, as well as large expenditures for emollients, topical steroids, clothing and bedding, laundry, and possibly consultation with alternative medicine practitioners [9]. These patients are often concerned about personal appearance, attractiveness career aspiration, and the ability to form personal relationships [10]. Impaired sexual function through both physical and psychological mechanisms can compound the adverse effects [9]. Locally, few studies were conducted to assess the quality of life in patients with different dermatological conditions although the depression and anxiety were the most frequent [11]. With regard to Saudi Arabia there is a lack of studies in the context of evaluation of quality of life of patients with dermatologic disorders. One study found that the prevalence of at least one negative emotional state among 300 dermatologic outpatients attending King Abdullah Medical City dermatology outpatient clinic is 24.4% [11]. Therefore, the aim of this study was to assess the quality of life of Saudi patients with various dermatological conditions in different regions of Saudi Arabia.
2. Materials and Methods
- In this cross sectional survey 756 dermatologic patients were randomly included from different regions of Saudi Arabia. The sample was consisted of 183 (24,2%) males and 573 (75,8%) females, aged 18 years old and more.Study tool: An online questionnaire including 15 questions concerning: socio-demographic questions (city, age, gender), the identification of dermatologic issues, and a second part of the questionnaire that evaluate patient’s quality of life and that was adopted from Dermatology Life Quality Index questionnaire. Quality of life in patients with skin disease assessment included 11 questions. The scoring of each question was as follows “Very much” scored 3, “A lot” scored 2, “A little” scored 1, “Not at all” scored 0, “Not relevant” scored 0 and “Question 7, ‘prevented work or studying’” scored 3. For each subject, a maximum score of 30 was calculated. Higher scores reflected more affected quality of life. The calculation of the quality of life scores allowed us to differentiate 5 levels indicated by “No effect at all on patient's life” (0-1), “Small effect on patient's life” (2-5), “Moderate effect on patient's life” (6-10), “Very large effect on patient's life” (11-20) and “Extremely large effect on patient's life” (21-30).Statistical analysis:Statistical package for Social Science (SPSS) program (version 22.0, SPSS Inc, Chicago, IL) was used for data statistical analysis. We used descriptive analysis to determine patient’s socio-demographic characteristics and patient’s skin problems, and to evaluate the quality of life of patients with dermatological conditions. The Chi-squared test allowed us to determine the significance of the relationship between socio-demographic factors and quality of life in patients with skin lesions. P≤ 0.05 was considered as statistically significant.Ethical consent:Each participant was informed about the study and asked to prove his acceptance of contribution.
3. Results
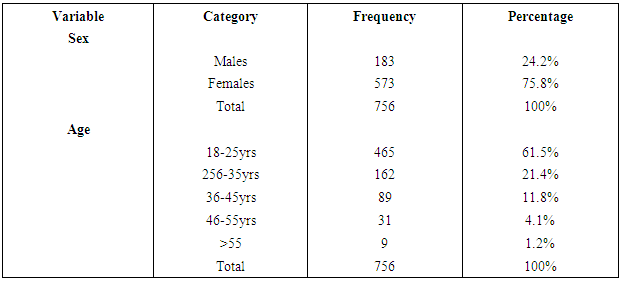
- In the present study a total of 756 patients with dermatological diseases have responded to the questionnaire. Out of 756 patients, 183/756(24.2%) were males and 573/756(75.8%) females, giving males' females' ration of 1.00 to 3.91, as shown in Table 1, Fig 1. The great majority of the study subjects were found in age group 18-25 years representing 465/756(61.5%) followed by age groups 26-35, 36-45, 46-55 and 55+ constituting 162/756(21.4%), 89/756(11.8%), 31/756(4.1%), 9/756(1.2%), as indicated in Table 1, Fig 2.
|
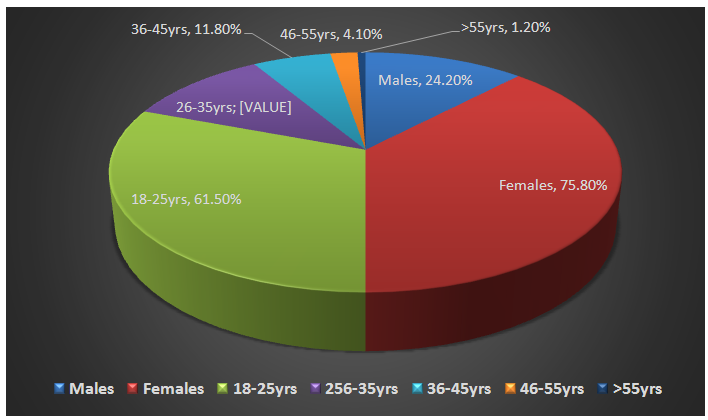 | Figure 1. Distribution of the study subjects by sex and age |
|
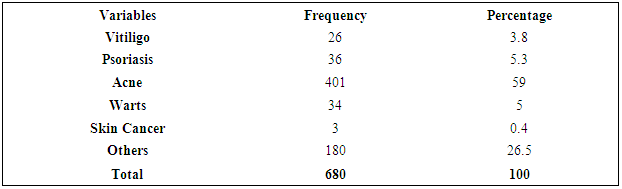
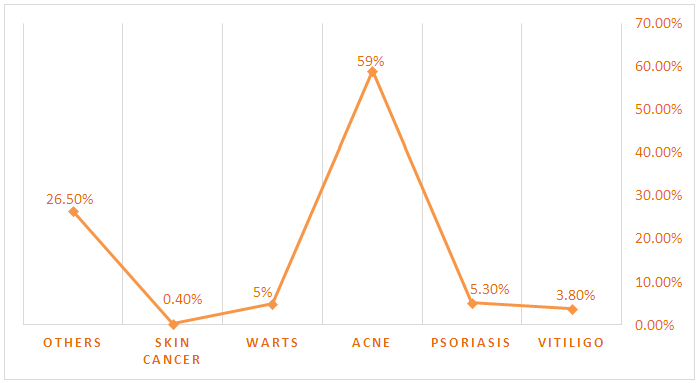 | Figure 2. Description of the study population by dermatological problems |
|
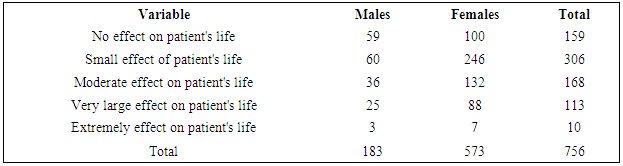
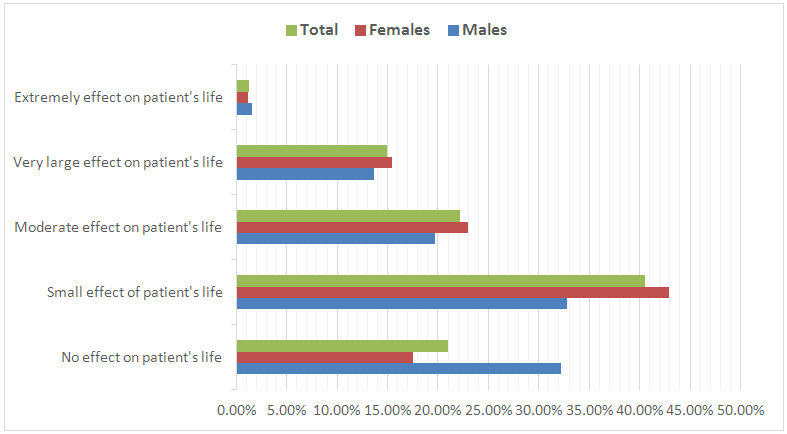 | Figure 3. Description of the study population by sex and life quality measures |
|
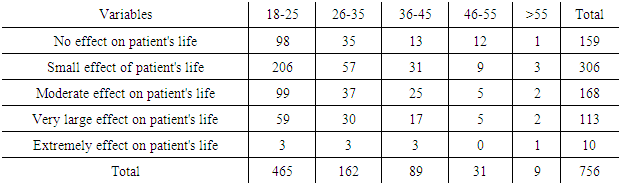
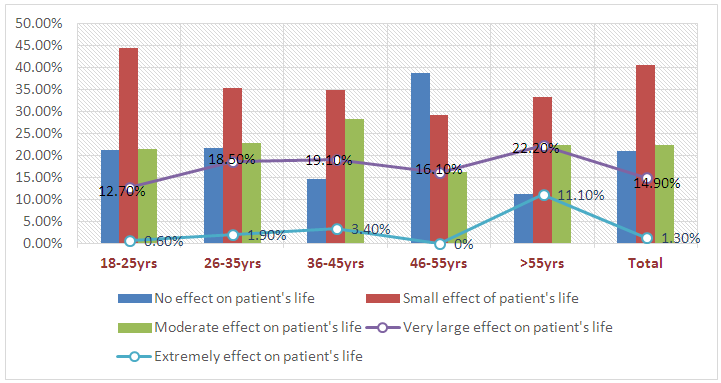 | Figure 4. Description of the study population by age and life quality measures |
4. Discussion
- In the current study, the studied patients with dermatological conditions experienced multitude of symptoms that influenced their quality of life. This work was conducted to evaluate the impact of these symptoms on patient’s quality of life. The most common dermatologic disorder encountered in the present study was Acne. Acne is a common skin condition in adolescents [12]. Acne vulgaris assumes significance in view of its high prevalence and the effect on quality of life of adolescents. Dermatological diseases, among which acne vulgaris, have psychological impact on the affected generating feelings of guilt, shame and social isolation [13]. A reasonable number of Psoriasis as well as vitiligo were also identified in the present study. In general Patients with chronic skin diseases had lower Dermatology Life Quality Index (DLQI), more perceived physical limitations and pain, and lower emotional well-being and general health ratings compared with the control group. However, chronic skin diseases are associated with symptoms of emotional distress, in particular insomnia and general anxiety [14].Generally patients mentioned good quality of life, where 21% had no effect of skin issues on their quality of life, 40.5% were slightly affected and 22.2% were moderately affected, however other patients reported a poor quality of life, where almost 16% had very large to extremely large effect on their life. This fluctuation suggest that patients react variously to critical life experiences. Our study indicates a significant relationship between gender and age, and patient’s quality of life, it shows that women and patients aged between 35 and 45 years old have a tendency to be more irritated by skin health affections. Female gender influence may be explained by women's psychological fragility.Several studies have shown that quality of life impairments correlate with disease severity, aberrant skin bio-physiology, depression, anxiety and stress symptoms. Physicians caring for these patients must evaluate the different but inter-correlated medical, bio-physiological and pertinent psychosocial domains. These significant correlations imply that a holistic approach should encompass psychotherapy, behavioral therapy and coping strategies in conjunction with dermatologic therapy [15].Some skin issues such as psoriasis and acne may be recurrent accentuating the discomfort of patients, thus a strong doctor-patient relationship could establish a trust link and positively influence treatment efficiency. This will encourage patients to be more controlled in taking their medications, as well as leading to better usage compliance and ultimate a better way of life. Some dermatological conditions could be managed and even prevented, even if symptoms could be uncomfortable like itching. Consequently the affected patients should be patient and keeping in mind to adopt preventing strategies that may help improving the disease control and subsequent quality of life. Psychological support may also reduce patient’s frustration and help them to accept their conditions. In fact this will encourages patients to adopt positive thoughts, explore their emotions and seek social sustain instead of seeking social stress.
5. Conclusions
- The findings of the present study demonstrate that, skin issues have an impact on the quality of life of patients. Patients need psychological support in addition to physical care, as this can lead to better outcomes of the treatment and better quality of life.